(UroToday.com) The 2025 AUA annual meeting featured the IBCG Bladder Cancer Forum evaluating common problems and controversies in bladder cancer, moderated by Dr. Wei Shen Tan, with a debate between Drs. Laura Bukavina and Morgan Roupret are discussing active surveillance for low-grade intermediate risk bladder cancer. Dr. Tan started with a case presentation of a 75 year old male with an ECOG performance status of 1 and a medical history significant for a previous myocardial infarction (2000), type 2 diabetes mellitus, a cerebrovascular accident (2020), and COPD. He is a current smoker and is on 81 mg of aspirin and Plavix. He was initially diagnosed in March 2022 with a 3 cm tumor, he underwent a TURBT followed by a single postoperative dose of gemcitabine, with pathology notably for low grade Ta urothelial carcinoma (ie. low grade intermediate risk disease). In June 2024, he had a follow-up TURBT for two 1 cm tumors that were both low grade Ta tumors for which he received 6 weekly cycles of gemcitabine. Dr. Tan then polled the audience based on the following question: “What treatment option would you select?”. The following were the options available:
- TURBT
- Active surveillance
- Chemoablation
- Office fulguration
- Other
Dr. Roupret then discussed active surveillance for low grade intermediate risk non muscle invasive bladder cancer. In his opinion, there are several reasons to consider active surveillance:
- There is overdiagnosis and overtreatment in low grade intermediate risk non muscle invasive bladder cancer
- Repeated TURBTs, cystoscopies, and instillations affect quality of life
- There is an economic burden with unnecessary interventions
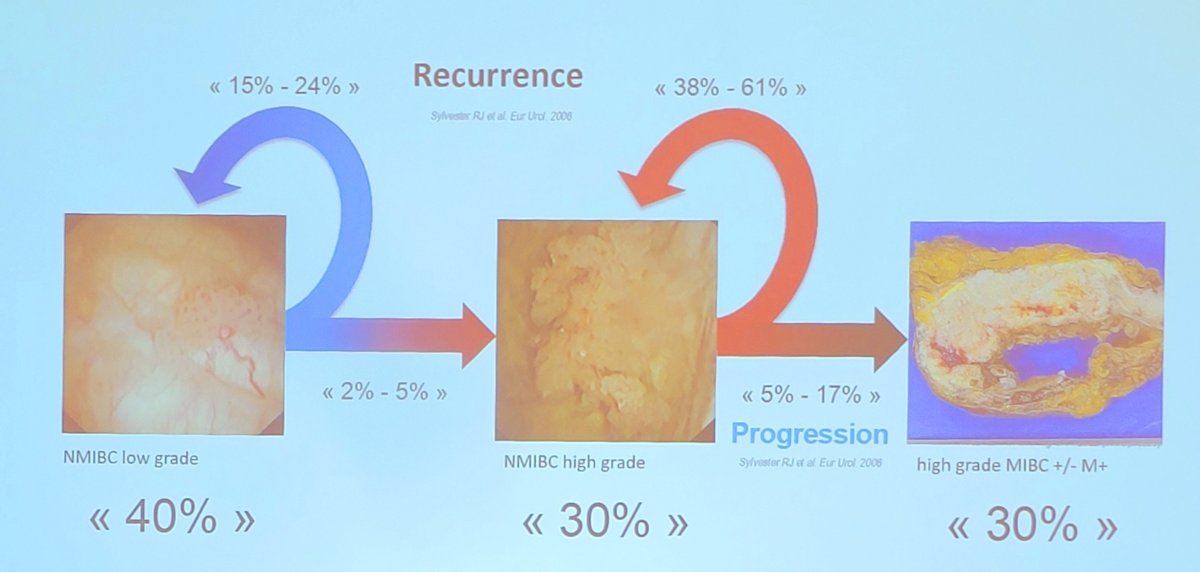
With regards to the epidemiology of low grade intermediate risk non muscle invasive bladder cancer, this substratification accounts for approximately 25% of newly diagnosed bladder cancer in the United States. The standard treatment is TURBT followed by adjuvant instillations of intravesical chemotherapy. Dr. Roupret notes that this is a disease of recurrence and not progression, given that 15-24% of low grade intermediate risk non muscle invasive bladder cancer will recur, but rarely progress (2-5%) to high grade non muscle invasive disease:
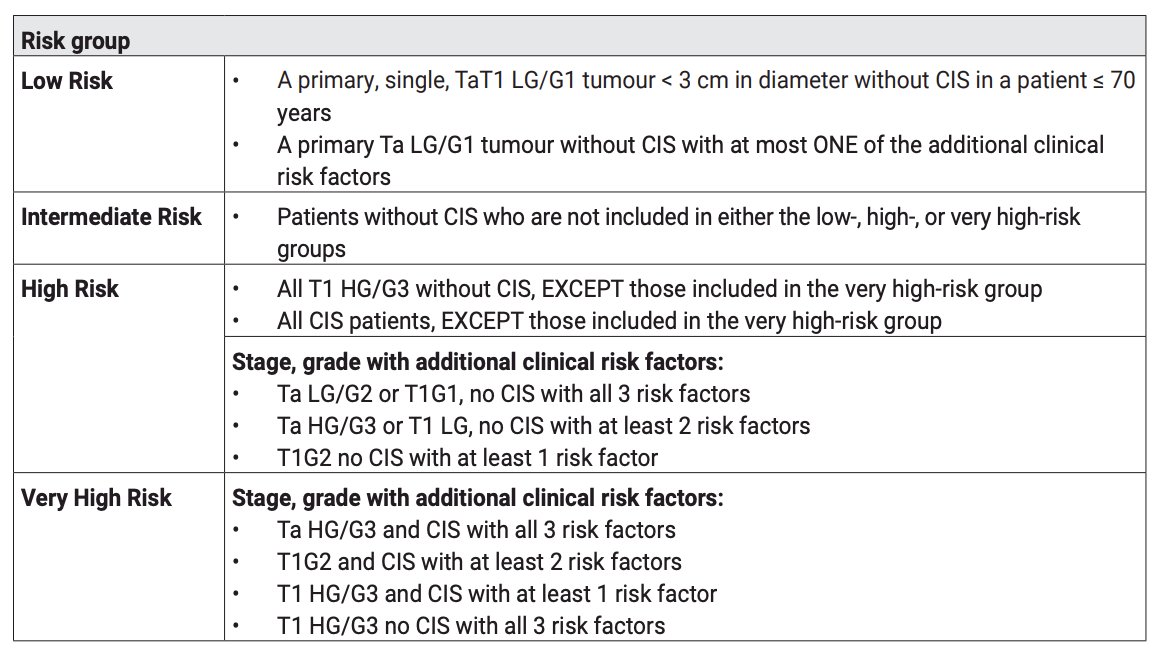
Dr. Roupret emphasized that this patient fits classically into the EAU intermediate risk disease group, with a low risk of disease progression:
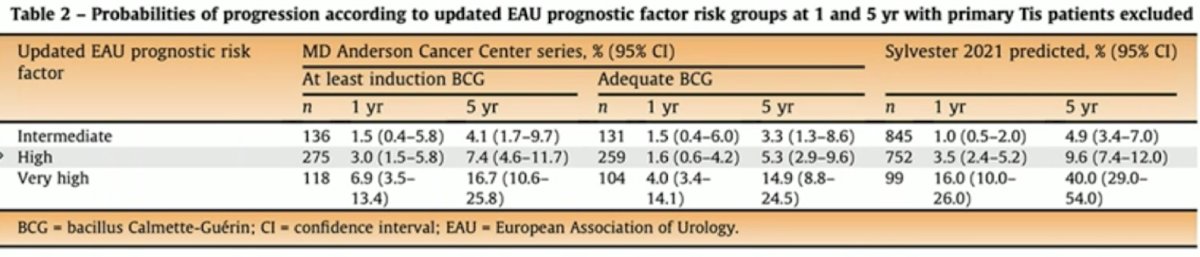
Based on the updated EAU prognostic factor risk groups in patients with non muscle invasive bladder cancer treated with BCG, the 1-year and 5-year risk of progression among intermediate risk disease treated with adequate BCG is low at 1.5% and 3.3%, respectively:
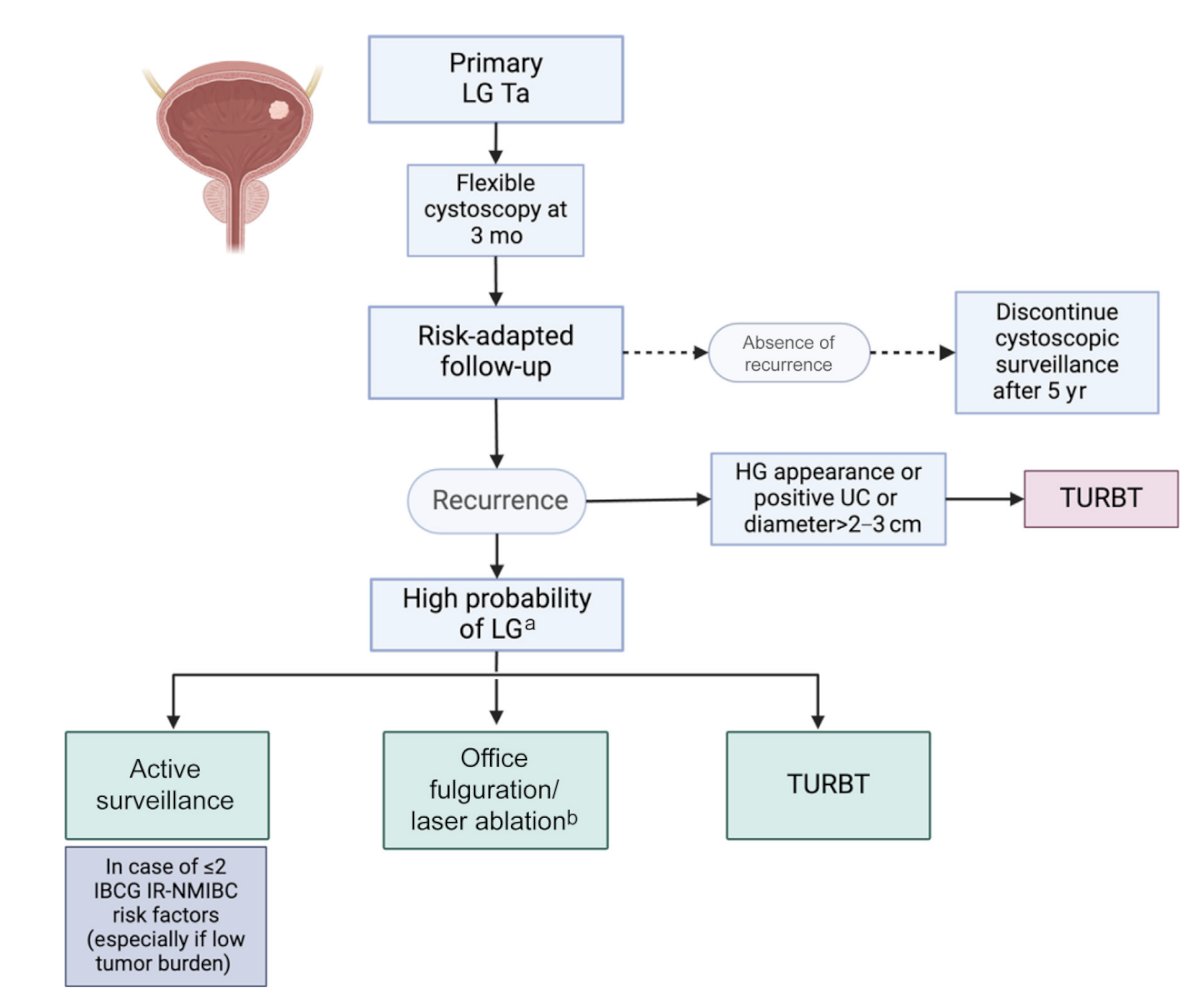
Moreover, the IBCG has recently published a collaborative review emphasizing deintensification of treatment for low grade bladder tumors.2 In 2023, the IBCG also assessed outcomes of intermediate risk patients undergoing active surveillance.3 In this study of 163 patients, over a median follow-up of 33 months (IQR 21-46), TURBT was performed on 109 patients. At a landmark time point of 24 months, patients with 0 risk factors were over 2-fold more likely to continue active surveillance compared to patients with ≥3 risk factors (59% versus 24%):
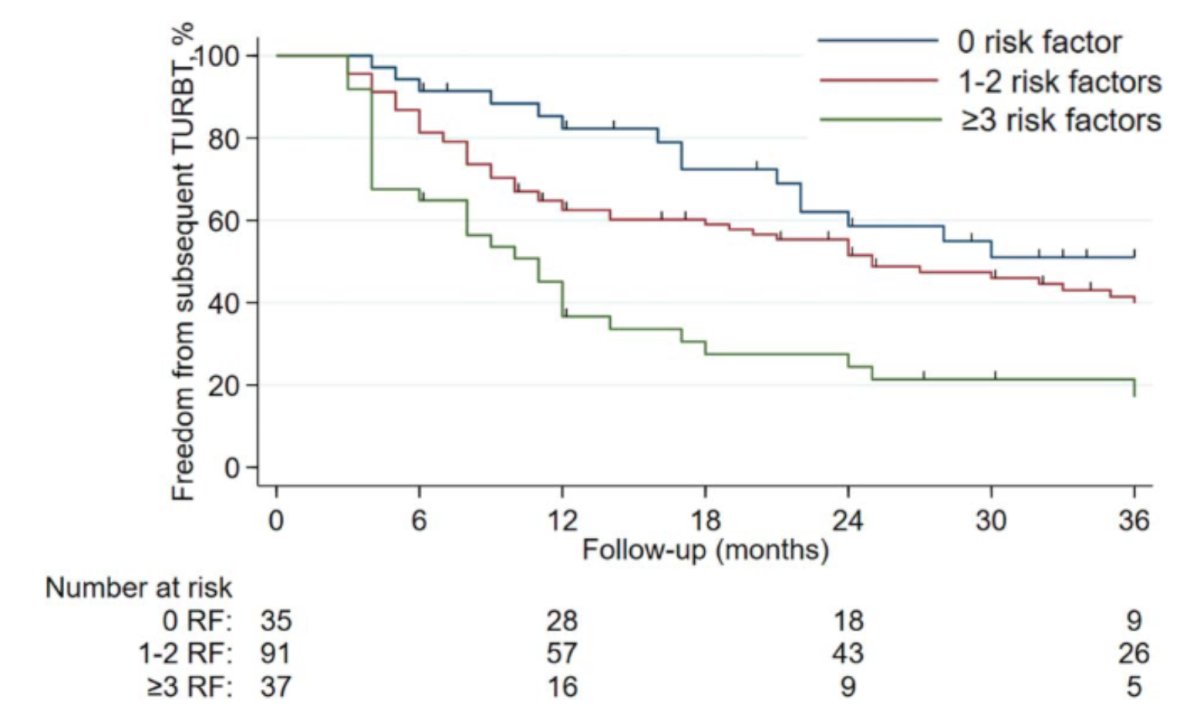
Multivariable Cox regression suggested that the IBCG intermediate risk non muscle invasive bladder cancer scoring system was associated with subsequent TURBT (1-2 risk factors [HR 1.66, 95% CI 0.96-2.90], ≥3 risk factors [HR 3.21, 95% CI: 1.70-6.09, p < 0.001]) after adjusting for age, T stage, and sex. The following is a proposed risk adapted approach by the IBCG for management of low grade Ta bladder tumors.2
Dr. Roupret concluded his argument for active surveillance in this patient with the following statements:
- Active surveillance preserves quality of life
- Active surveillance reduces healthcare costs
- Active surveillance maintains oncological safety in properly selected patients
- Active surveillance is rational, patient centered, evidence based, and future ready
Dr. Bukavina then presented her argument for why this patient is not an ideal candidate for active surveillance. For this patient, she notes that the tumor count doubled, increased in size, and notes that low grade does not mean harmless. With regards to his IBCG intermediate risk factors, she notes that this patient has four risk factors, and although he has comorbidities, he has already tolerated multiple TURBTs. Surveillance does not spare him interventions, it is just delaying the real ones, such as a radical cystectomy. If he is properly stratified as high intermediate risk, his recurrence and progression risk is as follows:
- 1 year recurrence: 33.5%
- 1 year progression: 2.6%
- 3 year recurrence: 67.5%
- 3 year progression: 8.2%
The Bladder Cancer Italian Active Surveillance (BIAS) protocol suggests that pragmatic deintensification is not always the answer.4 Among 251 patients on active surveillance, inclusion criteria included a history of low grade pTa/pT1a urothelial carcinoma, and < 5 tumors < 1cm in size. Triggers for treatment were an increase in size/number, gross hematuria, or positive cytology. This study showed that up to 40-60% of patients recur in low grade non muscle invasive bladder cancer, and progression to high grade or T1 occurs in 5-15% of patients over time. Thus, Dr. Bukavina notes that risk stratification is not perfect and can miss aggressive biology.
Surveillance also has its own burdens, including:
- Frequent cystoscopies: associated with anxiety, logistical, and financial burdens
- Multiple cystoscopies are not exactly “non-intervention”
- It is ‘death by a thousand scopes’
- Surveillance does not equal freedom from procedures
Dr. Bukavina concluded her argument against active surveillance for these patients with the following take-home messages:
- Urologists can only correctly predict tumor stage and grade in ~2/3 of cases
- So, if we are not good at predicting tumor stage and grade, how can we accurately predict who is a low grade intermediate risk patient?
- There is an opportunity cost for these patients: every delay in TURBT has the potential for upstaging
- In this case, active surveillance did not prevent recurrence, it hosted a bladder tumor party
The debate concluded by highlighting the pre- and post-debate answers to the polling question “What treatment option would you select?”
- TURBT
- Pre-debate: 54%
- Post-debate: 50%
- Active surveillance
- Pre-debate: 11%
- Post-debate: 3%
- Chemoablation
- Pre-debate: 7%
- Post-debate: 8%
- Office fulguration
- Pre-debate: 28%
- Post-debate: 39%
- Other
- Pre-debate: 0%
- Post-debate: 0%
Presented by:
- Laura Bukavina, MD, MPH, Cleveland Clinic, Cleveland, OH
- Morgan Roupret, MD, PhD, AP-HP Sorbonne University, Paris, France
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
Related content: Active Surveillance vs TURBT for Low-Grade Ta Bladder Cancer - Morgan Rouprêt & Laura Bukavina
References:
- Lobo N, Hensley PJ, Bree KK, et al. Updated European Association of Urology (EAU) Prognostic Factor Risk Groups Overestimate the Risk of Progression in Patients with Non-muscle-invasive Bladder Cancer Treated with Bacillus Calmette-Guerin. Eur Urol Oncol. 2022 Feb;5(1):84-91.
- Contieri R, Soloway MS, Gontero P, et al. Deintensification of treatment for low-grade bladder tumors: A collaborative review by the International Bladder Cancer Group (IBCG). Eur Urol Oncol. 2025 Feb;8(1):179-189.
- Tan WS, Contieri R, Buffi NM, et al. International Bladder Cancer Group Intermediate-risk nonmuscle-invasive bladder cancer scoring system predicts outcomes of patients on active surveillance. J Urol. 2023 Nov;210(5):763-770.
- Contieri R, Paciotti M, Lughezzani G, et la. Long-term follow-up and factors associated with active surveillance failure for patients with non-muscle-invasive bladder cancer: The Bladder Cancer Italian Active Surveillance (BIAS) experience. Eur Urol Oncol. 2022 Apr;(5):251-255.