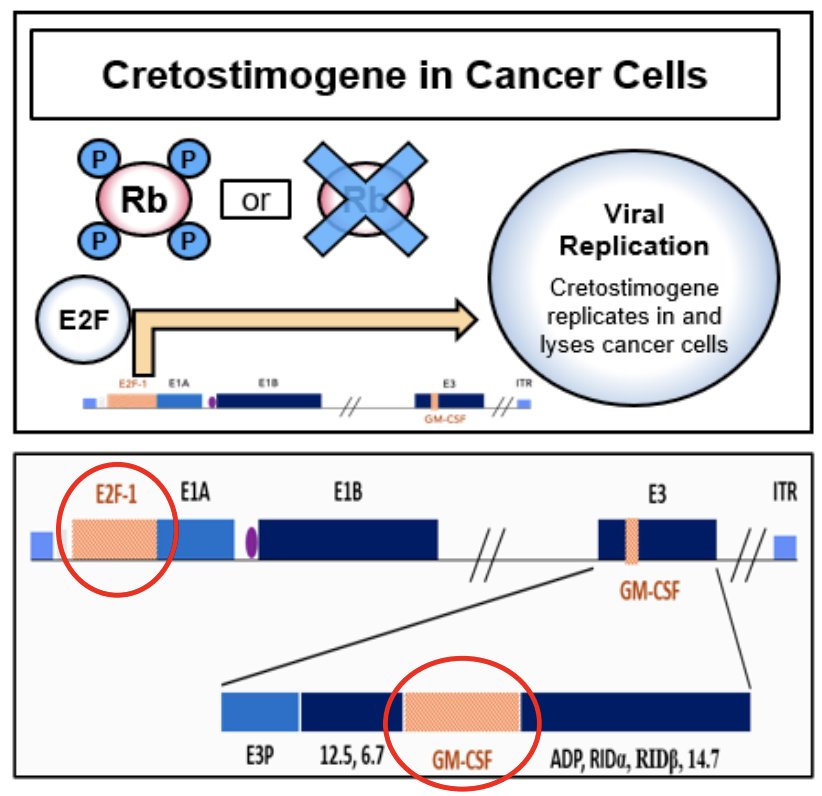
(UroToday.com) The 2025 AUA annual meeting featured a bladder cancer clinical trials in progress session and a presentation by Dr. Max Kates discussing PIVOT-006, a phase 3, randomized study of adjuvant intravesical cretostimogene grenadenorepvec versus surveillance for the treatment of intermediate-risk non-muscle invasive bladder cancer (NMIBC). Cretostimogene grenadenorepvec is an oncolytic immunotherapy designed to selectively replicate in bladder cancer cells with Rb-E2F pathway alterations, commonly found in high-risk BCG-unresponsive NMIBC. In addition, cretostimogene also expresses GM-CSF adding to local and systemic cancer control:
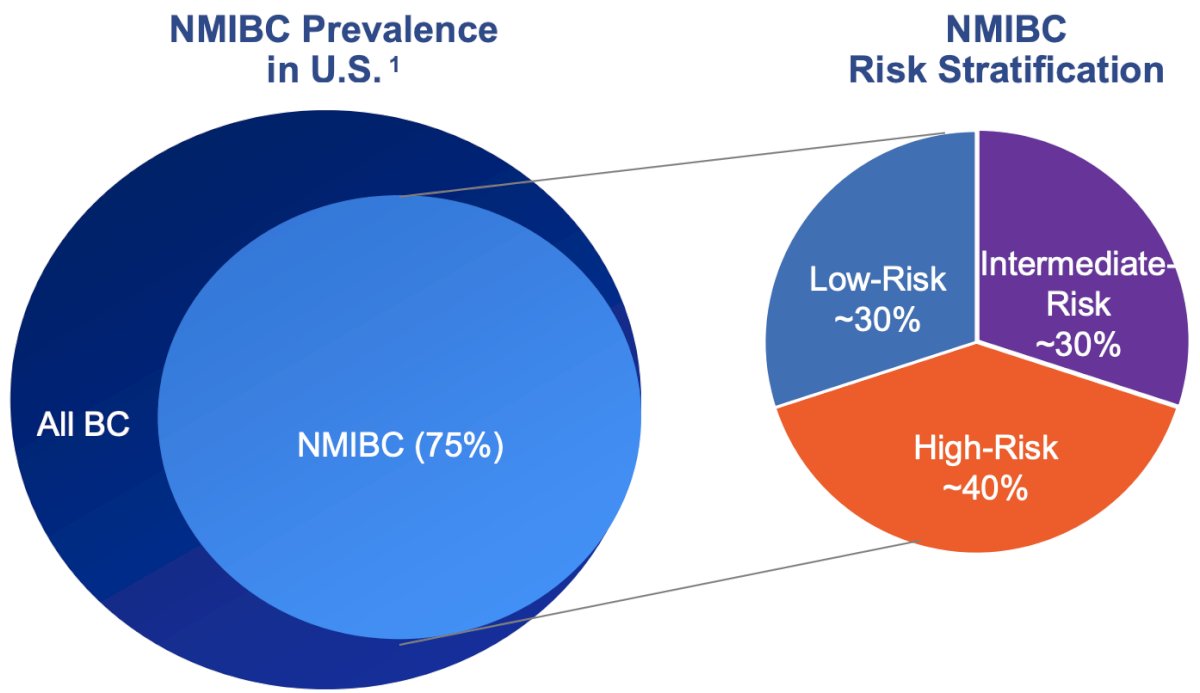
There is a significant unmet need with a high prevalence of intermediate risk non muscle invasive bladder cancer in the United States. Intermediate risk disease has a high risk of recurrence (50%-70%), but low risk of progression (<5%). Thus, it is a common, costly, and chronic disease, often requiring multiple resections and placing patients at risk from multiple anesthetics/surgeries:
The NCCN Bladder Cancer Guidelines recommend adjuvant intravesical therapy or surveillance for patients diagnosed with intermediate risk NMIBC. Despite this, up to 30%-60% of patients will recur and there is a general lack of level 1 evidence in the management of intermediate risk NMIBC. As a result, there is both a knowledge gap and an unmet medical need for improved therapies in the adjuvant setting of intermediate risk NMIBC.
Work presented at EAU 2024 by Dr. Contieri demonstrated that the IBCG intermediate non muscle invasive bladder cancer scoring system predicts the need for intervention for patients on active surveillance: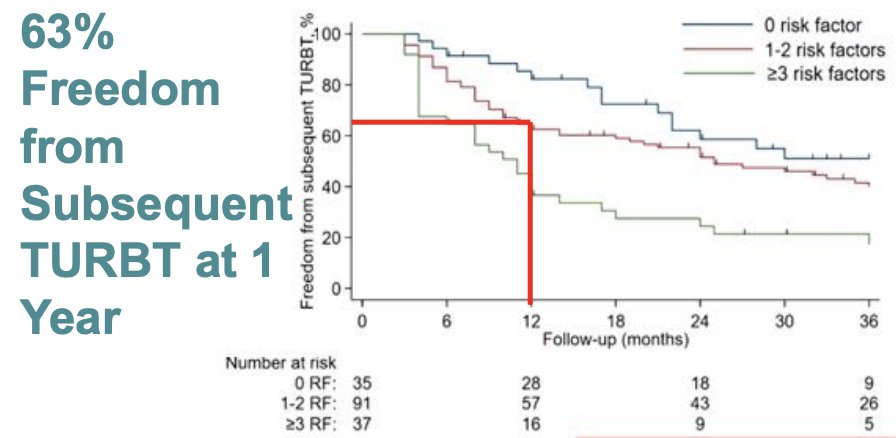
PIVOT-006 is one of the first adjuvant randomized clinical trials in intermediate risk non muscle invasive bladder cancer. Surveillance as a comparator offers several advantages, including:
- Reflecting the true effect size of adjuvant therapy
- Underscoring the natural history of the disease state
- Enabling efficient and streamlined clinical trial execution
Eligibility criteria for PIVOT-006 include:
- Histologically confirmed intermediate risk NMIBC diagnosis within 90 days of randomization, as defined by AUA/SUO Guidelines
- Age ≥18 years
- ECOG performance status of 0-2
- Absence of nodal or metastatic disease at screening
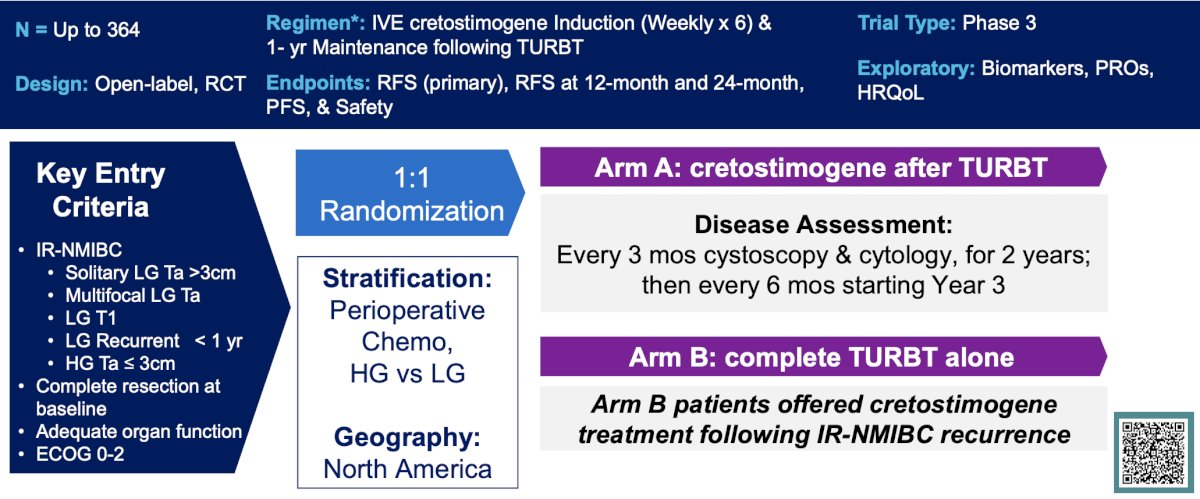
Stratification factors include receipt of single-dose perioperative chemotherapy and tumor grade. Patients (~n = 364) will be randomized 1:1 to receive intravesical cretostimogene (Cohort 1) adjuvant to TURBT or surveillance (Cohort 2). Participants in Cohort 2 will be eligible to receive intravesical cretostimogene if recurrence with intermediate risk NMIBC is noted:
Exclusion criteria include:
- Current or prior evidence of high risk non muscle invasive bladder cancer defined as:
- HG T1
- HG Ta > 3 cm that is recurrent or multifocal
- Any CIS
- Any variant histology
- Any high grade prostatic urethral involvement
- Any lymphovascular invasion
- Any BCG treatment failure in high grade patients
- Low risk non muscle invasive bladder: a low grade solitary, Ta <= 3 cm lesion that has recurred more than 12 months after a previous intermediate risk non muscle invasive bladder cancer diagnosis
- Has intermediate risk non muscle invasive bladder cancer that cannot be completely resected
- Has a history of muscle invasive bladder cancer, nodal or metastatic disease
Efficacy assessments will be visits, cystoscopies, biopsies for cause, and cytology every 3 months for the first 2 years, and every 6 months for the third year. Imaging will be every 12 months, and mapping biopsies/imaging will be done for isolated positive cytology (local and central pathology review). The recurrence free assessment will be done for recurrence or progression in the bladder, as well as the upper tract or prostatic urethra.
PIVOT-006 is an SUO-CTC trial, with a diverse representation across LUGPA and academic sites. First enrollments were in January 2024 and is ahead of the expected enrollment period. PIVOT-006 anticipates completing enrollment in late 2025-early 2026.
Presented by: Max Kates, MD, Director, Bladder Cancer Program, Associate Professor of Urology, Johns Hopkins Medicine, Baltimore, MDWritten by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, NV.
Related content: PIVOT-006 Trial: Cretostimogene Grenadenorepvec for Intermediate-Risk Non-Muscle Invasive Bladder Cancer - Max Kates