(UroToday.com) The 2025 AUA annual meeting featured the 4th annual IBCG Bladder Cancer Forum evaluating common problems and controversies in bladder cancer, moderated by Dr. Neha Vapiwala with a debate between Drs. Kent Mouw and Bogdana Schmidt are discussing whether trimodality therapy is a valid option for all of our patients with muscle invasive bladder cancer. Dr. Vapiwala started with a case presentation of a 67 year old male with no significant comorbidities who presented with painless gross hematuria. Cystoscopy showed a unifocal, 3 cm mass in the right anterior wall of the bladder, and pathology demonstrated high grade urothelial carcinoma with focal squamous differentiation invading the muscle. Post-cystoscopy imaging noted a right lateral anterior bladder mass demonstrating hyper-enhancement and deep bladder wall involvement, consistent with invasive bladder cancer. There was also minimal perivesical anterior stranding that may be related to tumor infiltration or possibly reflects inflammation due to a recent intervention. Dr. Vapiwala then polled the audience based on the following question: “Which of these is the top (most important) reason why you would NOT recommend trimodality therapy for your patient?”. The following were the options available:
- T3/T4 tumor
- Hydronephrosis
- Poor baseline bladder function
- Concern for trimodality therapy toxicity
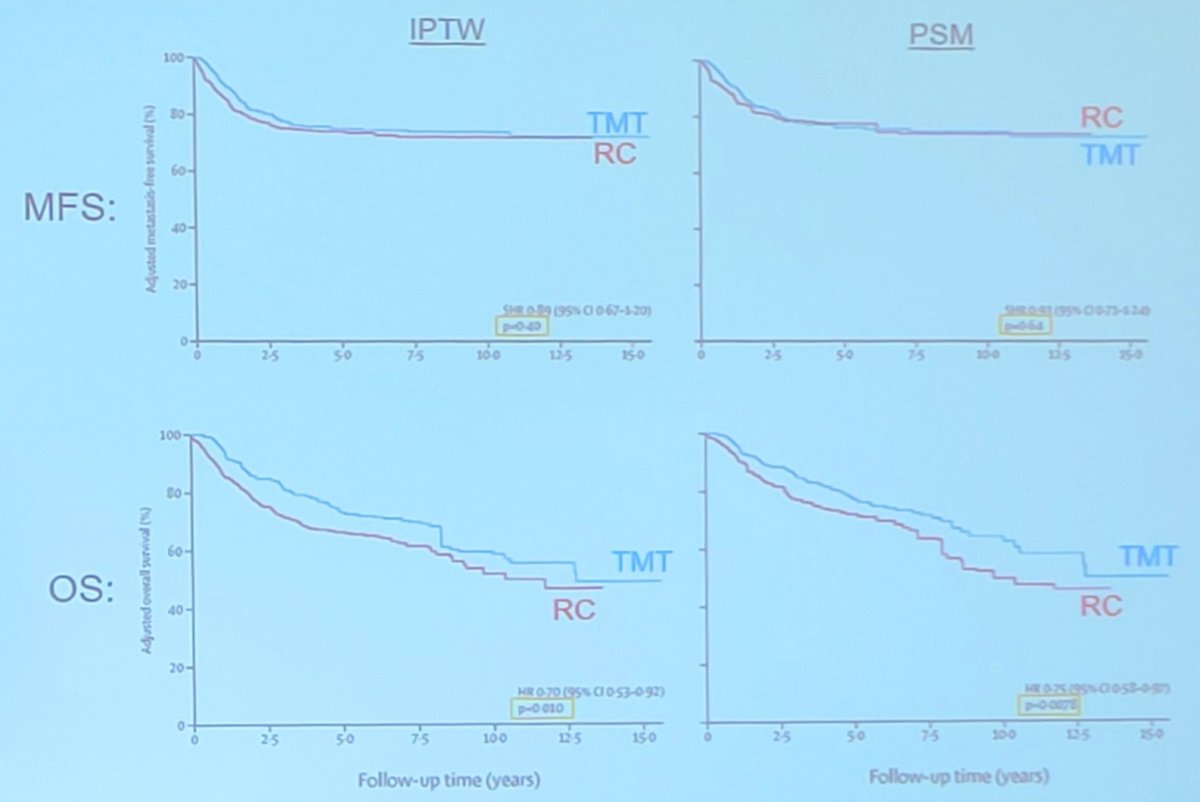
Dr. Kent Mouw then took the position that trimodality therapy is a great option for many patients with muscle invasive bladder cancer. Arguably, the best data outside of a randomized clinical trial comes from a high-level propensity matched score matched multi-institutional (Toronto, MGH, USC) study assessing radical cystectomy versus trimodality therapy in highly selected patients.1 This retrospective analysis included 703 patients with muscle invasive bladder cancer clinical stage T2-T3/4aN0M0. Specifically, there were 421 radical cystectomy patients and 282 trimodality therapy patients who would have been eligible for either trimodality therapy or radical cystectomy (2005-2017). To compare homogeneous cohorts, all patients included in this analysis had solitary tumors <7 cm, no or unilateral hydronephrosis, and no extensive carcinoma in situ. Treatment propensity scores were estimated using logistic regression, and patients were matched 3:1 with replacement and a caliper of 0.25. Covariates included age, sex, clinical T stage (cT2 vs cT3-4), hydronephrosis, (neo)adjuvant chemotherapy, body mass index, smoking history, and ECOG status. Overall survival was estimated with adjusted Cox models, and cancer-specific survival, distant failure-free survival, regional failure-free survival, and metastasis-free survival (combined distant and pelvic nodal failure) were estimated with adjusted competing risk models.
The 3:1 matched cohort comprised 1,116 patients (834 radical cystectomy versus 282 trimodality therapy). After matching, age (71.3 versus 71.6 years), cT2 clinical stage (88 versus 90%), presence of hydronephrosis (12 versus 10%), and use of (neo)adjuvant chemotherapy (60 versus 56%) were similar between radical cystectomy and trimodality therapy cohorts. At 5 years, there was no difference in metastasis-free survival using both IPTW and propensity score matching, with overall survival slightly favoring trimodality therapy:
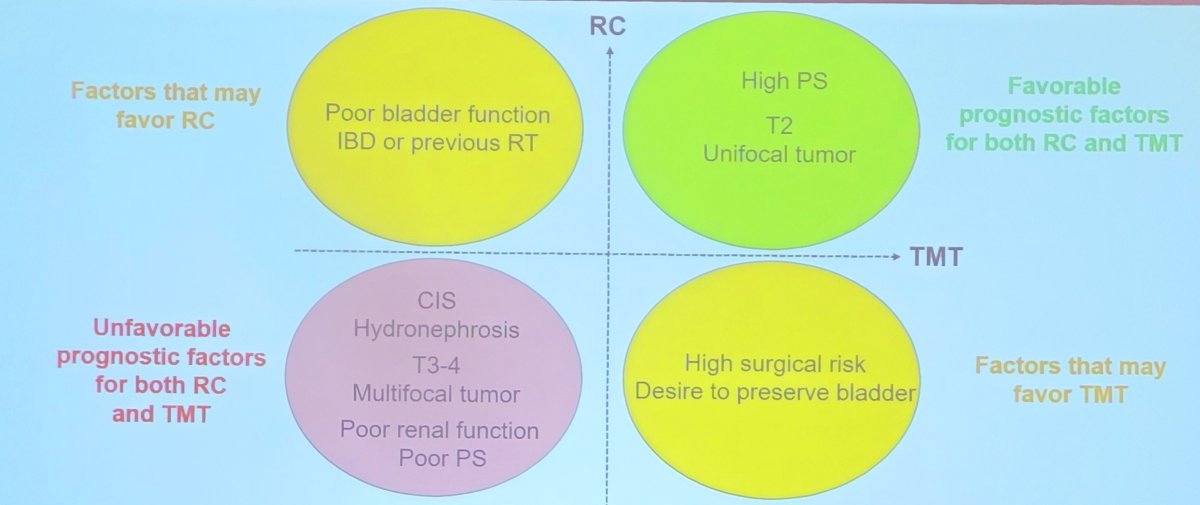
Dr. Mouw emphasized that the characteristics that confer a poor outcome with trimodality therapy are also those that are associated with poor outcomes with radical cystectomy, as highlighted below:
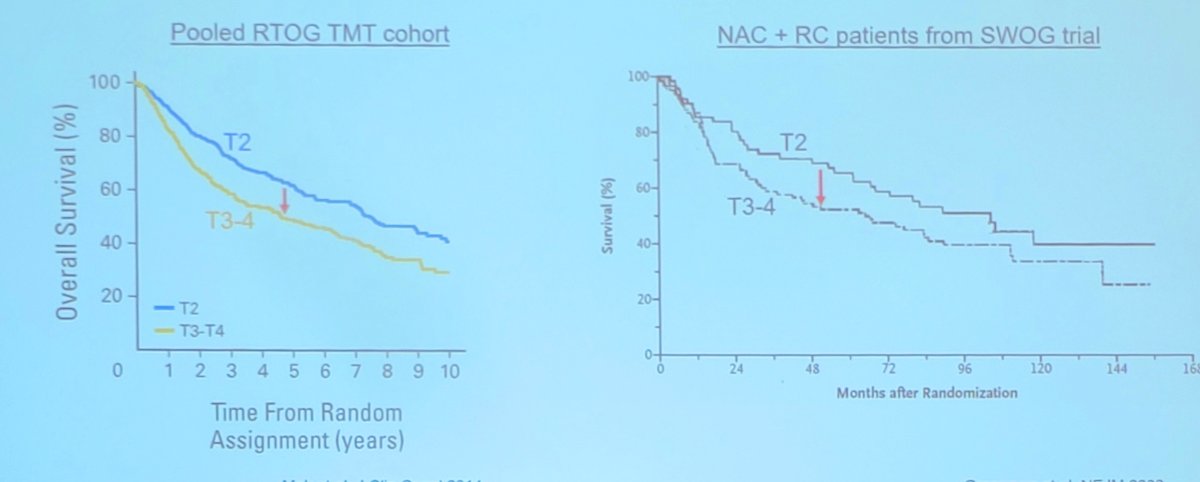
This is further seen when comparing a pooled RTOG trimodality therapy cohort2 and the SWOG neoadjuvant chemotherapy followed by radical cystectomy randomized clinical trial:3
Dr. Mouw also noted that safety and patient related quality of life support trimodality therapy. Generally, the cystectomy rate in large series for trimodality therapy toxicity is 1-2%, and the lifetime risk of dying from a radiation therapy induced pelvic cancer is less than the 90 day risk of death following a radical cystectomy. Using validated patient reported quality of life instruments, trimodality therapy patients report (compared to radical cystectomy):
- Similar bowel and bladder scores
- Better sexual function
- Better informed decision making
- Less life interference
Dr. Mouw concluded his presentation discussing trimodality therapy for this patient with muscle invasive bladder cancer with the following take home messages:
- There is no need to pause treatment for mid-radiotherapy response assessment
- A 4 week radiotherapy course is as good (or better) than a 7 week radiotherapy course, with a 2 week course of treatment currently being tested
- Multiple chemotherapy regimens are supported by strong data (cisplatin, 5FU/mitomycin C, gemcitabine)
- There is a potential role for concurrent/adjuvant immunotherapy
- This is a great opportunity for multi-disciplinary management (diagnosis, treatment, surveillance)
Dr. Schmidt then made the argument that radical cystectomy is still the gold standard treatment for muscle invasive bladder cancer. Because Dr. Mouw reported all of the benefits of trimodality therapy, she started her discussion by assessing what we really know about trimodality therapy. To further analyze this, Dr. Schmidt discussed the patient reported outcomes of the SPARE trial, a randomized feasibility study of selective bladder preservation versus radical cystectomy.4 There are several notable points we learned from this trial:
- It is hard to randomize patients to radical cystectomy versus bladder sparing
- It took 30 months to randomize 45 patients
- Non-compliance was frequent: 24% of patients randomized to radical cystectomy received radiotherapy
- Long term bladder preservation rate was 11/15 (73%) in those who received radiotherapy per protocol
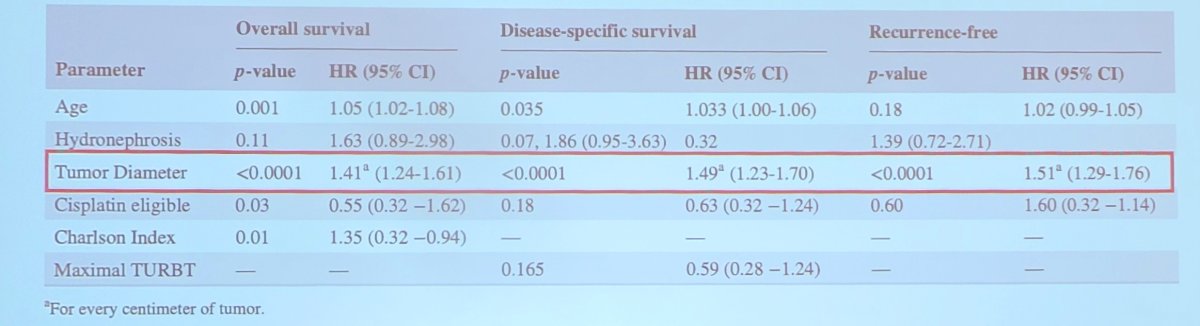
Thus, the conclusion from SPARE is that a randomized trial comparing radical cystectomy versus bladder sparing after neoadjuvant chemotherapy is not feasible. Based on this, Dr. Schmidt emphasized that we cannot keep saying we need more data, because more data is not coming. When we look at the specific data we have, size matters. In a publication from Gofrit et al.5 assessing how to select the best candidates for trimodality therapy, tumor diameter was associated with worse overall survival, disease specific survival, and recurrence free survival:
Location is also important, as noted in the RTOG 88-02 trial, whereby hydronephrosis was the only analyzed factor to be significantly associated with the probability of distant metastases and death. Moreover, in the RTOG 89-03 trial, complete response rates with and without hydronephrosis were 38% (overall survival 33%) versus 64% (overall survival 54%), respectively. Multifocality is also important, which is a significant risk factor for recurrence, as well as the quality of TURBT. Among patients who have resection of all visible tumor, a complete response rate of 79% is achievable versus 57% in those with incomplete resection of tumors.
The bottom line, according to Dr. Schmidt, is that up to 30-40% of patients can experience local recurrence or progression of disease. Although safe, cystectomy is more challenging if trimodality therapy fails. Additionally, clinical staging can miss extravesical or nodal disease, and we may also miss micro-metastases, leading to undertreatment. Ultimately, oncological outcomes show comparable survival for trimodality therapy versus radical cystectomy in highly selected patients only.
Dr. Schmidt concluded her presentation arguing against trimodality therapy for all patients, with the following take home points:
- There is no one size fits all: trimodality therapy can be effective in a minority of well-selected muscle invasive bladder cancer patients with small, unifocal tumors, without hydronephrosis and complete TURBT
- Radical cystectomy is still the gold standard for most patients
The debate concluded by highlighting the pre- and post-debate answers to the polling question “Which of these is the top (most important) reason why you would NOT recommend trimodality therapy for your patient?”
- T3/T4 tumor
- Pre-debate: 30%
- Post-debate: 20%
- Hydronephrosis
- Pre-debate: 13%
- Post-debate: 20%
- Poor baseline bladder function
- Pre-debate: 50%
- Post-debate: 57%
- Concern for trimodality therapy toxicity
- Pre-debate: 7%
- Post-debate: 3%
Presented by:
- Kent Mouw, MD, PhD, Dana Farber Cancer Institute/Brigham and Women’s Hospital, Boston, MA
- Bogdana Schmidt, MD, PhD, University of Utah, Salt Lake City, UT
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
Related content: Cystectomy vs. Bladder Preservation: Weighing Options for Muscle-Invasive Bladder Cancer - Bogdana Schmidt & Kent Mouw
References:
- Zlotta AR, Ballas LK, Niemierko A, et al. Radical cystectomy versus trimodality therapy for muscle-invasive bladder cancer: A multi-institutional propensity score matched and weighted analysis. Lancet Oncol. 2023 Jun;24(6):669-681.
- Mak RH, Hunt D, Shipley WU, et al. Long-term outcomes in patients with muscle-invasive bladder cancer after selective bladder-preserving combined-modality therapy: A pooled analysis of Radiation Therapy Oncology Group protocols 8802, 8903, 9506, 9706, 9906, and 0233. J Clin Oncol. 2014 Dec 1;32(34):3801-3809.
- Grossman HB, Natale RB, Tangen CM, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med 2003;349(9):859-866.
- Huddart RA, Birtle A, Maynard L, et al. Clinical and patient-reported outcomes of SPARE—A randomized feasibility study of selective bladder preservation versus radical cystectomy. BJU Int. 2017 Nov;120(5):639-650.
- Gofrit ON, Meirovitz A, Frank S, et al. Trimodality therapy in T2-4aN0M0 bladder cancer –How to select the best candidate? Cancer Med. 2020 Nov;9(22):8491-8497.