(UroToday.com) The American Urological Association's 2025 Annual Meeting, in Las Vegas, Nevada, was host to the Society of Urologic Oncology (SUO) Session. Drs. Sima Porten, Stephen Boorjian, Vikram Narayan, and Jeffrey Holzbeierlein participated in the case discussions in NMIBC: Sequencing Therapy after BCG Failures.
Case # 1Dr. Porten began by presenting the case of a 68-year-old man with high-grade Ta (HGTa) and carcinoma in situ (CIS), involving three tumors approximately 2 cm each. He had previously completed a full-dose BCG induction course (six instillations). A follow-up cystoscopy appeared suspicious, prompting a blue light TURBT. During the procedure, Dr. Porten resected raised patches, biopsied an additional blue light–positive area, and performed a prostatic urethra biopsy. Pathology revealed multifocal CIS in the bladder, with no involvement of the prostatic urethra. His past medical history included hypertension and mild diabetes mellitus; he was a former smoker. Three questions were asked of the panel:
- How would you classify this patient and what is the next best treatment option? Alternatives?
- What if you did not have enough BCG?
- Would you consider treating this patient differently at diagnosis?
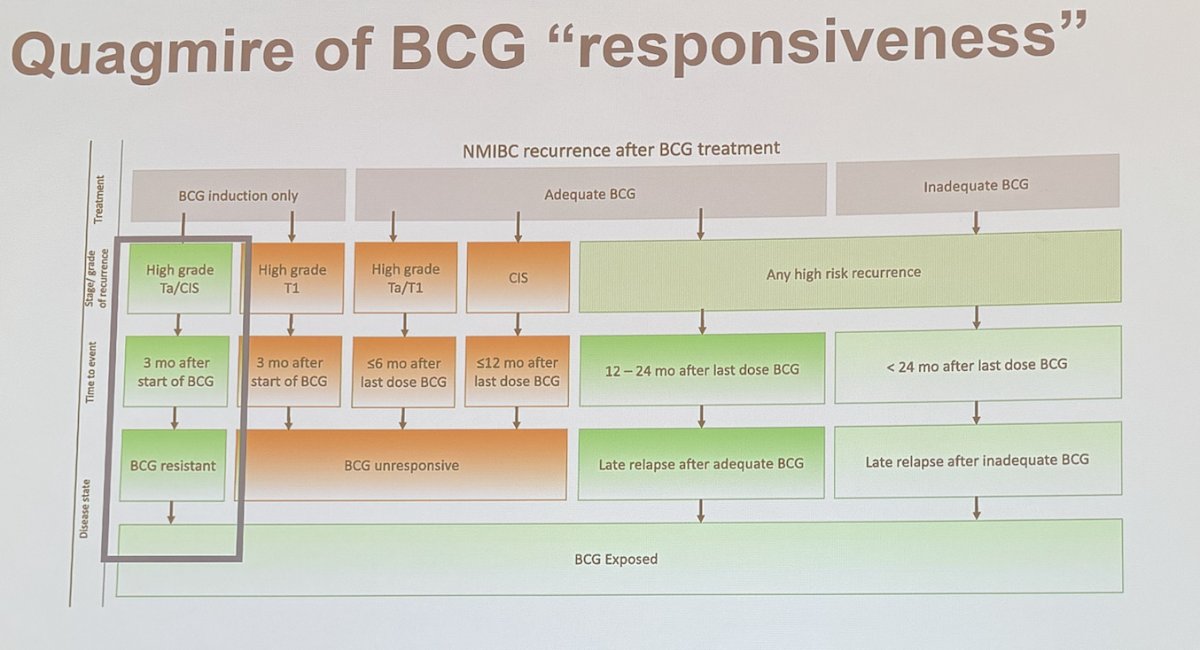
Dr. Boorjian answered the first question by emphasizing that this patient should not yet be classified as BCG-unresponsive, as he has only completed one induction course, and it has been less than six months since treatment. In patients with CIS, the definition of BCG unresponsiveness typically requires at least 12 months, as illustrated below. He also highlighted the ongoing challenge ("quagmire") of defining BCG responsiveness. Treatment options in this case could include a second induction course followed by maintenance therapy. Radical cystectomy (RC) remains a definitive option for patients with high-risk NMIBC.
Dr. Boorjian also discussed the emerging role of artificial intelligence (AI) combined with biomarkers to help predict response to BCG reinduction in patients previously exposed to BCG. He highlighted the Vesta test (developed by Valar Labs), which identifies the risk of BCG unresponsiveness, risk of progression, and risk of recurrence. He noted that this test could potentially serve as a biomarker to identify patients at higher risk of failing BCG therapy.
He noted that for this specific case, he would proceed with a second induction course of BCG.
Dr. Holzbeierlein mentioned that he is a strong advocate for thorough resection, particularly emphasizing the importance of resecting areas of CIS. He noted that peripheral data suggest blue light cystoscopy (BLC) improves outcomes for CIS, and many who use BLC routinely find it extremely valuable. He highlighted that approximately 80% of patients labeled as BCG-unresponsive are actually cases of poor initial resection, where CIS was missed.
When asked about managing BCG shortages, Dr. Holzbeierlein acknowledged the challenge and referenced SUO-published guidelines on the topic. Key strategies include prioritizing BCG use for high-grade disease (not low-grade), using split doses, employing half-dose or third-dose BCG, giving induction plus one course of maintenance, and then switching to gemcitabine-docetaxel (Gem/Doce) maintenance if shortages persist. He also emphasized the importance of enrolling patients in clinical trials when possible.
Dr. Narayan was asked how he would approach treating this patient differently. He emphasized that in cases of first recurrence with high-grade disease and CIS, there is an opportunity to incorporate biomarkers early in the treatment course. He discussed the use of AI-based pathology tests upfront to help guide decisions between BCG and gemcitabine-docetaxel (Gem/Doce), especially if a biomarker signal suggests resistance to therapy. Dr. Narayan also mentioned urinary-based tests highlighted by Dr. Josh Meeks, such as Oncuria Predict (Diacarta), a multiplex bead-based urinary immunoassay that measures 10 cancer-associated biomarkers (MMP9, VEGFA, CA9, SDC1, PAI1, APOE, A1AT, ANG, and MMP10). Oncuria Predict can discriminate patients unlikely to respond to intravesical BCG therapy (n=64). Additionally, he mentioned UroAmp (Convergent Genomics), a urinary comprehensive genomic profiling test that evaluates pre- and post-treatment mutation burden to assess the risk of recurrence after intravesical therapy.
Dr. Porten continued the case discussion, noting that the patient underwent a repeat induction course (six instillations at half dose) and completed one additional maintenance course, totaling 15 instillations. On follow-up, cystoscopy revealed a 3 cm papillary tumor. Cytology was performed, and a blue light TURBT was carried out, with complete resection of the tumor, biopsy of an additional blue light–positive area, and a prostatic urethra biopsy. A CT urogram showed no evidence of disease (NED). Pathology revealed high-grade Ta (HGTa) disease with no lymphovascular invasion (LVI), muscle present, and concurrent CIS in the bladder (blue light positive). The prostatic urethra remained clear. Importantly, bladder function was preserved. At this point, the patient was classified as having BCG-unresponsive disease. Dr. Porten highlighted the available treatment options for BCG-unresponsive disease, as illustrated below.
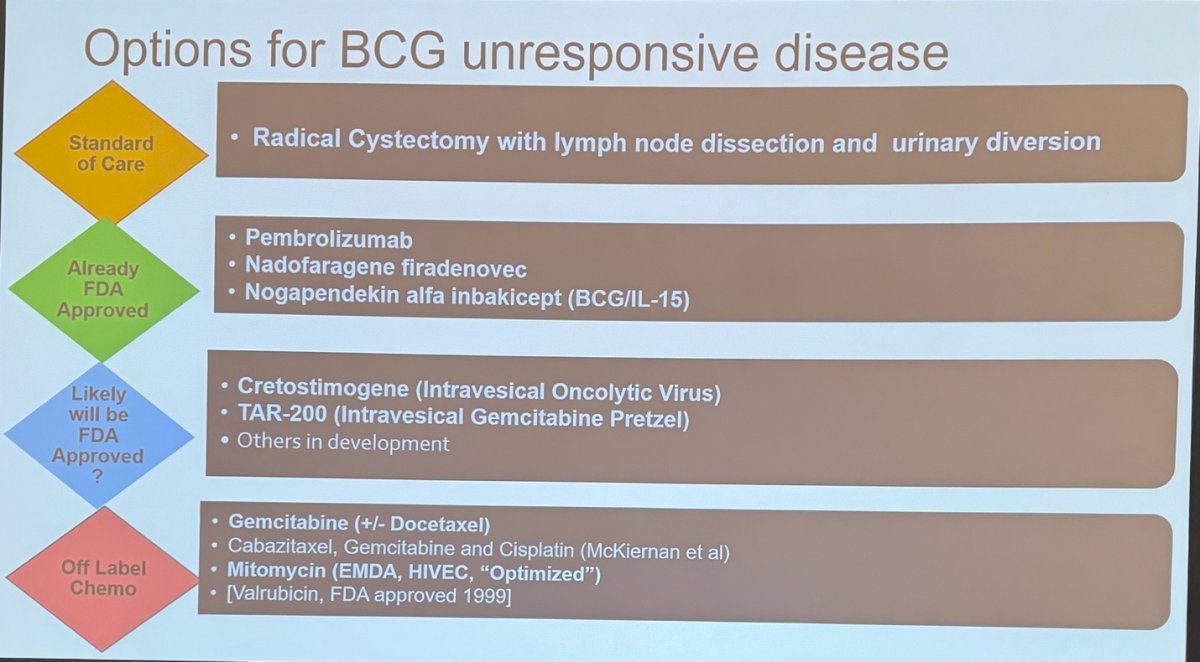
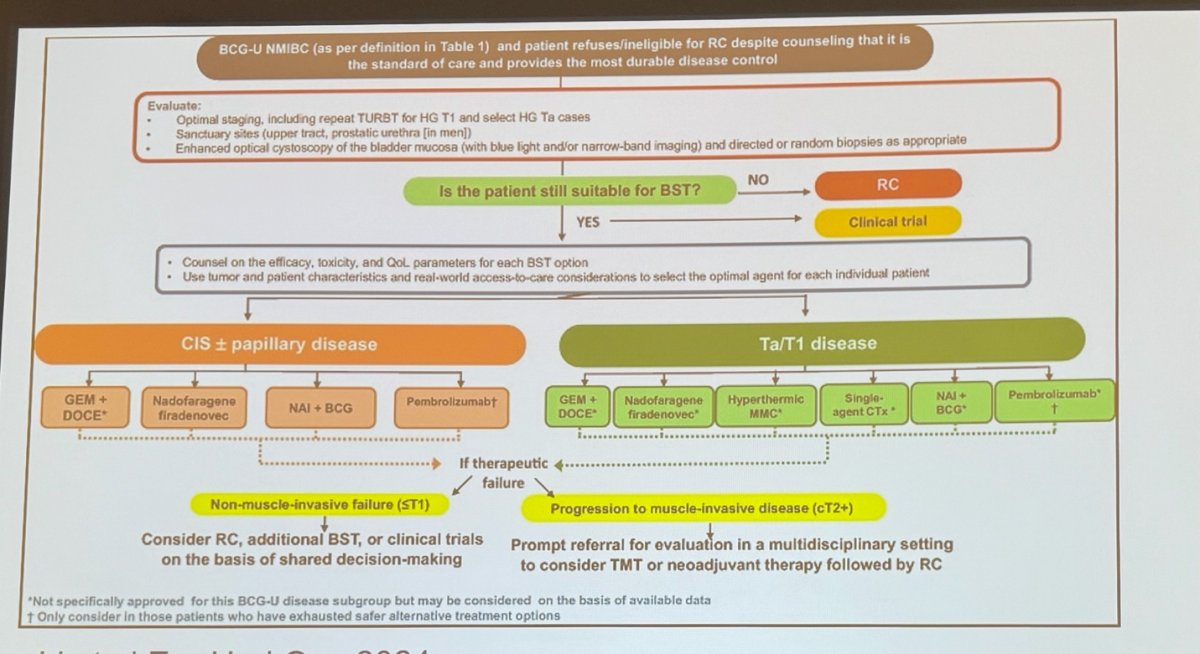
Dr. Narayan discussed the role of RC in this patient. He noted that other FDA-approved options for BCG-unresponsive disease include pembrolizumab, nadofaragene firadenovec, and nogapendekin alfa inbakicept. He also mentioned that gemcitabine-docetaxel (Gem/Doce) can be used off-label; it is generally well tolerated and can be effective, although data on long-term durability are limited. For patients with T1 disease, he emphasized that RC remains his preferred option. He noted that while many of the available alternatives offer potential, there is lingering concern about their long-term durability and outcomes. He proposed to use the algorithm below to improve treatment decision-making for these patients:
Dr. Boorjian emphasized the importance of shared decision-making, considering both the disease standpoint and the patient standpoint. He noted that the broad umbrella term of labeling all these cases as "BCG-unresponsive" can obscure important nuances, especially since patients with T1 disease within this cohort have the worst prognosis, a key disease factor that should drive treatment decisions. He also stressed the importance of evaluating the patient's current bladder function and quality of life (QOL) during discussions. Dr. Boorjian highlighted the ongoing CISTO trial (led by Dr. John Gore), which is examining bladder-sparing therapy (BST) versus RC with the primary endpoint being bladder function; this study suggests there may be no major difference in functional outcomes between RC and BST. He emphasized that these factors must be part of the conversation with patients when counseling on next steps.
Dr. Holzbeierlein discussed several patient factors he would consider important in decision-making. He noted that the presence of lymphovascular invasion (LVI) would be a significant risk factor for disease progression, as would T1 disease. He also mentioned variant histology, acknowledging that it remains unclear which histologic variants may respond better to therapy.
Dr. Holzbeierlein briefly touched on bladder preservation strategies, noting the growing role of chemoradiation. He referenced the RTOG 0926 trial, which evaluated the use of BCG combined with external beam radiation therapy (EBRT) as a bladder preservation approach in this patient population.1

They concluded the case with the following comments:
- The patient strongly desired bladder preservation. A repeat TURBT confirmed CIS with clear muscle.
- He underwent gemcitabine/docetaxel (Gem/Doce) induction (six instillations) followed by monthly maintenance for six months, but subsequently developed another high-grade Ta (HGTa) recurrence.
- Ultimately, the patient underwent radical cystoprostatectomy with lymph node dissection (LND) and neobladder reconstruction. Final pathology revealed pTis disease with focal high-grade T1 and LVI, with negative surgical margins and 0/20 positive lymph nodes.
Dr. Porten presented the case of a 70-year-old female with multifocal high-grade Ta (HGTa) disease who had completed full-dose BCG induction (six instillations) followed by three maintenance instillations at half-dose (15 total instillations). A CT urogram performed at diagnosis showed no evidence of upper tract disease or lymphadenopathy. On surveillance cystoscopy, multiple (at least 10) papillary tumors were identified scattered throughout the bladder. Urine cytology was atypical urothelial cells (AUC), Paris Class III. The patient was noted to be an active smoker. On TURBT, they resected 12 tumors, 1-2 cm each, and pathology revealed HGTa with muscle clear. The patient had a very poor bladder function post-TURBT.
Dr Porten asked the panelists the following questions:
- In this patient with BCG unresponsive disease-HGTa (papillary only), what are the options?
- How do you mitigate the desire for bladder preservation despite poor function?
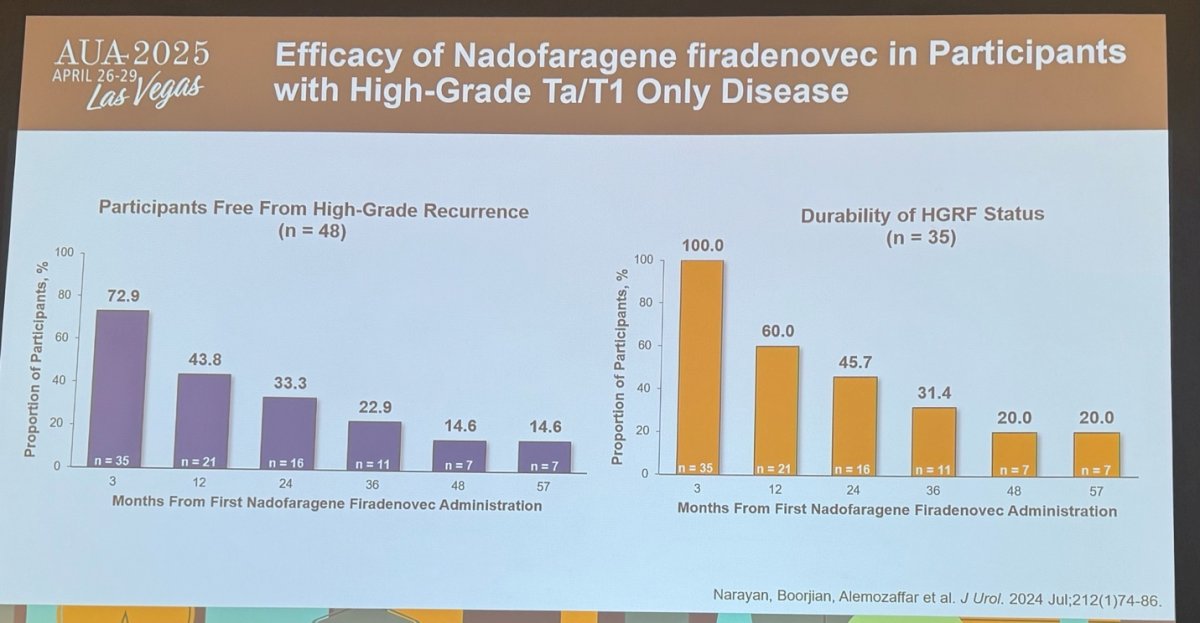
Dr. Narayan began by highlighting that papillary-only disease is very different from cases with CIS, as CIS represents a field defect throughout the bladder. In CIS, intravesical therapy (like BCG) is the primary treatment, whereas in papillary disease, surgery is the primary treatment, and systemic therapy serves an adjuvant role. For this particular patient, Dr. Narayan stated that his preference would be nadofaragene firadenovec, citing data showing good durability, especially compared to CIS outcomes as shown below. He also mentioned the potential future role of the gemcitabine "pretzel" (TAR-200 device), which is likely to become available soon.
The patient was started on pembrolizumab monotherapy and remained with no evidence of disease (NED) for nine months. Subsequent cystoscopy revealed one papillary tumor and four erythematous areas, with a positive urine cytology. She underwent another TURBT, during which the posterior papillary tumor was resected and targeted as well as random biopsies were taken. Pathology showed high-grade Ta (HGTa) disease with concomitant CIS. The patient was also experiencing moderate urinary symptoms.
Dr. Boorjian discussed that although the patient had previously tried pembrolizumab, she now strongly desired to preserve her bladder. He outlined several treatment options, noting that nadofaragene firadenovec is favorable due to its tolerable side-effect profile and convenient dosing schedule. He also mentioned that the NAI 803 agent (nogapendekin alfa inbakicept) and Gem/Doce are additional options. He highlighted that the use of suppositories, “Valium suppository" has shown a significant increase in bladder retention rates and a decrease in recurrence rates.
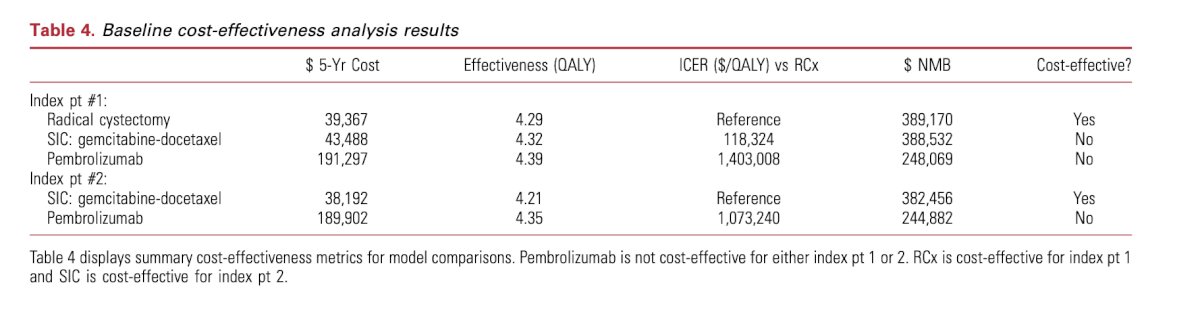
Dr. Boorjian then transitioned to discussing the important issue of financial toxicity, noting that the cost of therapy is a critical factor that has not been fully addressed in the field. He presented a cost-effectiveness study comparing pembrolizumab versus BCG, which showed that the incremental cost-effectiveness ratio (ICER) for Gem/Doce was ten times lower than that for pembrolizumab, as shown below. He emphasized that cost considerations should be factored into treatment decisions, particularly at the health care system level, as they are a critical factor in ensuring sustainable care.2
Dr. Porten continued the case discussion, noting that the patient received one year of treatment with nadofaragene firadenovec (four instillations). On surveillance cystoscopy, a few erythematous patches and a 0.5 cm papillary tumor were identified. Urine cytology was positive for high-grade urothelial carcinoma. A CT urogram showed no evidence of disease, and pathology from TURBT revealed high-grade Ta (HGTa) disease and CIS in 2 of 6 biopsy samples. The patient reported only very mild urinary symptoms at this stage.
Dr. Holzbeierlein discussed the challenges in managing this patient with BCG-unresponsive disease who had already received pembrolizumab and nadofaragene firadenovec. He emphasized the need to consider the next line of therapy and highlighted concerns about the patient's quality of life (QOL), noting it was unusual that her urinary symptoms had improved given the significant tumor burden. He pointed out that many patients in this situation experience very poor QOL, often needing to use the toilet constantly, and questioned, "What are we saving this bladder for?" He stressed the importance of evaluating the upper urinary tract as part of ongoing management.
From a personal perspective, Dr. Holzbeierlein noted that all treatments the patient had received so far had been immunotherapy-based. Given this, he suggested that trying intravesical chemotherapy, specifically Gem/Doce, would be reasonable.
Dr. Porten concluded the case by noting that the patient was started on a combination of BCG and nogapendekin alfa inbakicept (NAI-803) and is currently on maintenance therapy with half-dose BCG. Her first cystoscopy post-induction showed no recurrence, It remains unlikely that the patient will ever agree to bladder removal.
Presented by:- Sima Porten MD, MPH, Associate Professor, Urologic Oncologist, Department of Urology, UCSF, San Francisco, CA
- Stephen Boorjian MD, Carl Rosen Professor and Chair of the Department of Urology, Director of the Urologic Oncology Fellowship, Mayo Clinic, Rochester, MN
- Vikram Narayan MD, Assistant Professor of Urology, Emory School of Medicine. Atlanta GA.
- Jeffrey Holzbeierlein MD, FACS, Physician-in-Chief, Associate Professor of Urology, and Research Team Leader, The University of Kansas Cancer Center, Kansas City, KS
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
References:- Efstathiou JA, Gillies E, Feng FY, et al. Trimodality bladder-sparing treatment for high-grade T1 non-muscle-invasive bladder cancer: Results from NRG Oncology RTOG 0926. J Clin Oncol. 2024;42(1):49-59. doi:10.1200/JCO.23.02510
- Wymer KM, Sharma V, Saigal CS, Chamie K, Litwin MS, Packiam VT, Mossanen M, Pagliaro LC, Borah BJ, Boorjian SA. Cost-Effectiveness Analysis of Pembrolizumab for Bacillus Calmette-Guérin-Unresponsive Carcinoma In Situ of the Bladder. J Urol. 2021 May;205(5):1326-1335. doi: 10.1097/JU.0000000000001515. Epub 2020 Dec 21. PMID: 33347775.