(UroToday.com) The 2025 AUA annual meeting featured the 4th annual IBCG Bladder Cancer Forum evaluating common problems and controversies in bladder cancer, moderated by Dr. Petros Grivas with a debate between Drs. Roger Li and Jonathan Rosenberg are discussing whether we should use ctDNA to guide treatment decisions regarding adjuvant chemotherapy or immunotherapy after radical cystectomy.
Dr. Grivas started the debate with a case presentation of a 72 year old man with hematuria, a medical history notable for hypertension, no known cancers in his family, excellent social support, and a history of smoking 1 pack of cigarettes per day for 20 years. On presentation, imaging showed a filling defect in the lateral bladder wall suspicious for a 6 cm bladder tumor, without lymphadenopathy, hydronephrosis, or distant metastasis. His CT chest was also negative for metastases, eGFR 68 cc/min, ECOG performance status was 1, and he was otherwise a candidate for cisplatin-based chemotherapy. Subsequent TURBT showed a urothelial carcinoma with 40% squamous differentiation, involvement of the muscularis propria, as well as positive for CIS and lymphovascular invasion. The patient was counseled on his options, including neoadjuvant chemotherapy followed by radical cystectomy versus trimodality therapy versus clinical trial enrollment. The patient elected to undergo accelerated MVAC (with G-CSF) x 4 cycles, then restaging to consider radical cystectomy + pelvic lymphadenectomy. He completed chemotherapy with no unexpected or serious adverse events, and post chemotherapy imaging showed only bladder wall thickening with peri-vesical fat stranding, but no lymphadenopathy or distant metastases. He elected for a radical cystectomy, which showed ypT2N0 (+CIS and lymphovascular invasion) urothelial carcinoma with 60% squamous differentiation. Dr. Grivas then polled the audience based on the following question: “Should ctDNA be used to guide adjuvant nivolumab in this setting?” The following were the options available:
- Yes
- Not yet
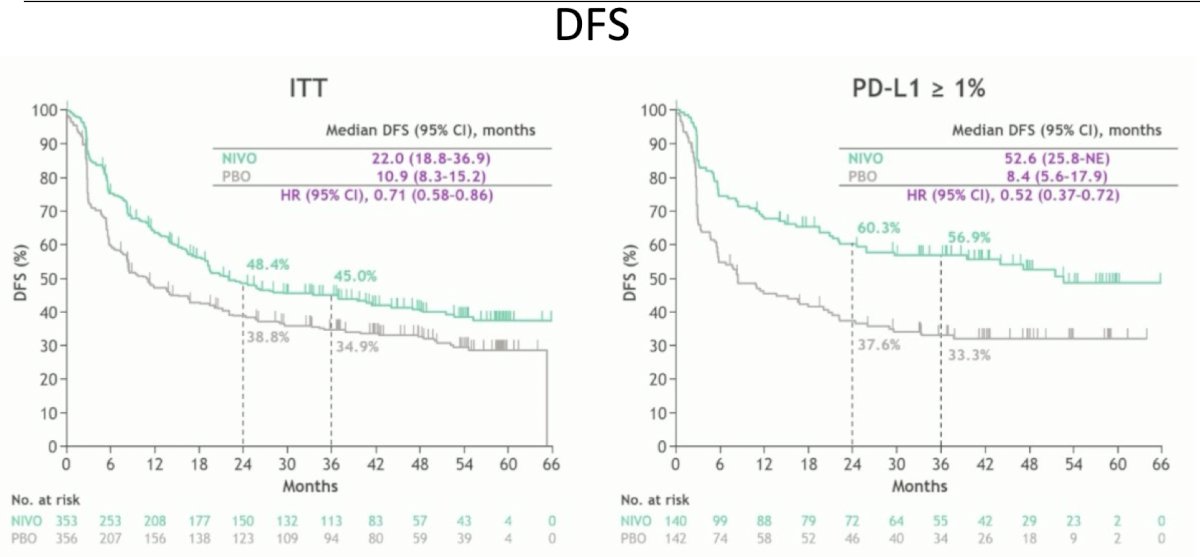
Dr. Li then took the position that yes, ctDNA should be used for guiding the need for adjuvant nivolumab in this setting. From the CheckMate-274 trial1 adjuvant nivolumab is approved based on pathology from the radical cystectomy specimen. In CheckMate-274, patients with high risk disease were randomized to one year of adjuvant nivolumab versus placebo. The co-primary endpoints were disease free survival in the intention to treat population and in the PD-L1 positive population. The first analysis of CheckMate-274 noted an improvement in disease free survival among all patients receiving nivolumab versus placebo in both the intention to treat population, as well as the PD-L1 positive population:
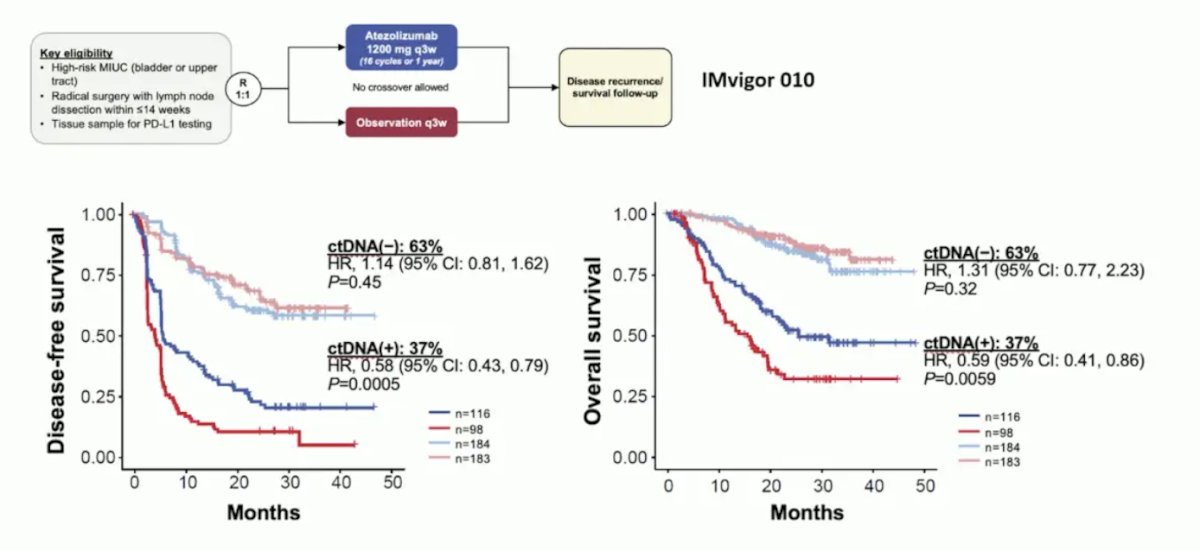
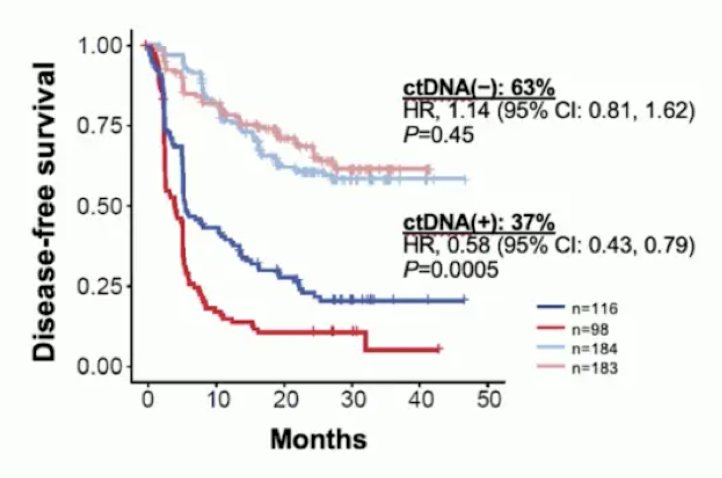
Thus, Dr. Li argues that we have entered into a time of precision medicine, and we should be using ctDNA to guide our management. Next, Dr. Li discussed the seminal analysis of ctDNA that established it as a biomarker in the adjuvant therapy space. From the IMvigor010 trial, Powles et al.1 showed that ctDNA is very prognostic in the adjuvant setting for muscle invasive bladder cancer, particularly in the observation arm for assessing disease free and overall survival:

Additionally, in this same analysis, ctDNA was prognostic for assessing minimal residual disease and correlating with disease free and overall survival:
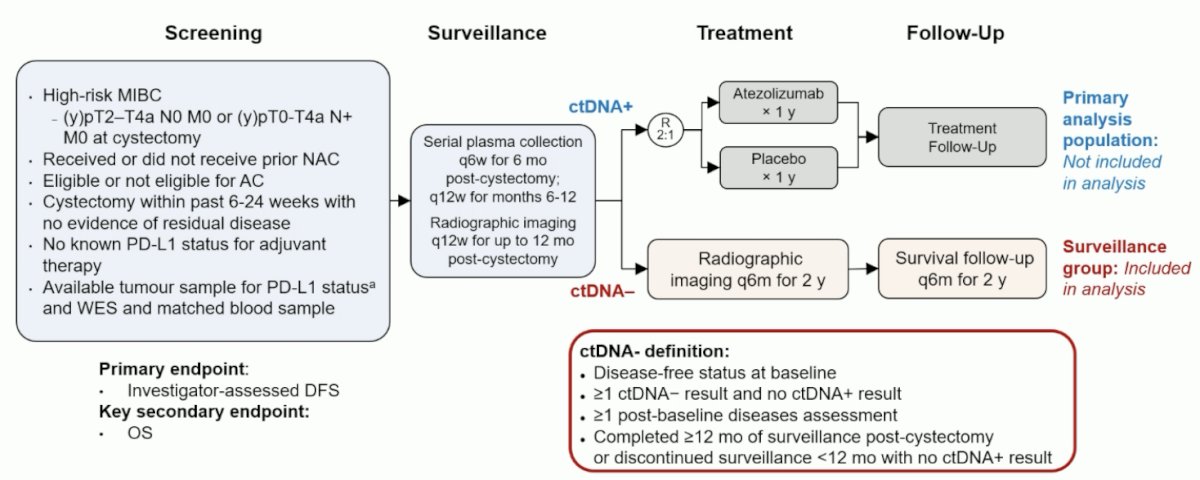
Based on these findings, IMvigor011 has been developed, incorporating ctDNA as a key part of the trial design. IMvigor011 is a global, double-blind, randomized phase III study evaluating the efficacy of atezolizumab versus placebo in patients with high-risk muscle invasive bladder cancer who are ctDNA positive post-cystectomy. The IMvigor011 trial design is as follows:
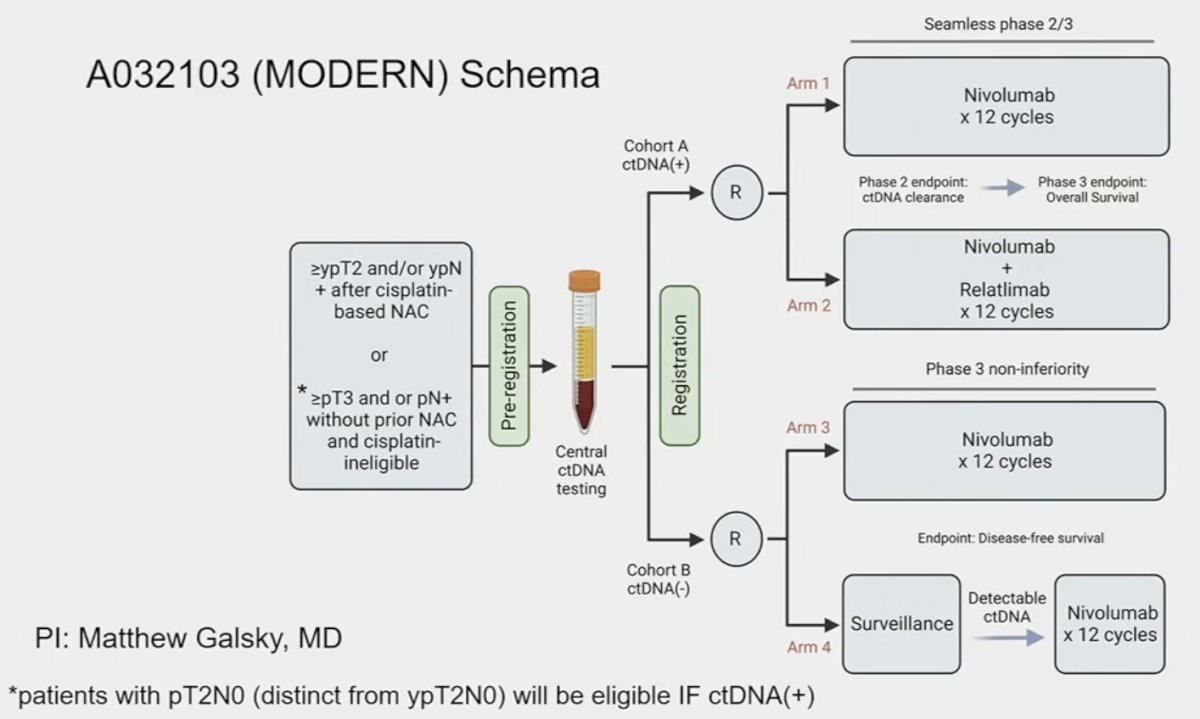
Another important trial in this disease space is the MODERN trial, which is evaluating adjuvant therapy treatment combinations (nivolumab, nivolumab + relatlimab, or surveillance) based on ctDNA status:
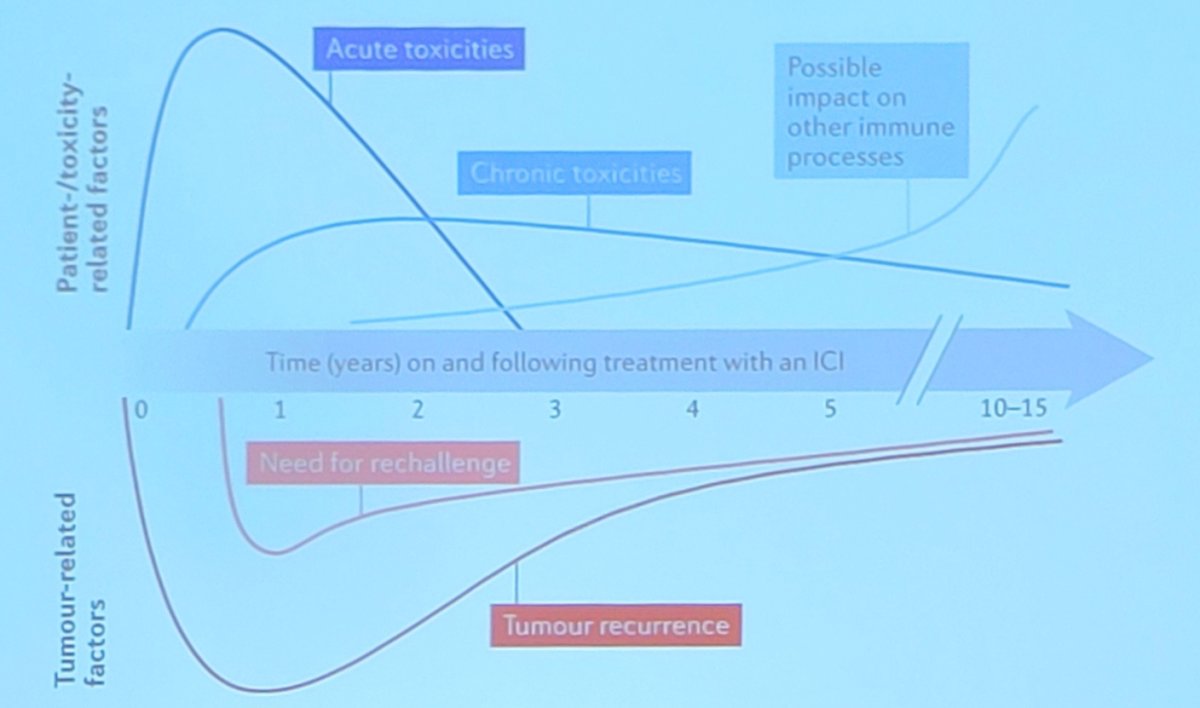
It is important to emphasize that there are potentially substantial toxicities with these therapies, which may have long term consequences:
Dr. Li’s final argument was to make sure we stratify patients correctly for adjuvant nivolumab with ctDNA, given the cost is high ($129,257) per year of treatment. To start off his portion of the debate that perhaps ctDNA is not quite ready for primetime, Dr. Rosenberg highlighted what we currently know about ctDNA:
- ctDNA positivity is prognostic
- Its presence almost always indicates future relapse
- ctDNA negative patients do better, though many still relapse
- ctDNA positive patients seem to benefit from treatment with single agent atezolizumab in a retrospective analysis of a negative trial
- No prospective phase III data exist to tell us whether ctDNA is better than pathologic staging to make decisions in the adjuvant setting
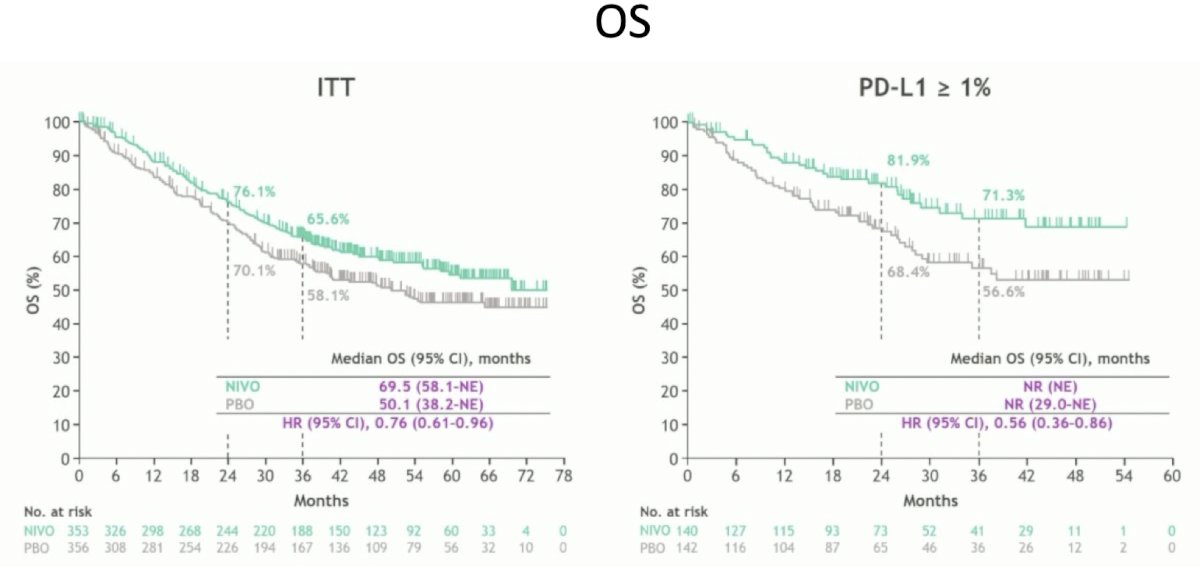
As mentioned earlier by Dr. Li, adjuvant nivolumab demonstrated a disease free survival benefit among high risk patients after radical cystectomy,1 and in a subsequent analysis Dr. Matt Galsky showed an improvement in overall survival in those who received nivolumab. Thus, this was the first trial of adjuvant immunotherapy that showed an improvement in overall survival:3
With regards to the ctDNA analysis from IMvigor010,2 Dr. Rosenberg cautions that over 30% of patients who are ctDNA negative will eventually still relapse:
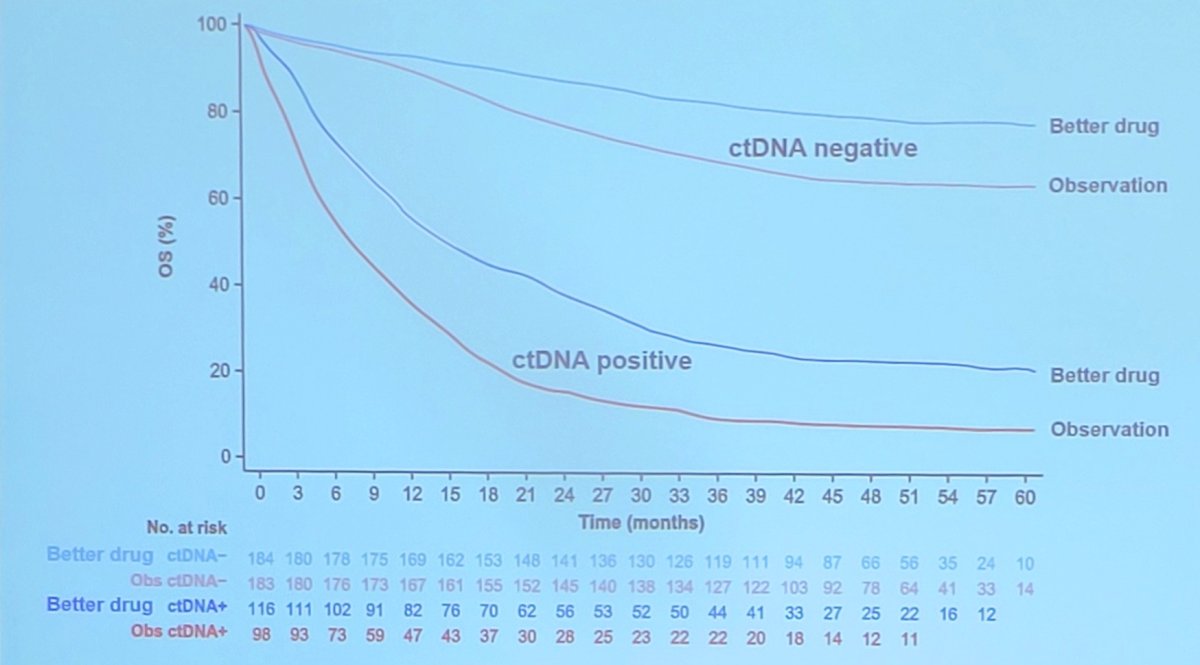
So, what if the problem is the drug, not the ctDNA status? ctDNA is prognostic, but a better therapy may show benefit regardless of ctDNA status. Moreover, ctDNA negative patients may still benefit from treatment with an active agent, and IMvigor011 won’t help us with this question. Thus, more additional prospective data is needed, with the following basic analysis design proposed by Dr. Rosenberg:
Importantly, MODERN will start to answer the important questions of whether this is a predictive biomarker. Dr. Rosenberg concluded his portion of the debate by highlighting what we need to know for proper implementation of ctDNA testing:
- Prospective data is required to understand whether ctDNA negative patients benefit at all, although retrospective data from CheckMate-274 and AMBASSADOR4 would be helpful as well
- Can treatment at seroconversion lead to similar outcomes? This will be answered with the MODERN trial
- Can we safely forgo treatment in high risk ctDNA negative patients? This will be answered with the MODERN and IMvigor011 trials
- ctDNA is not (yet) ready for primetime to select patients for adjuvant therapy
- We need to encourage enrolment in the MODERN trial to answer these questions
- Based on CheckMate-274, this patient should receive adjuvant nivolumab
The debate concluded by highlighting the pre- and post-debate answers to the polling question “Should ctDNA be used to guide adjuvant nivolumab in this setting?”
- Yes
- Pre-debate: 54%
- Post-debate: 46%
- Not yet
- Pre-debate: 46%
- Post-debate: 54%
Presented by:
- Roger Li, MD, Moffitt Cancer Center, Tampa, FL
- Jonathan Rosenberg, MD, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
Related content: ctDNA in Bladder Cancer: Prognostic Value and Ongoing Clinical Trials - Jonathan Rosenberg & Petros Grivas
References:
- Bajorin DF, Witjes JA, Gschwend JE, et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. 2021 Jun 3;384(22):2102-2114.
- Powles T, Assaf ZJ, Davarpanah N, et al. ctDNA guiding adjuvant immunotherapy in urothelial carcinoma. Nature. 2021 Jl;595(7867):432-437.
- Galsky MD, Witjes JA, Gschwend JE, et al. Adjuvant nivolumab in high-risk muscle-invasive urothelial carcinoma: Expanded efficacy from CheckMate 274. J Clin Oncol. 2025 Jan;43(1):15-21.
- Apolo AB, Ballman KV, Sonpavde G, et al. Adjuvant pembrolizumab versus observation in muscle-invasive urothelial carcinoma. N Engl J Med. 2025 Jan 2;392(1):45-55.