(UroToday.com) The American Urological Association (AUA) 2025 Annual Meeting, held in Las Vegas, was host to a bladder cancer clinical trials in progress session. Dr. Francesco Del Giudice presented the ongoing CUT-less randomized trial comparing MRI (VI-RADS) followed by photodynamic-guided transurethral resection versus white light conventional and second resection in non-muscle invasive bladder cancer (NMIBC) patients.
The initial surgical management of both non-muscle and muscle invasive bladder cancer (MIBC) remains a TURBT. However, an incomplete tumor resection may occur in 33–76% of cases. Furthermore, underestimation of tumour depth of invasion at first TURBT (i.e., understaging) has been demonstrated in 7–30% of cases, increasing up to 45–51% in those with T1 tumours without detrusor muscle present in the resection specimen. Accordingly, restaging TURBT is guideline-recommended for select patients with HG Ta and all T1 tumors to ensure completeness of resection and minimize the risk of disease understaging. However, Dr. Del Giudice argued that there are several drawbacks to this approach:
- Significant detriments to the patient's quality of life (e.g., second hospitalisation, potential risk of complications, delay in definitive treatment, etc.)
- Additional negative social implications (e.g., productivity loss, indirect costs, etc.).
- Increased healthcare-related costs (e.g., surgical procedure costs, in-hospital recovery costs, postoperative care etc.)
The VI-RADS scoring system was developed to standardize the imaging and reporting of bladder cancer and to evaluate the likelihood of muscle-invasive disease. This scoring system leverages the high contrast resolution of MRI, allowing for an excellent differentiation of bladder wall layers. A 5-point scale is utilized as follows:
- Muscle invasion is highly likely
- Muscle invasion is unlikely to be present
- Muscle invasion is equivocal
- Muscle invasion is likely to be present
- Invasion of muscle and beyond the bladder is highly likely
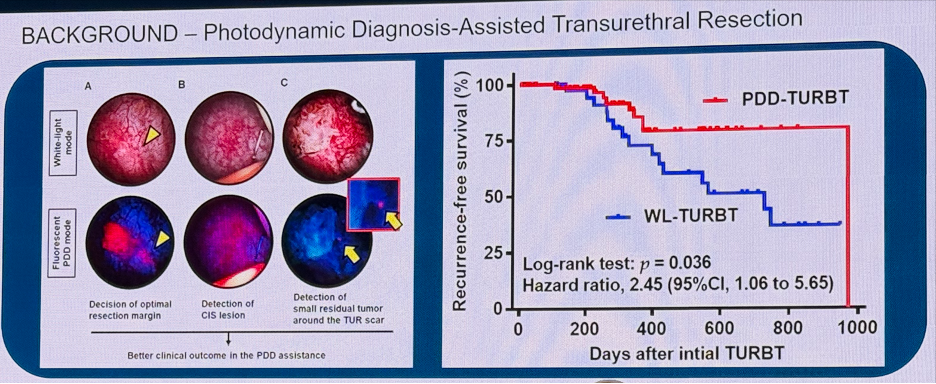
To this end, Dr. Del Giudice and colleagues hypothesized that combining PDD-guided TURBT with the VI-RADS scoring system may allow for the selection of NMIBC patients that may safely forego a re-staging TURBT. CUT-less is an Italian single center, open-label, non-inferiority, phase IV trial whereby patients with primary or recurrent NMIBC undergo a multiparametric MRI with a VI-RADS assessment. Patients with VI-RADS 1–2 findings are subsequently randomized 1:1 to:
- Experimental arm: TURBT with PDD with no restaging TURBT performed for patients with findings of LG T1, HG T1, and HG Ta without detrusor muscle present
- Patients with MIBC, LG Ta, or HG Ta with detrusor muscle present at the PDD-guided TURBT are excluded
- Standard of care arm: Conventional, white light-guided TURBT following which patients with LG T1, HG T1, and HG Ta without detrusor muscle present proceed to a white light-guided re-staging TURBT 2-6 weeks after the initial TURBT
- Patients in both arms subsequently receive induction followed by maintenance BCG
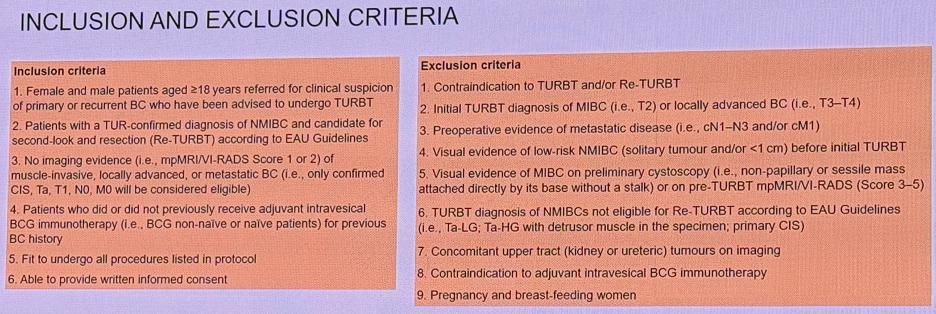
The study inclusion/exclusion criteria are summarized below. The key eligibility criteria are as follows:
- Contraindications to TURBT and/or re-staging TURBT
- Findings of cT2-4 disease on initial TURBT or cN1-3 and/or cM1 disease on staging scans
- Visual evidence of low-risk NMIBC (solitary tumor and/or <1 cm) before initial TURBT
- High likelihood of MIBC on preliminary cystoscopy or mpMRI (VI-RADS score 3-5)
- Concomitant upper tract tumors
- Contraindications to adjuvant intravesical BCG immunotherapy
The primary endpoint was the proportion of early bladder cancer recurrences (i.e., within 4.5 months follow-up) in those patients with NMIBC treated using a standard of care approach, compared to the experimental arm. Secondary endpoints include:
- Proportion of late bladder cancer recurrences (i.e., after 4.5 months follow-up)
- Proportion of patients that progress from NMIBC to MIBC
- Changes in health-related QoL outcomes
- Within-trial cost-benefit analysis to calculate the incremental cost per restaging TURBT avoided and the cost-utility of the experimental arm approach as measured by the incremental cost per quality-adjusted life year (QALY) gained at 2 years and over the patients' lifetime
Dr. Del Giudice concluded his presentation with the following take home messages:
- VI-RADS alone will not replace surgery. The future is translational and multidisciplinary:
- VI-RADS score 1-2 + intraoperative PDD → Skip res-staging TURBT by re-defining the EAU selection criteria
- VI-RADS score 4-5 and sampling TURBT or cytology → Immediate radical cystectomy
- VI-RADS score 3 must improve → currently it is negatively affecting both NMIBC and MIBC pathways
- Increased adoption of the VI-RADS scoring system may lead to health economic benefits in the care of bladder cancer patients
Presented by: Francesco Del Giudice, MD, PhD, FEBU, Assistant Professor of Urology at the Department of Maternal Infant and Urologic Sciences, Sapienza University, Rome, Italy
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
Related content: CUT-less Trial Aims to Eliminate Secondary TURBT in Non-Muscle Invasive Bladder Cancer - Francesco Del Giudice