(UroToday.com) The American Urological Association (AUA) 2025 Annual Meeting, held in Las Vegas, NV, was host to a bladder cancer clinical trials in progress session. Dr. Trinity Bivalacqua presented updates to the trial protocol of CORE-008, a phase II multi-arm, multi-cohort trial evaluating intravesical cretostimogene grenadenorepvec in high-risk, non-muscle invasive bladder cancer (NMIBC) patients.
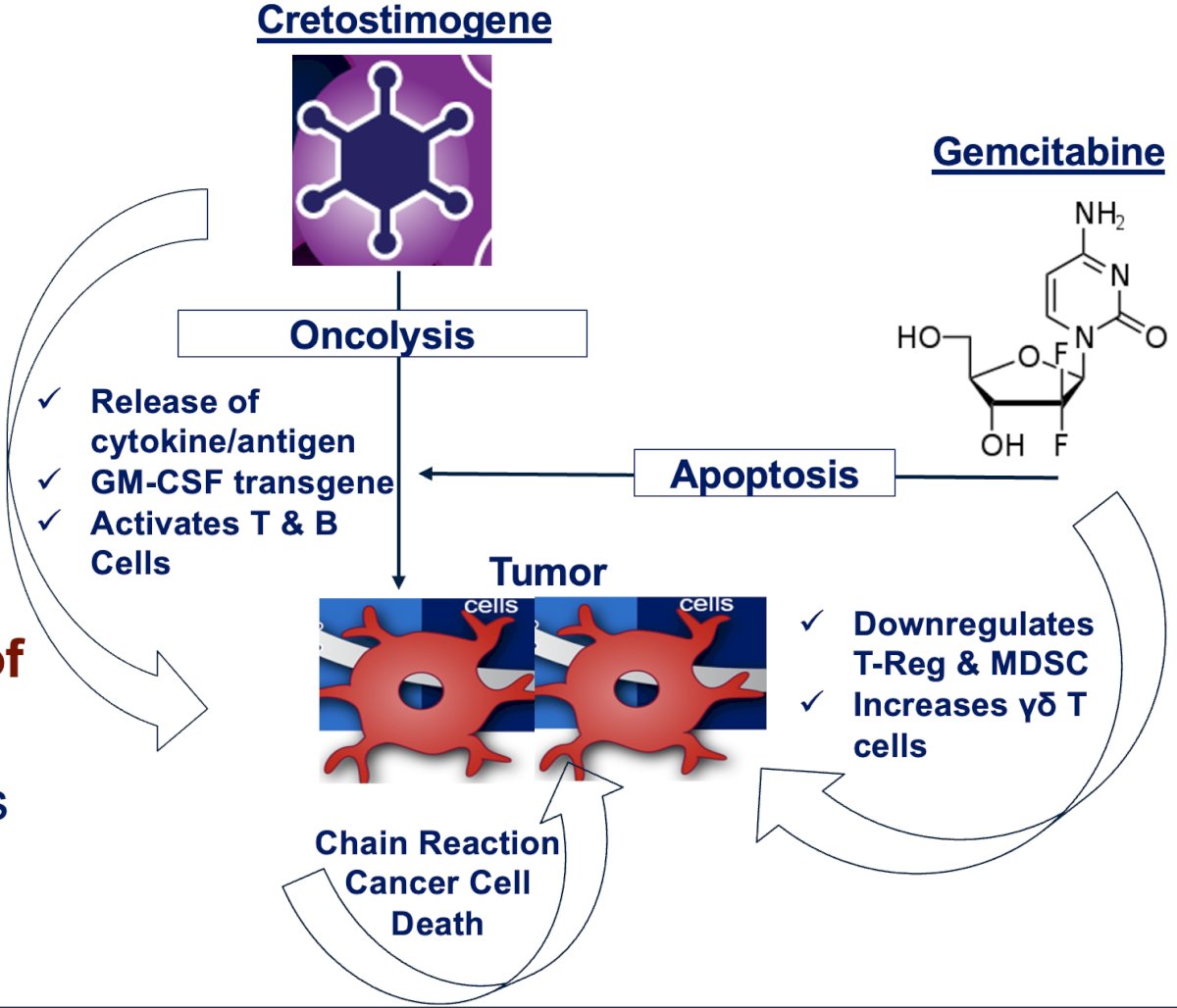
Cretostimogene grenadenorepvec works in two important and complementary ways. First, it selectively replicates inside tumor cells with RB-E2F alterations, causing tumor cell lysis and immunogenic cell death. The rupture of the cancer cells releases tumor-derived antigens, along with GM-CSF, that can stimulate a systemic anti-tumor immune response involving the body’s immune system.

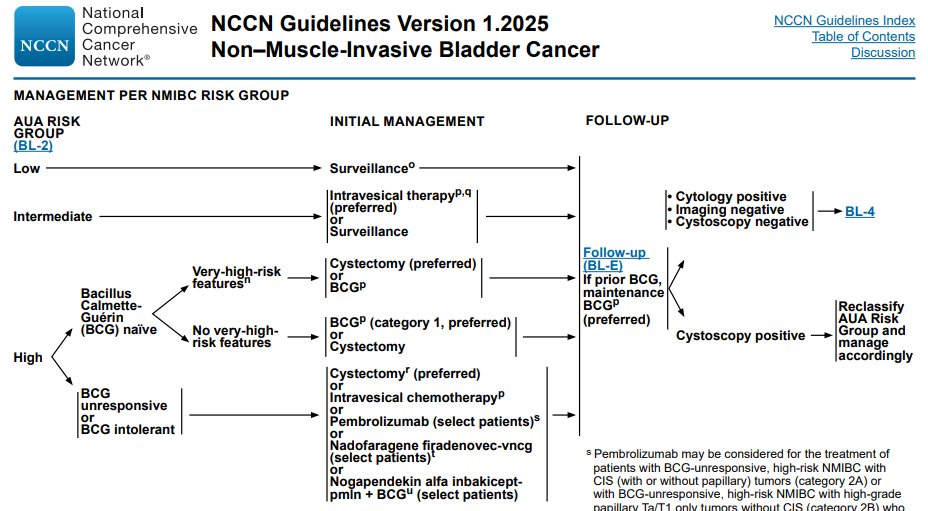
Current guidelines recommend either intravesical BCG instillations or radical cystectomy for patients with high-risk NMIBC. Current challenges with BCG include:
- High recurrence rates (up to 50%)
- High progression rates (20–40%)
- Ongoing BCG shortages
Furthermore, radical cystectomy has a significant impact on quality of life and is associated with significant perioperative morbidity. As such, there is a high unmet need in the high-risk NMIBC disease space.
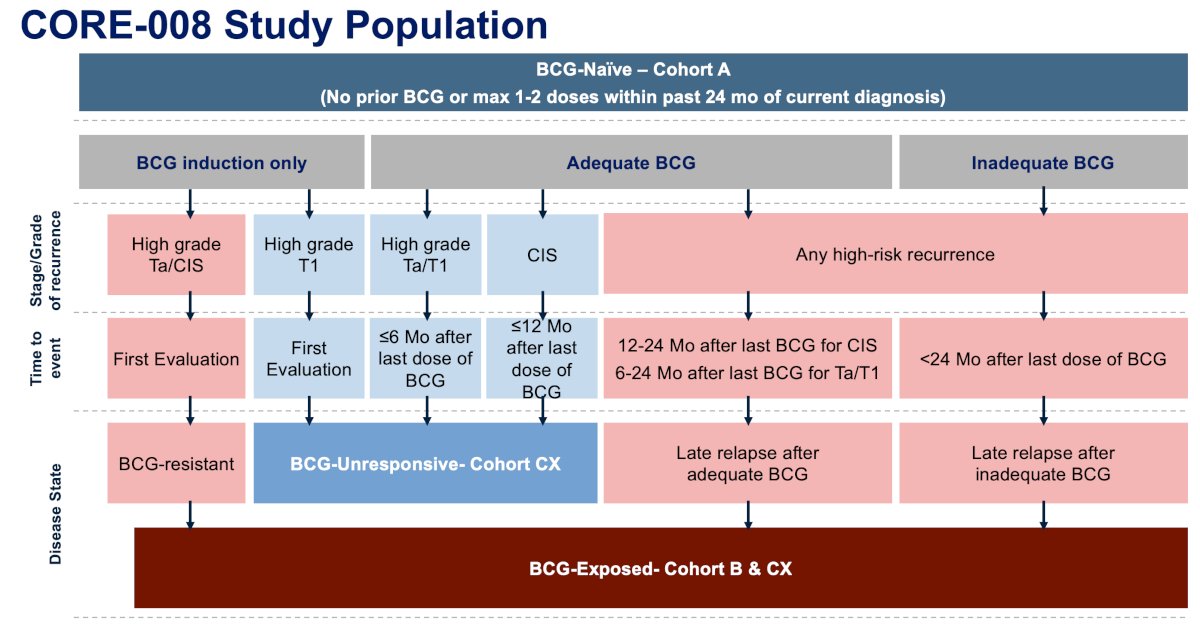
The CORE-008 study population is summarized below. CORE-008 is assessing the efficacy and safety of cretostimogene in a broad HR NMIBC population. Cohort A includes BCG-naïve patients (i.e., no prior BCG or 1-2 doses within the preceding 24 months of diagnosis). The red boxes below include BCG-exposed (Cohort B) patients who have received prior BCG and recurred either immediately at the 1st evaluation (BCG-resistant) or recurred at a delayed timepoint, after either adequate or inadequate BCG. Cohort CX will include BCG-exposed and BCG-unresponsive patients, highlighted in the light blue boxes. These patients must receive adequate BCG and present with recurrence at specified timepoints.
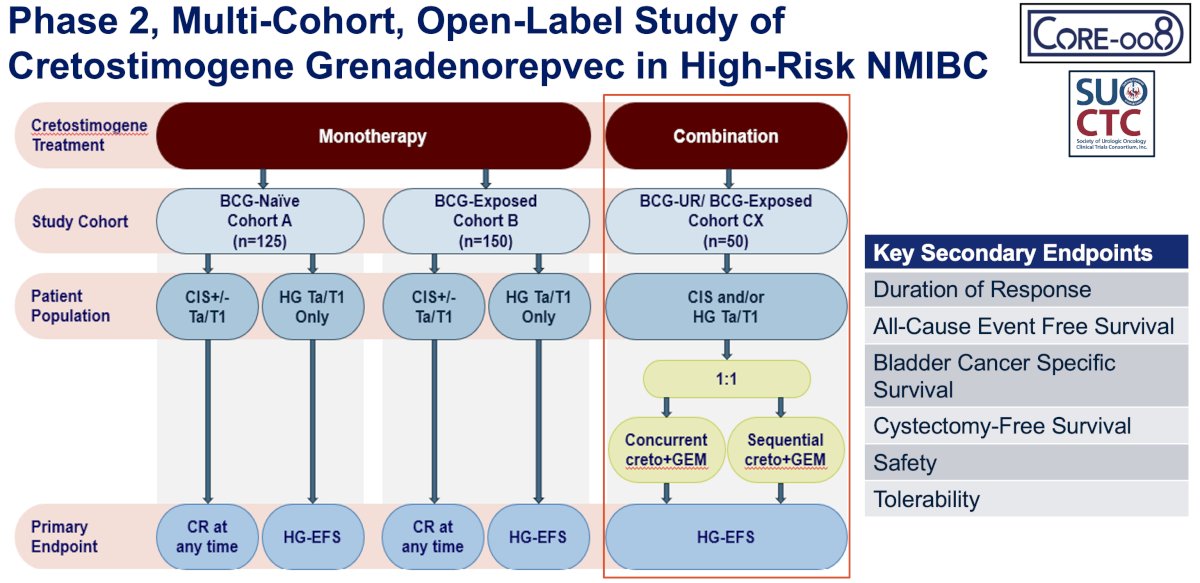
CORE-008 is a phase II, multi-arm, multi-cohort trial to further evaluate the efficacy and safety of cretostimogene in patients with HR NMIBC, as defined by the AUA guidelines. Two cohorts are specific for cretostimogene monotherapy:
- Cohort A (BCG-naive) includes patients who have not received prior BCG.
- Cohort B (BCG-exposed) consists of patients who have received prior BCG and recurred at the initial clinical evaluation at a delayed time point.
Eligibility criteria have been updated to allow both CIS-containing and papillary-only patients in both cohorts. The primary endpoint includes complete response at any time for the CIS containing and high-grade event-free survival (HG-EFS) for the papillary-only populations.
In Cohort CX, BCG-unresponsive/exposed patients will receive cretostimogene in combination with intravesical gemcitabine, randomized to either concurrent administration (Arm 1) or sequential therapy (Arm 2).
What is the rationale for combining cretostimogene with gemcitabine? It is hypothesized that this combination of intravesical cretostimogene with gemcitabine will utilize complementary mechanisms of action and potential immune modulating synergy to enhance outcomes. The efficacy, safety, and tolerability of this combination have been demonstrated, and prior phase I-III studies of gemcitabine + immunotherapy (e.g., BCG, pembrolizumab) have demonstrated promising results in high-risk NMIBC. Proposed complementary mechanisms of action include:
- Direct oncolytic and pro-apoptotic effects
- Potential immune modulating synergy
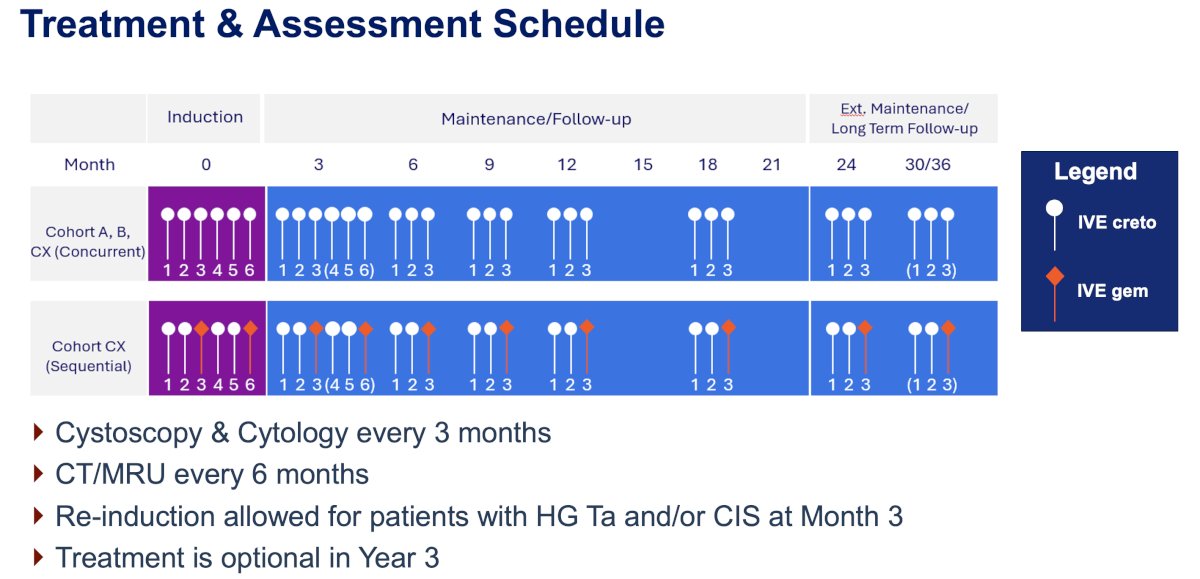
Intravesical cretostimogene will be instilled in combination with DDM, an excipient that enhances adenoviral delivery, for six weekly doses during the induction phase, followed by three weekly maintenance cycles quarterly through month 12, then every six months through month 36. Participants were eligible for repeat induction therapy at Month 3 if persistent HG Ta or CIS was noted at biopsy. Specifically, for patients within Cohort CX randomized to sequential treatment, patients will receive cretostimogene on Weeks 1, 2, 4, and 5, and gemcitabine on Weeks 3 and 6 (as shown in orange). This cycle of 2 weekly cretostimogene instillations followed by a single gemcitabine instillation will continue in maintenance. Disease assessments include serial cystoscopy, urine cytology, axial imaging, and directed bladder biopsies.
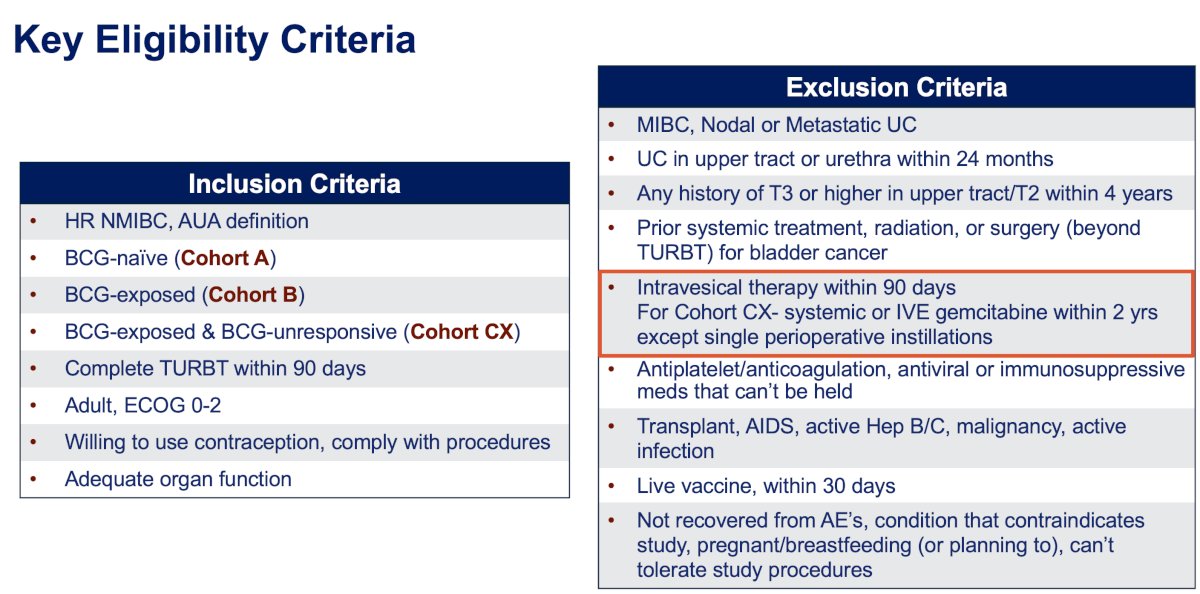
The study's key eligibility criteria are summarized below.
CORE-008 is currently ongoing and actively enrolling. As of April 2025:
- Cohort A (BCG-Naïve)
- CIS containing arms has completed enrollment
- HG Ta/T1 arm is planned
- Cohort B (BCG-Exposed) is planned and received collaborative SUO-CTC support
- Cohort CX (BCG-Exposed & BCG-unresponsive): Open as of April 21, 2025

Presented by: Trinity Bivalacqua, MD, PhD, Professor, Department of Urology, University of Pennsylvania Perelman School of Medicine, Philadelphia, PA
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
Related content: CORE-008 Cohort A: Cretostimogene in BCG-Naïve High-Risk NMIBC – Trial Design & Update - Trinity Bivalacqua
CORE-008 Cohort B: Cretostimogene for BCG-Exposed NMIBC – Trial Activation & Clinical Goals - Trinity Bivalacqua
CORE-008 Trial Cohort CX: Combining Cretostimogene Grenadenorepvec and Gemcitabine for Bladder Cancer - Trinity Bivalacqua