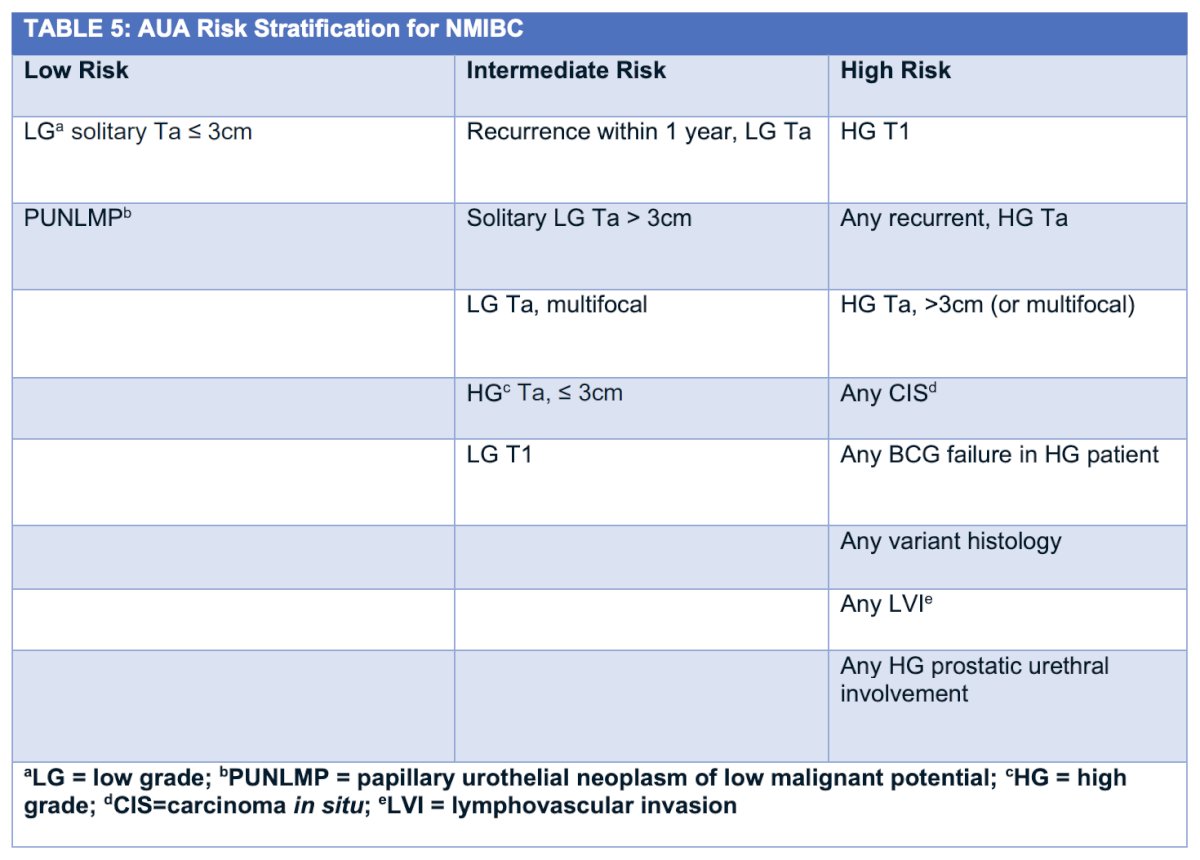
(UroToday.com) The 2025 AUA annual meeting featured the IBCG Bladder Cancer Forum evaluating common problems and controversies in bladder cancer, moderated by Dr. Laura Mertens, with a debate between Drs. Joshua Meeks and Benjamin Pradere are discussing balancing BCG with new and emerging treatments in the era of personalized medicine for patients with high risk non-muscle invasive bladder cancer (NMIBC). Dr. Mertens started by noting that there is heterogeneity in risk stratification of non muscle invasive bladder cancer, highlighting the differences between the AUA/SUO guidelines:
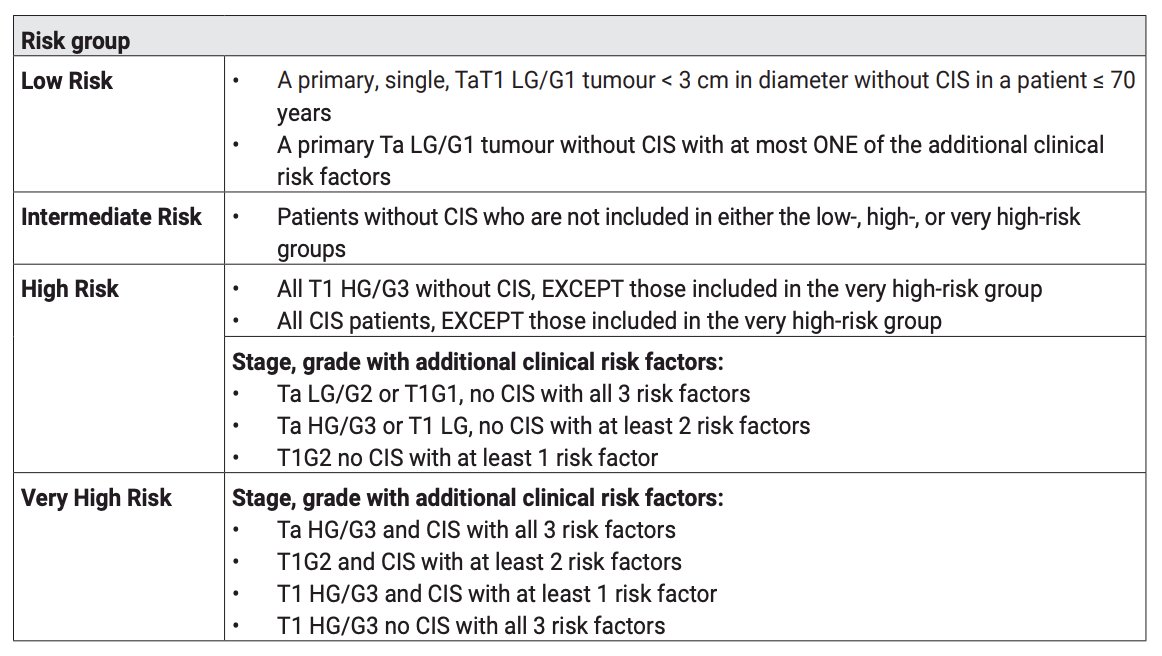
and the EAU guidelines:
Next, Dr. Mertens presented a case of a 71-year-old man who presented with hematuria. He was a former machine operator, ex-smoker, and had a medical history significant for hypertension, diabetes mellitus, chronic renal insufficiency, and a BMI of 35 kg/m2. Cystoscopy showed a ~4 cm high risk tumor. In these situations, the EAU guidelines state that:
- In a high risk patient with newly diagnosed CIS, high grade T1 or high risk Ta urothelial carcinoma, a clinician should administer a six week induction course of BCG (Strong recommendation; Evidence Strength: Grade B)
- In a high risk patient who completely response to induction BCG, a clinician should continue maintenance BCG, based on availability, for three years, as tolerated (Moderate recommendation; Evidence Strength: Grade B)
Dr. Mertens then polled the audience based on the following question: “How would you treat this patient with high risk non muscle invasive bladder cancer?”. The following were the options available:
- BCG induction + 1 year of maintenance
- BCG induction + 3 years of maintenance
- Alternative intravesical agent
- Alternative systemic agent
- Immediate cystectomy
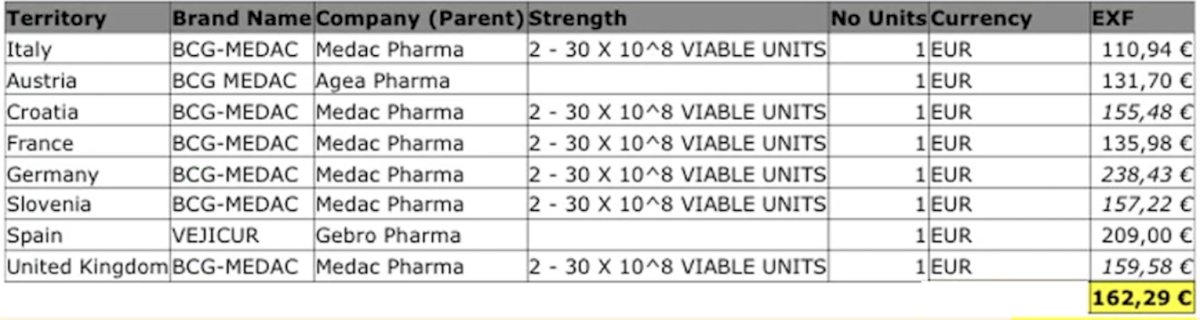
Dr. Josh Meeks then discussed that BCG remains the best option in this disease space. He notes that, based on multiple studies, BCG is the most efficacious. Matulay et al.1 retrospectively reviewed patients receiving adequate BCG therapy at MD Anderson Cancer Center between January 2004 and August 2018. Among 542 patients who received adequate BCG, 518 (90%) had EAU high-risk disease, with CIS present in 175 (32%) specimens. Over a median follow-up of 47.8 months, freedom from high-grade recurrence at 1, 3, and 5 years was 81%, 76%, and 74%, respectively, and progression-free survival was 97%, 93%, and 92%, respectively. Progression to muscle invasion at 5 years was exclusively seen in patients with high-risk disease (progression-free survival 91%; log-rank test, p = 0.024). Moreover, Dr. Meeks notes that BCG is the most tolerable regimen, with side effects that urologists are familiar with and comfortable managing. In addition, response to BCG is prognostic and is also the financially best choice:
Moreover, there are no biomarkers needed for BCG, and BCG remodels the bladder immune environment. The following demonstrates the enormous remodeling of the T cell microenvironment after BCG administration: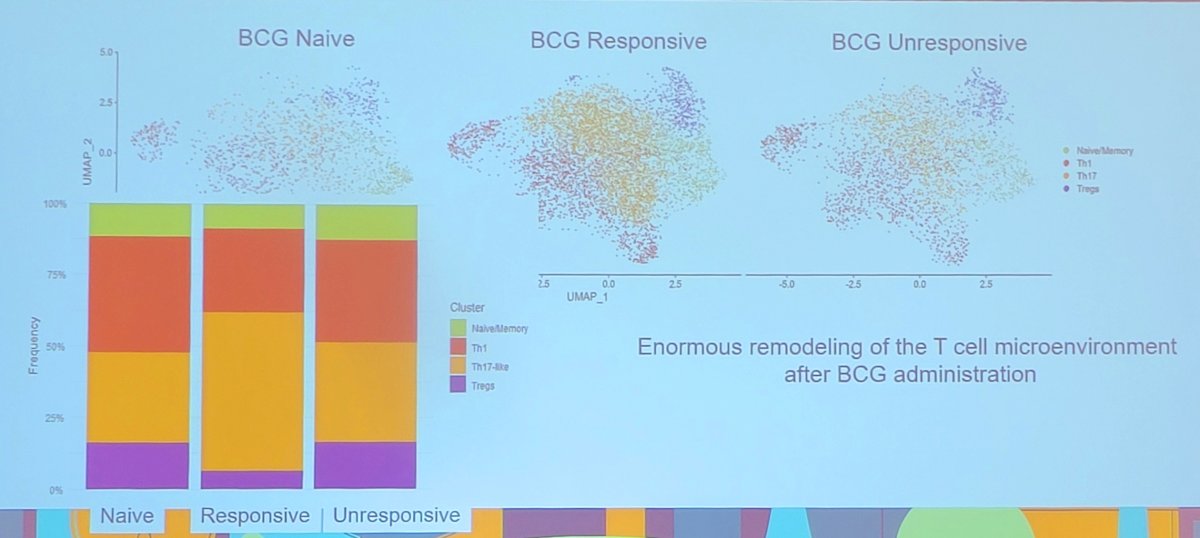
In summary, Dr. Meeks stated that BCG is good, cheap, and tolerable, and our urology clinics are well designed to administer BCG.
Dr. Pradere then discussed alternatives to BCG in this disease space, but first noted that BCG is, in fact, great. However, there are some nuances to how good BCG may be. For example, in the NIMBUS trial,2 345 patients from 51 sites were randomized between December 2013 and July 2019. The standard BCG schedule was 6 weeks of induction followed by 3 weeks of maintenance at 3, 6, and 12 month (15 instillations). The reduced frequency BCG schedule was induction at weeks 1, 2, and 6 followed by 2 weeks (week 1 and 3) of maintenance at 3, 6, and 12 month (nine instillations):
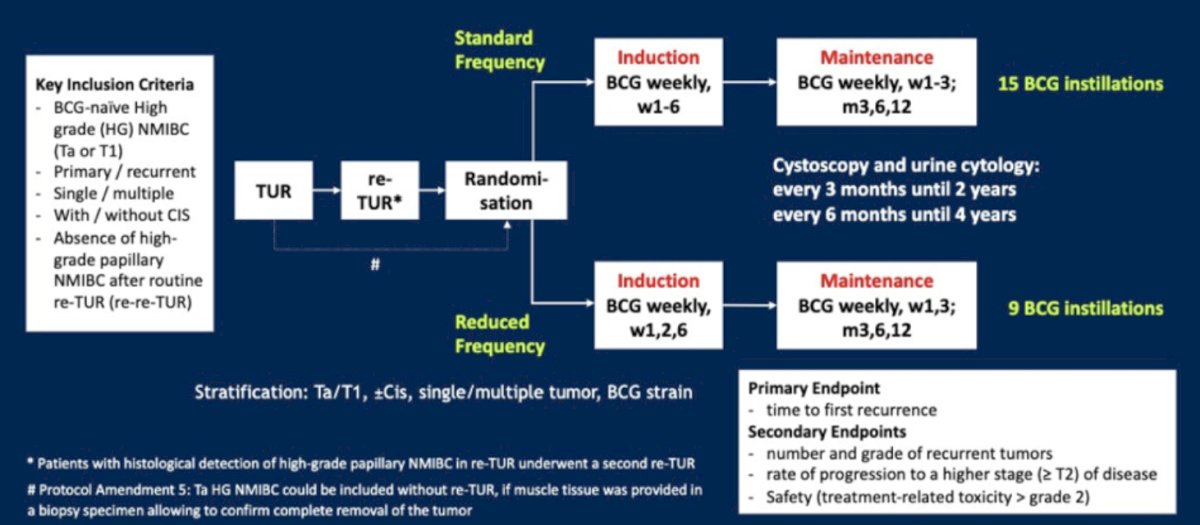
Overall, 170 patients were randomized to reduced frequency and 175 to standard BCG. After a 12 month of median follow-up, the intention-to-treat analysis showed a safety-relevant difference in recurrences between treatment arms: 46/170 (reduced frequency) versus 21/175 patients (standard). Based on these results, the trial concluded that the reduced frequency schedule was inferior to the standard schedule regarding the time to first recurrence.
Dr. Pradere also notes that there are logistical and clinical pitfalls of BCG. Logistically, you need to have a good TURBT, adherence to the maintenance schedule, and there is, particularly in the United States, a BCG shortage. Clinically, there may be issues with tolerance, recurrence, and progression with BCG:
There are also heterogeneous outcomes with BCG, highlighting that not all high risk non muscle invasive bladder cancer is the same:
- Recurrence:
- 1 year recurrence free survival: 66% to 96%
- 2 year recurrence free survival: 63% to 96%
- 5 year recurrence free survival: 39% to 66%
- Progression:
- 1 year progression free survival: 81% to 98%
- 2 year progression free survival: 70% to 96%
- 5 year progression free survival: 70% to 84%
Dr. Pradere notes that for safety and tolerance, BCG is not great, but urologists are used to it. Local BCG-related toxicity is ~63%, and systemic BCG-related toxicity is ~32%. Importantly, up to 70% of patients experience local or systemic side effects, and 20% discontinue BCG due to intolerance. In the NIMBUS trial, 82% of patients in the control arm had an adverse event, and in the recently presented at AUA 2025 CREST trial, 64% of patients in the BCG control arm had an adverse event. Adherence to long-term maintenance BCG is challenging, and Dr. Pradere notes that previous studies suggest that adherence to maintenance is limited to 50% at 9 months and 10% at 3 years. This was corroborated in the CREST trial, which showed a 40% discontinuation rate in the BCG control arm. Dr. Pradere notes that there are several alternatives in the making, as highlighted in the following figure:3
![This was corroborated in the CREST trial that showed a 40% discontinuation rate in the BCG control arm. Dr. Pradere notes that there are several alternatives in the making, as highlighted in the following figure [3]:](/images/com-doc-importer/207-aua-2025/aua-2025-patient-with-high-risk-nmibc-balancing-bcg-with-new-and-emerging-treatments-in-the-era-of-personalized-medicine/image-6.jpg)
With regards to gemcitabine + docetaxel in this disease space, although there are no large clinical trial, there is a body of evidence suggesting efficacy and safety in intermediate risk, high risk, and very high risk patients. The Hopkins experience included a prospective phase 2 trial of 25 BCG naïve patients with a median follow-up of 20 months.4 There was a 100% complete response rate at 3 months, with a 12-month recurrence-free survival of 92%, with no progression and no patients requiring radical cystectomy. In a multicenter assessment of gemcitabine + docetaxel in intermediate risk disease, Tan et al. evaluated oncological outcomes for 182 patients treated with BCG (n = 100) or intravesical sequential gemcitabine and docetaxel (n = 82).5 Notably, recurrence rates were similar in the two treatment groups (HR 1.06, 95% CI 0.65-1.73; p = 0.8).
Finally, the CREST trial presented at AUA 2025 was a three-arm study comparing different combinations of sasanlimab and BCG. Arm A received sasanlimab administered subcutaneously combined with BCG induction and maintenance, Arm B received sasanlimab with BCG induction only, and Arm C received BCG induction and maintenance alone. For the presentation at AUA 2025, the focus was on the comparison between Arm A and Arm C. The primary endpoint was event-free survival, defined as recurrence of high-grade disease, progressive disease, persistence of CIS, or death from any cause: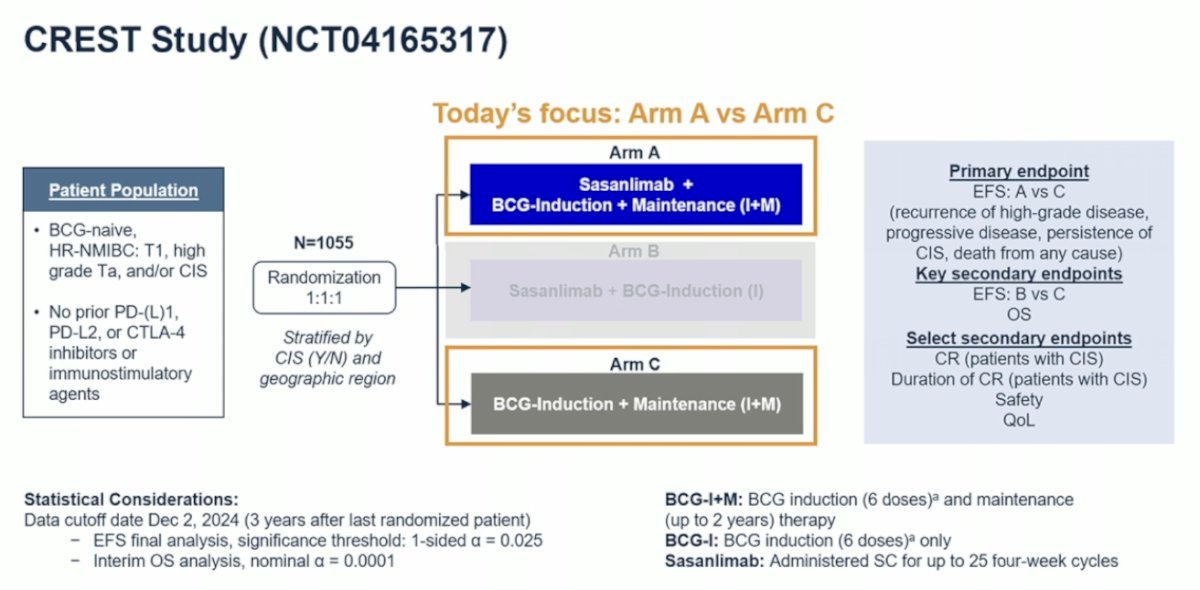
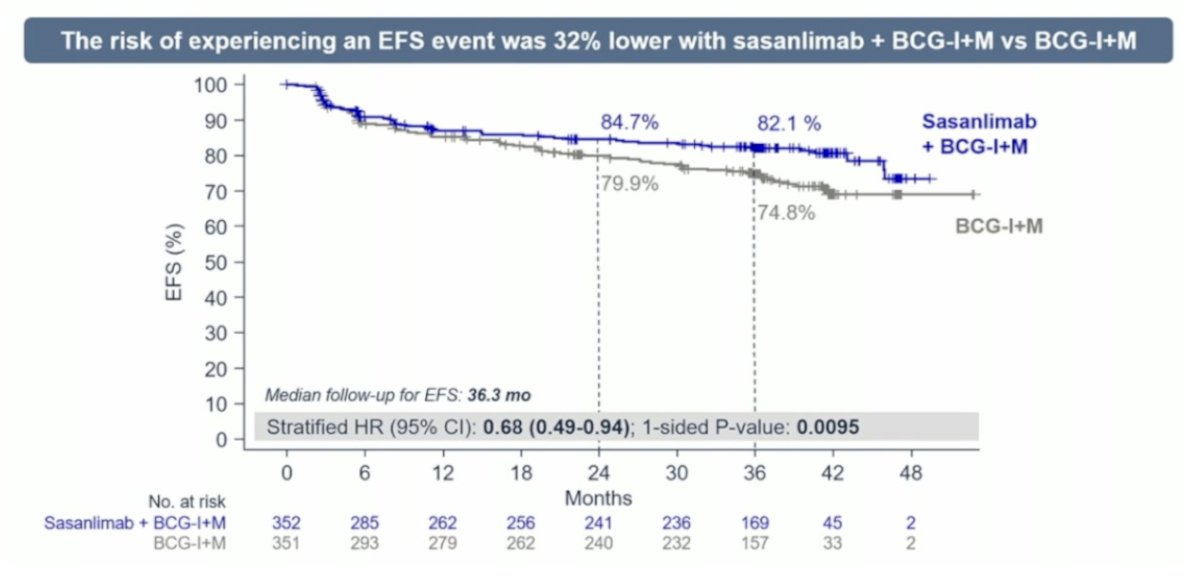
Over a median follow-up of 36.3 months, the risk of experiencing an event-free survival event was 32% lower with sasanlimab + BCG compared to BCG induction and maintenance alone (stratified HR 0.68, 95% CI 0.49–0.94; 1-sided p-value = 0.0095):
In patients with CIS, the probability of maintaining a complete response at 36 months was 92% with sasanlimab plus BCG induction and maintenance, compared to 84.7% with BCG induction and maintenance alone: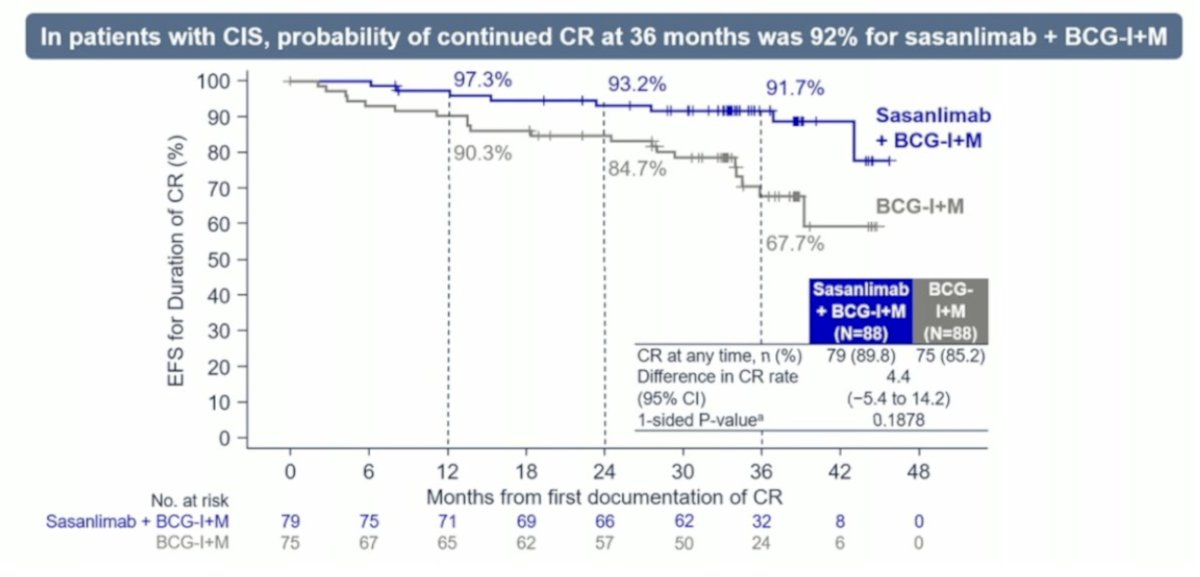
Dr. Pradere concluded his debate presentation by conceding that BCG is a king in this disease space, but is in danger and may not stay the only option. There are many challenges that remain to be addressed, interpreted, and discussed.
The debate concluded by highlighting the pre- and post-debate answers to the polling question “How would you treat this patient with high-risk non-muscle invasive bladder cancer?”:
- BCG induction + 1 year of maintenance
- Pre-debate: 42%
- Post-debate: 29%
- BCG induction + 3 years of maintenance
- Pre-debate: 49%
- Post-debate: 57%
- Alternative intravesical agent
- Pre-debate: 6%
- Post-debate: 9%
- Alternative systemic agent
- Pre-debate: 0%
- Post-debate: 1%
- Immediate cystectomy
- Pre-debate: 3%
- Post-debate: 3%
Moderated by: Laura Mertens, Netherlands Cancer Institute, Amsterdam, Netherlands
Presented by:
- Joshua Meeks, Northwestern University Feinberg School of Medicine, Chicago, IL
- Benjamin Pradere, La Croix du Sud Hospital, Kigali, Rwanda
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, NV.
Related content: BCG Efficacy in Bladder Cancer Amid Emerging Immunotherapy Combinations - Joshua Meeks & Benjamin Pradere
References:
- Matulay JT, Li R, Hensley PJ, et al. Contemporary Outcomes of Patients with Nonmuscle-Invasive Bladder Cancer Treated with Bacillus Calmette-Guérin: Implications for Clinical Trial Design. J Urol. 2021;205(6):1612-1621.
- Grimm MO, van der Hiejden AG, Colombel M, et al. Treatment of High-grade non-muscle-invasive bladder carcinoma by standard number and dose of BCG instillations versus reduced number and standard dose of BCG instillations: Results of the European Association of Urology Research Foundation Randomized Phase III Clinical Trial “NIMBUS”. Eur Urol 2020 Nov;78(5):690-698.
- Longoni M, Scilipoti P, Soria F, et al. Oncological outcomes in Bacillus Calemette-Guerin-naïve high-risk non-muscle-invasive bladder cancer patients: A systematic review on current treatment strategies and future perspectives. Eur Urol Oncol. 2025 Apr 8:S2588-9311(25)00081-1.
- Patel SH, Gabrielson AT, Chan S, et al. A phase 2 trial of intravesical gemcitabine and docetaxel in the treatment of Bacillus Calmette-Guerin-naïve nonmuscle-invasive urothelial carcinoma of the bladder. J Urol. 2024 Jul;212(1):95103.
- Tan WS, McElree IM, Davaro F, et al. Sequential intravesical gemcitabine and docetaxel is an alternative to Bacillus Calmette-Guerin for the treatment of intermediate-risk non-muscle invasive bladder cancer. Eur Urol Oncol. 2023 Oct;6(5):531-534.