(UroToday.com) The 2025 AUA annual meeting featured the IBCG Bladder Cancer Forum evaluating common problems and controversies in bladder cancer, moderated by Dr. Patrick Hensley, with a debate between Drs. Hikmat Al-Ahmadie and Alexandre Zlotta discussing whether there is a role for artificial intelligence in diagnosis and risk stratification for bladder cancer.
Dr. Hensley started with a case presentation of a healthy 65 year old female that presented with gross hematuria. The patient’s urine cytology was negative, and subsequent cystoscopy showed a solitary 3 cm papillary lesion. A subsequent TURBT showed a low grade (G2) Ta tumor, with a 3% high grade component (G3). Dr. Hensley then polled the audience based on the following question: “Is there a role for artificial intelligence informed non muscle invasive bladder cancer risk stratification in 2025?”. The following were the options available:
- Clinical artificial intelligence risk stratification only
- Pathological artificial intelligence risk stratification only
- Both clinical and pathological artificial intelligence risk stratification
- Neither is ready for primetime
Dr. Zlotta then discussed artificial intelligence in clinical stratification. He notes that there are currently several unmet needs:
- Minimize variability of pathological grading – can artificial intelligence help? Unlikely
- Less variability among surgeons – can artificial intelligence help? No
- Better non muscle invasive bladder cancer prognostic tools – can artificial intelligence help? Yes
In a study from Dr. Zlotta’s group published in 2025 in the Journal of Urology,1 they suggest that better tools are needed to minimize interobserver variability in pathological grading. This is secondary to grading concordance between uro-pathologists being quite poor:
- 2004/2022 system: concordance index: 0.78 (95% CI 0.65-0.90)
- WHO 1973 system: concordance index: 0.41 (95% CI 0.32-0.50)
Moreover, there is significant variation in the early recurrence rate of non muscle invasive bladder cancer after TURBT between sites that can not be explained by currently understood tumor features. For example, in the RESECT study, there were noted differences in surgical technique (and surgeons), as well as perioperative practices playing a role. For the remainder of his debate presentation, Dr. Zlotta highlighted work presented at AUA 2025 by his group (presenter: Dr. Jethro Kwong) assessing PROGRxN-BCa, an artificial intelligence-based model to predict progression risk in non muscle invasive bladder cancer to improve the sub-stratification of intermediate-risk disease non muscle invasive bladder cancer patients.
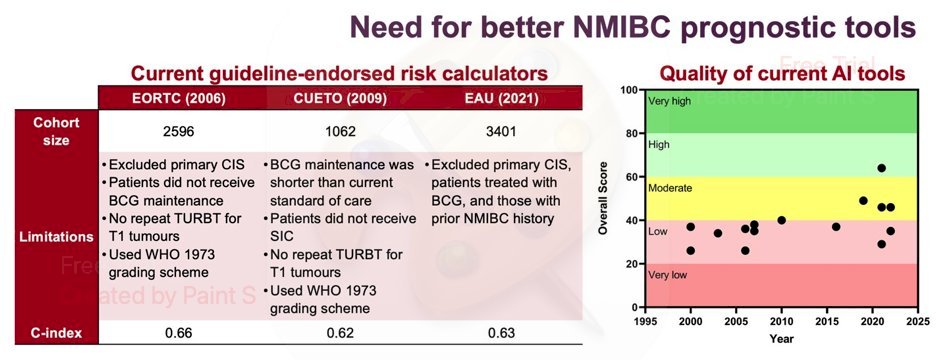
Accurate prediction of tumor progression is vital to inform patient counselling, intensify treatment when appropriate, and consider eligibility for clinical trials. However, there are numerous limitations with both clinical and artificial intelligence tools available today:
This study, presented at AUA 2025, is the largest non muscle invasive bladder cancer cohort to date (n=12,659). The model was developed using a training set of 3,324 patients treated at 4 academic or community hospitals between 2005 and 2022. It then underwent external validation using a cohort of 9,335 patients treated at 30 North American and European institutions between 2005 and 2023. PROGRxN-BCa was based on a random survival forest, and it was compared against the current guideline endorsed EAU risk calculator for the outcome of time to progression to muscle invasive or metastatic disease.
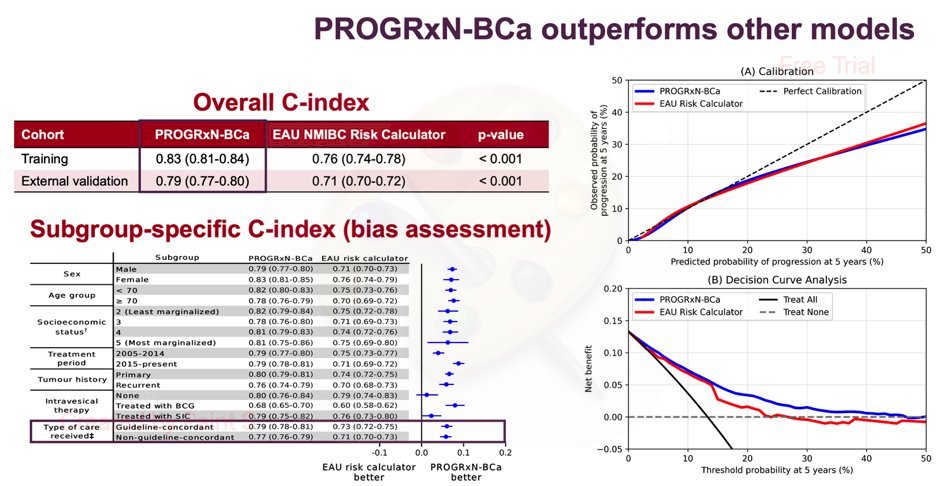
The study investigators found that:
- The PROGRxN-BCa artificial intelligence model outperformed the other models based on overall c-index and across clinically relevant subgroups, generally around 10% better
- What is notable is that this model was also consistently better, irrespective of whether guideline concordant care was followed (ie, repeat TURBT, BCG for T1, etc)
- This model is also well calibrated and has a higher net benefit on decision curve analysis
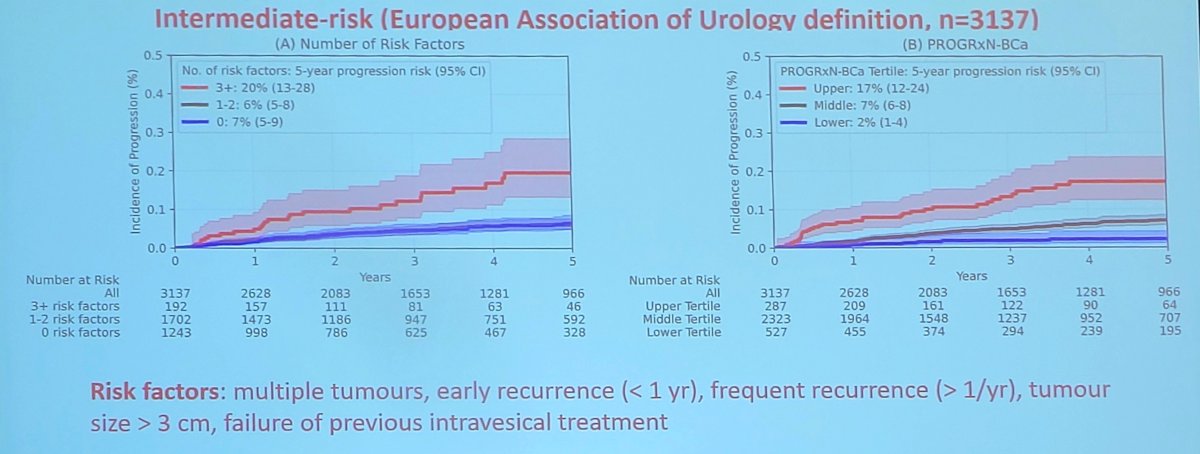
The study investigators also looked at the sub-stratification of intermediate-risk patients. Current guidelines recommend counting the number of intermediate risk factors, but it is challenging to distinguish patients with 0 risk factors from those with 1-2. However, with this artificial intelligence model, patients can be separated into distinct risk tertiles:
The conclusions from this international validation of PROGRxN-BCa were as follows:
- PROGRxN-BCa outperformed current tools in the largest non muscle invasive bladder cancer cohort of its kind, improving substratification and potentially optimizing risk-adapted management for guidelines
- Improvement was consistent among patients who received guideline concordant or non-guideline concordant care, and among patients who had at least five years of follow-up (n = 3,133)
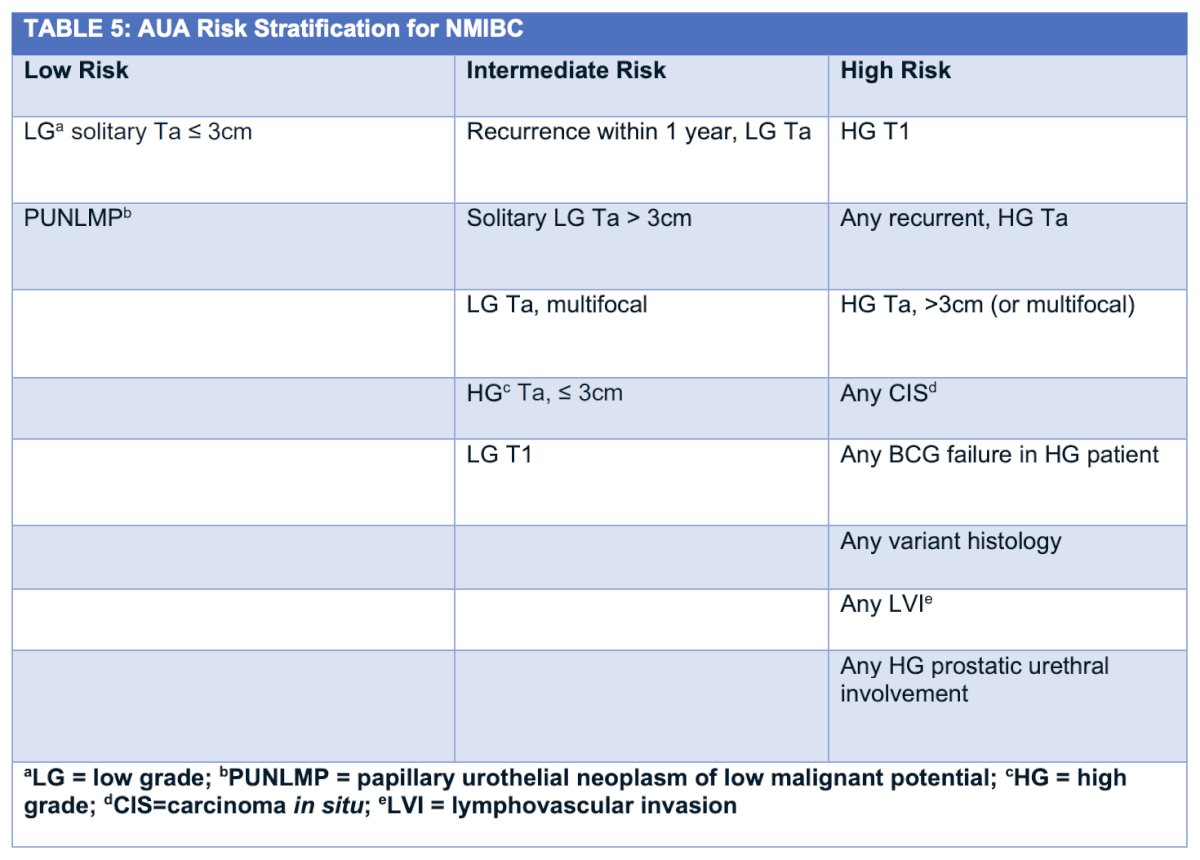
Dr. Al-Ahmadie then discussed artificial intelligence in histopathological substratification. At a high level, classification of urothelial neoplasms is dichotomized as non muscle invasive bladder cancer and muscle invasive bladder cancer. The following table highlights the current AUA/SUO guidelines for non muscle invasive bladder cancer:
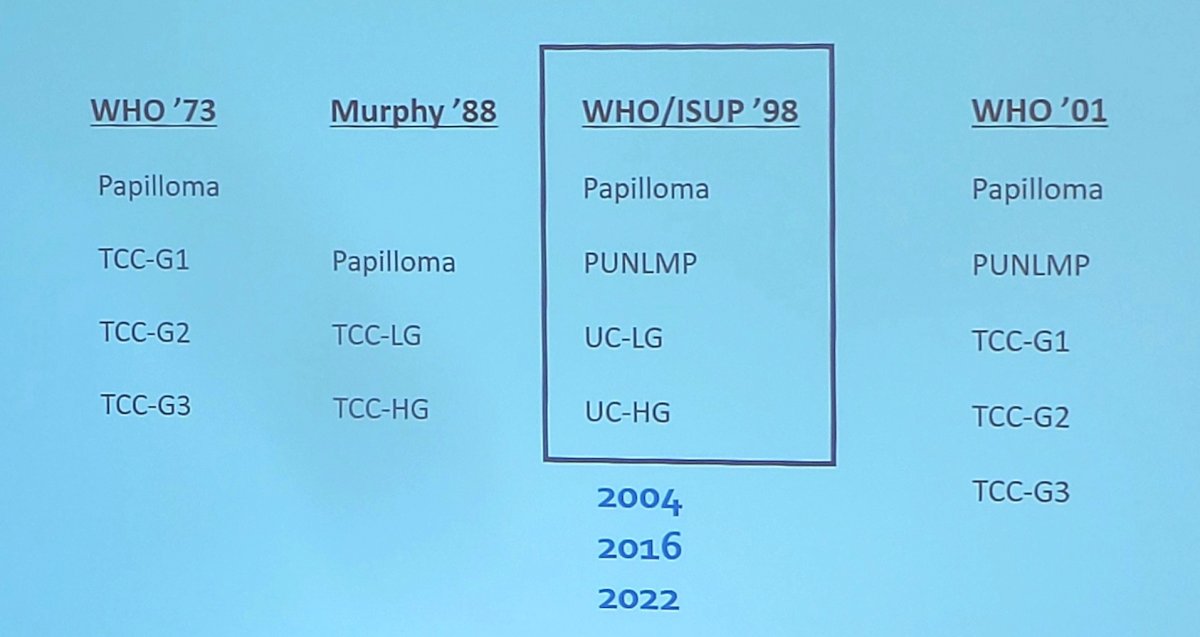
Dr. Al-Ahmadie notes that historical studies using the 2004 WHO/ISUP classification are quite good at predicting recurrence, progression, and cancer specific mortality of non muscle invasive bladder cancer. To date, there are multiple classification schemas for grading urothelial carcinoma:
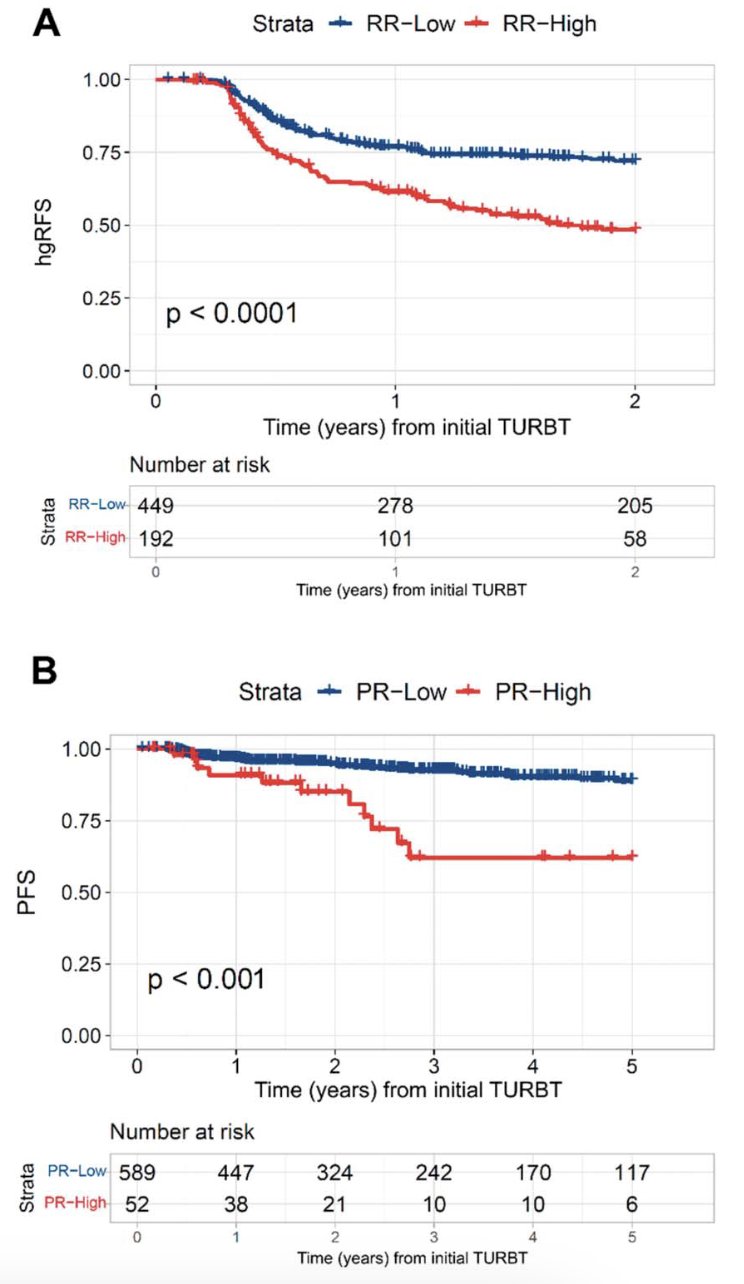
Dr. Al-Ahmadie notes that several studies have assessed sub-staging and quantification of lamina propria invasion, and more recently, two studies have assessed artificial intelligence applications of image analysis. Jansen et al.2 noted that automated classification correctly graded 76% of the low grade cancers and 71% of the high grade cancers compared to consensus reading by pathologists. Lotan et al.3 assessed 944 cases (development: 303, validation: 641) and found that in the validation cohort, “high recurrence risk” cases had inferior high-grade recurrence free survival versus “low recurrence risk” cases (HR 2.08, p < 0.0001). Moreover, “high progression risk” patients had poorer progression free survival (HR 3.87, p < 0.001) and higher risk of cystectomy (HR 3.35, p < 0.0001) than “low progression risk” cases:
Dr. Al-Ahmadie concluded his portion of the debate with the following concluding statements:
- Histologic classification (H&E, IHC) is time tested, practical, and cheap
- Histology provides micro-anatomy, reflective of underlying biology
- H&E-based classification can be flexible and adaptable
- It correlates with many molecular subtypes (luminal, basal/squamous, neuronal/neuroendocrine-like, mesenchymal, infiltrating, etc)
- It can be maximized by current (and future) image analysis/computational pathology/artificial intelligence tools
The debate concluded by highlighting the pre- and post-debate answers to the polling question “Is there a role for artificial intelligence informed non muscle invasive bladder cancer risk stratification in 2025?”
- Clinical artificial intelligence risk stratification only
- Pre-debate: 3%
- Post-debate: 6%
- Pathological risk stratification only
- Pre-debate: 21%
- Post-debate: 10%
- Both clinical and pathological artificial intelligence risk stratification
- Pre-debate: 39%
- Post-debate: 50%
- Neither is ready for primetime
- Pre-debate: 37%
- Post-debate: 34%
Moderated by: Patrick Hensley, University of Kentucky, Lexington, KY
Presented by:
- Hikmat Al-Ahmadie, Memorial Sloan Kettering Cancer Center, New York, NY
- Alexandre Zlotta, Mount Sinai Hospital, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, NV.
Related content: AI Risk Calculator Outperforms EAU Models for Bladder Cancer Prognosis - Alexandre Zlotta
Artificial Intelligence and Machine Learning in Bladder Cancer Pathology and Clinical Decision-Making - Hikmat Al-Ahmadie & Alexandre Zlotta
References:
- Villegas E, Lajkosz K, Din S, et al. Long-term recurrence risk, metastatic potential, and length of cystoscopic surveillance of low-grade nonmuscle-invasive bladder cancer. J Urol. 2025;213:295-303.
- Jansen I, Lucas M, Bosschieter J, et al. Automated detection and grading of non-muscle-invasive urothelial cell carcinoma of the bladder. Am J Pathol. 2020 Jul;190(7):1483-1490.
- Lotan Y, Krishna V, Abuzeid WM, et al. Predicting response to intravesical Bacillus Calmette-Guerin in high-risk nonmuscle-invasive bladder cancer using an artificial intelligence-powered pathology assay: Development and validation in an International 12-center cohort. J Urol. 2025 Feb;213(2):192-204.