(UroToday.com) The American Urological Association's 2025 Annual Meeting, in Las Vegas, Nevada, was host to the PD37: Bladder Cancer: Invasive III Session. Dr Arash Samiei presented PD37-01: Improving Risk Prediction in Radical Cystectomy Patients Using Artificial Intelligence Models.
Dr. Samiei began the presentation by emphasizing that surgical complications following radical cystectomy (RC) remain a major challenge for patients and clinicians. As the highest-morbidity procedure in urologic oncology, RC is associated with complication rates approaching 50%—even at high-volume centers. These complications have a substantial impact on patient outcomes, quality of life, and healthcare costs. Hospital readmissions alone add an average of 4 inpatient days and $10,000–$30,000 in additional costs per episode. Dr. Samiei also highlighted the limitations of existing risk prediction models, such as ACS-NSQIP, which often underestimate complication rates and lack the precision needed for real-time, individualized surgical risk assessment.
An unmet need is that we need reliable, procedure-specific risk stratification to inform clinical judgment and improve perioperative outcomes. To address this need, the investigators developed innovative predictive models using artificial intelligence (AI) to identify patients at high risk for complications. These AI models were trained on a large dataset from the National Cancer Database (NCDB) and compared to LR in their ability to predict adverse outcomes after RC. The overarching goal of this study was to equip surgeons with AI-driven tools to enhance decision-making and ultimately improve surgical outcomes.
The investigators selected 24 variables encompassing patient demographics, socioeconomic indicators, staging, pathology, and treatment characteristics. Several artificial intelligence (AI) models, including neural networks, extreme gradient boosting (XGBoost), logistic regression, and random forest were developed and compared to traditional logistic regression. Model performance was evaluated using 10-fold cross-validation, with a focus on area under the curve (AUC) and accuracy as performance metrics.
How AI models workDr. Samiei highlighted that physicians often rely on decision-making grounded in clinical guidelines and individual expertise. In contrast, AI mimics clinical reasoning by learning decision logic from large-scale patient datasets. Rather than following static rules, AI systems refine their predictions through exposure to thousands of real-world cases, offering a data-driven complement to traditional clinical judgment.
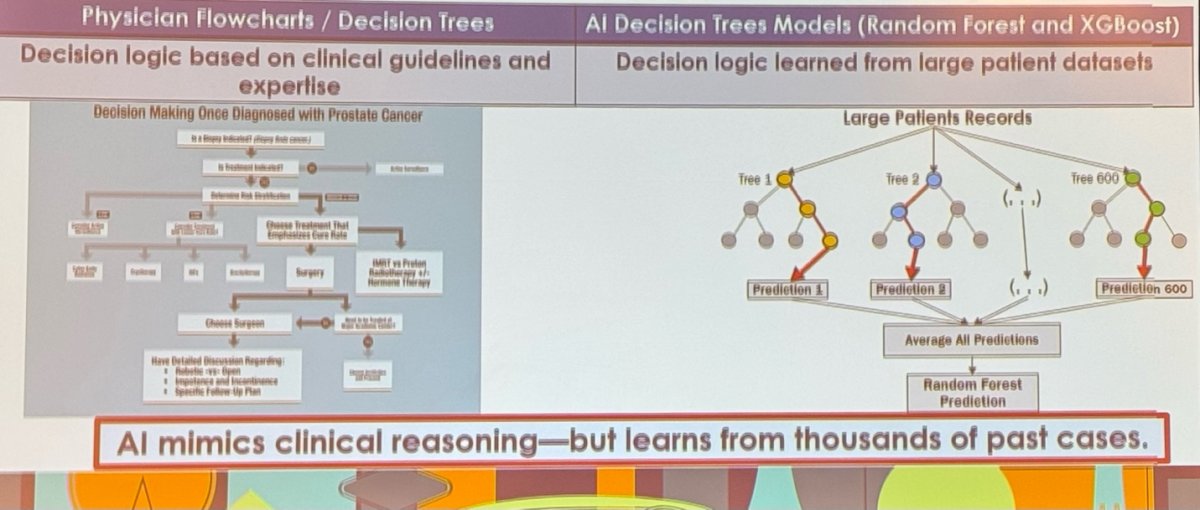
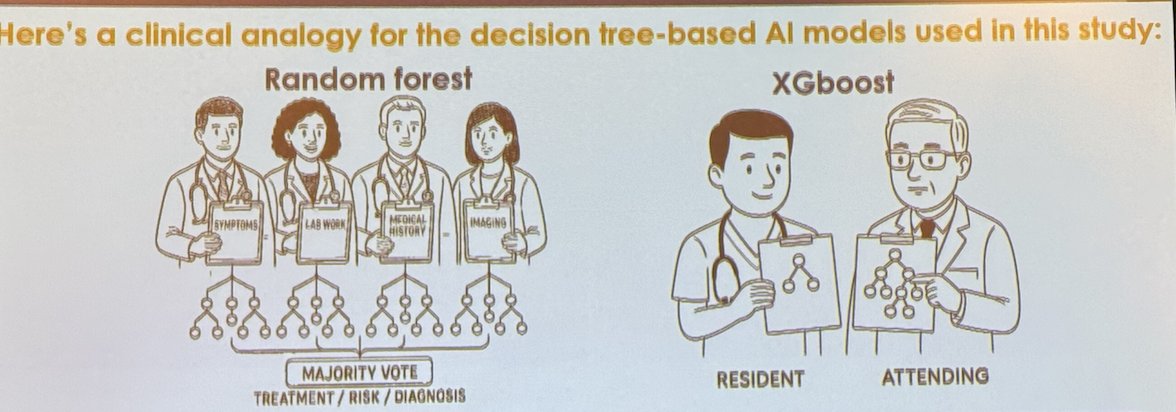
Decision tree–based AI models use branching logic to explore different pathways and identify optimal solutions. Among these, Random Forest models aggregate predictions from multiple decision trees and make final decisions based on a “majority vote”—akin to combining multiple expert opinions. XGBoost, on the other hand, builds sequential trees where each new tree focuses on correcting the errors of the previous one, similar to how an attending physician provides feedback to help a resident improve with each case.
Moreover, physicians intuitively assign different levels of importance or weight to clinical variables when making decisions. AI models aim to replicate this process. Adjusted-weight models, such as logistic regression and neural networks, learn variable importance from large datasets. Logistic regression assigns weights in a linear fashion, offering straightforward interpretability. In contrast, neural networks adjust weights across multiple layers, allowing them to capture complex, non-linear relationships and patterns in the data.
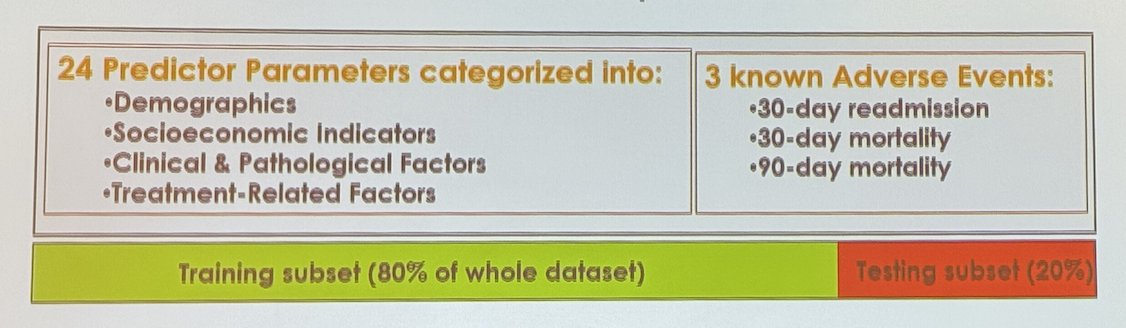
Dr. Samiei and colleagues conducted a retrospective analysis of patients diagnosed with bladder cancer who underwent radical cystectomy between 2004 and 2021, using data from the NCDB. They identified 24 predictor variables categorized into four groups: demographics, socioeconomic indicators, clinical and pathological factors, and treatment-related characteristics. The primary outcomes assessed were 30-day unplanned readmission, 30-day mortality, and 90-day mortality. The dataset was divided into a training subset (80%) and a testing subset (20%) for model development and validation.
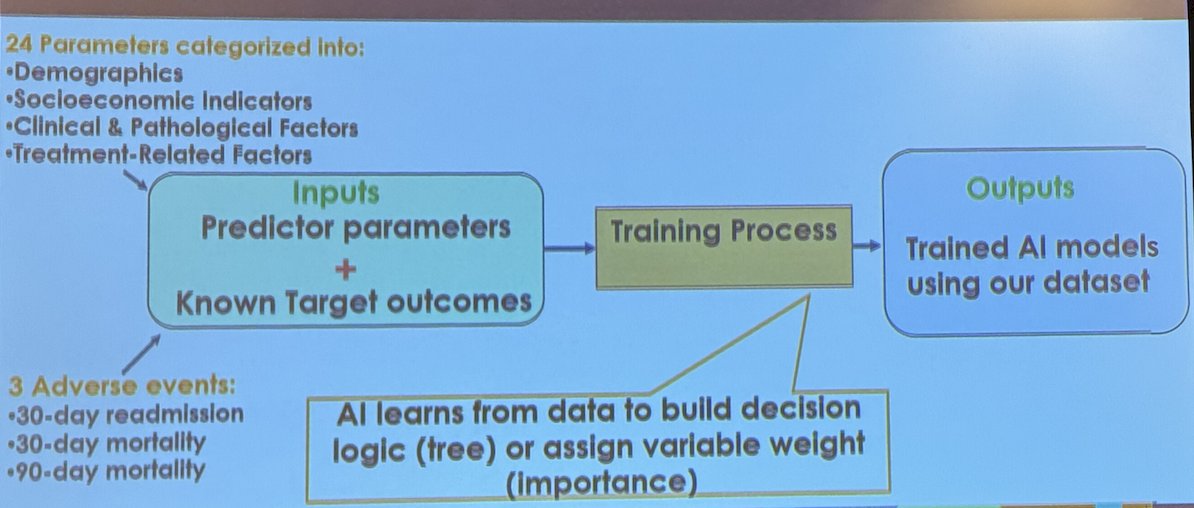
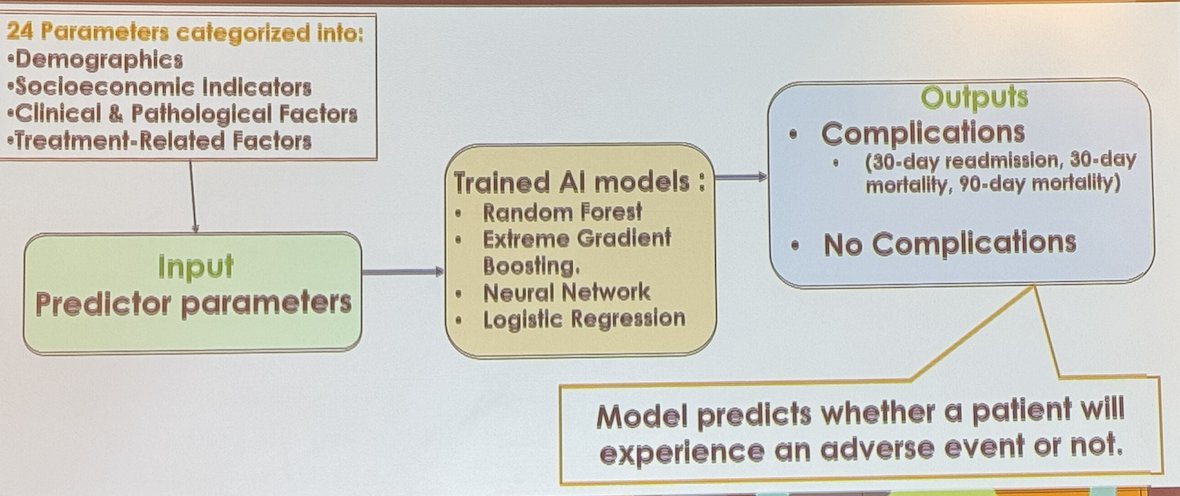
The NCDB cohort included 59,825 patients who underwent radical cystectomy. Below is an illustration of how the models were built and trained using 80% of the dataset. For this training set, the inputs included the selected predictor parameters along with the known target outcomes (e.g., readmission, mortality). These inputs were used to train various AI models. The AI learns from the data by either building decision logic (as in tree-based models) or assigning variable weights (as in logistic regression or neural networks) to optimize prediction accuracy.
Moreover, model evaluation was performed using the remaining 20% of the database (testing set). In this phase, only the predictor parameters were used as inputs, while the model generated outputs predicting whether a patient would experience a complication or not. The goal was to assess the model’s ability to accurately classify patients as likely to experience an adverse event versus those who would not, based solely on their clinical and demographic characteristics.
Model performance was compared using the Area Under the Curve (AUC), which measures how well a model distinguishes between patients who did and did not experience complications. Dr. Samiei noted that among the predictive models tested, XGBoost demonstrated the highest performance with an AUC of 0.801. This was followed by the neural network model (AUC 0.775) and random forest (AUC 0.770). Traditional logistic regression showed the lowest predictive performance, with an AUC of 0.706.
Dr. Samiei concluded the presentation with the following key points:
- Advanced AI models outperformed traditional logistic regression in predicting postoperative complications following radical cystectomy.
- AI-driven preoperative risk assessment may help identify high-risk patients and support personalized surgical planning.
- Ongoing efforts aim to validate and refine these models across external datasets to enhance their clinical utility.
Presented by: Arash Samiei, MD, PGY4-Urology resident at Allegheny Health Network, Pittsburgh, PA.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025