(UroToday.com) The American Urological Association's 2025 Annual Meeting, in Las Vegas, Nevada, was host to the Society of Urologic Oncology (SUO) Session. Dr. Joshua Meeks delivered the State-of-the-Art Lecture on Urothelial Markers
Dr. Meeks began his presentation by highlighting that biomarkers for urothelial cancer (UC) can be identified in tissue, urine, or blood. He outlined the key roles of biomarkers in UC management, which include guiding treatment intensification, supporting treatment de-intensification, and enabling precision targeting.
Dr. Meeks highlighted that DNA damage response (DDR) alterations play a significant role in predicting chemotherapy response in UC. Specifically, mutations in genes such as ATM, ERCC2, RB1, and FANCC have been associated with improved progression-free survival (PFS), with an odds ratio of 5.36 (95% CI: 2.05–14.02; two-sided p = 0.0006). He also discussed the use of MSK-IMPACT®, an integrated mutation profiling platform developed at Memorial Sloan Kettering (MSK), for identifying actionable targets in urothelial cancer. Genes commonly associated with chemotherapy sensitivity in this context include ATM, ERCC2, RB1, BRCA1/2, ATR, and FANCC.
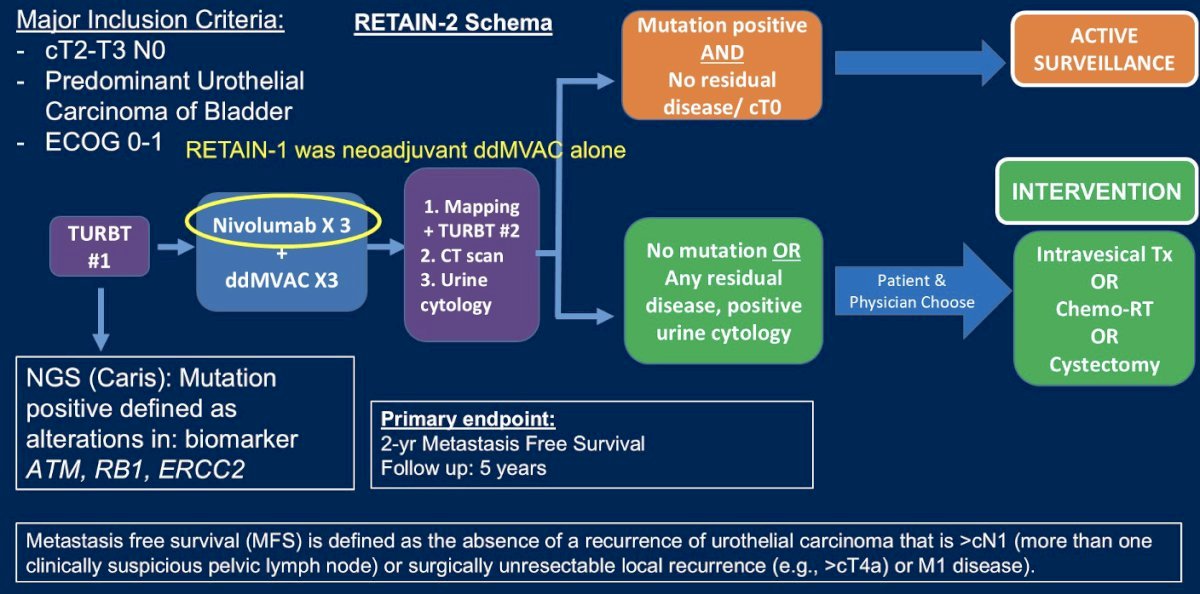
The RETAIN-2 trial is a phase II, multi-institutional trial in which patients with cT2-T3N0M0 MIBC, ECOG PS 0-1, and CrCl ≥50 mL/min received the combination of neoadjuvant dose-dense methotrexate, vinblastine, doxorubicin, and cisplatin (ddMVAC) plus nivolumab. Pre-NAC transurethral bladder resection (TURBT) specimens were sequenced for mutations (pathogenic or variant of unknown significance [VUS]) in ATM, ERCC2, or RB1. Patients with >1 mutation and clinical complete response (cCR) post-NAC (based on restaging TUR, urine cytology and CT imaging) initiated active surveillance (AS). The remaining patients (i.e., those without a mutation and/or no clinical complete response) underwent bladder-directed therapy: intravesical therapy (< cT2 post-NAC), chemoradiotherapy, or radical cystectomy. The study design is shown below.
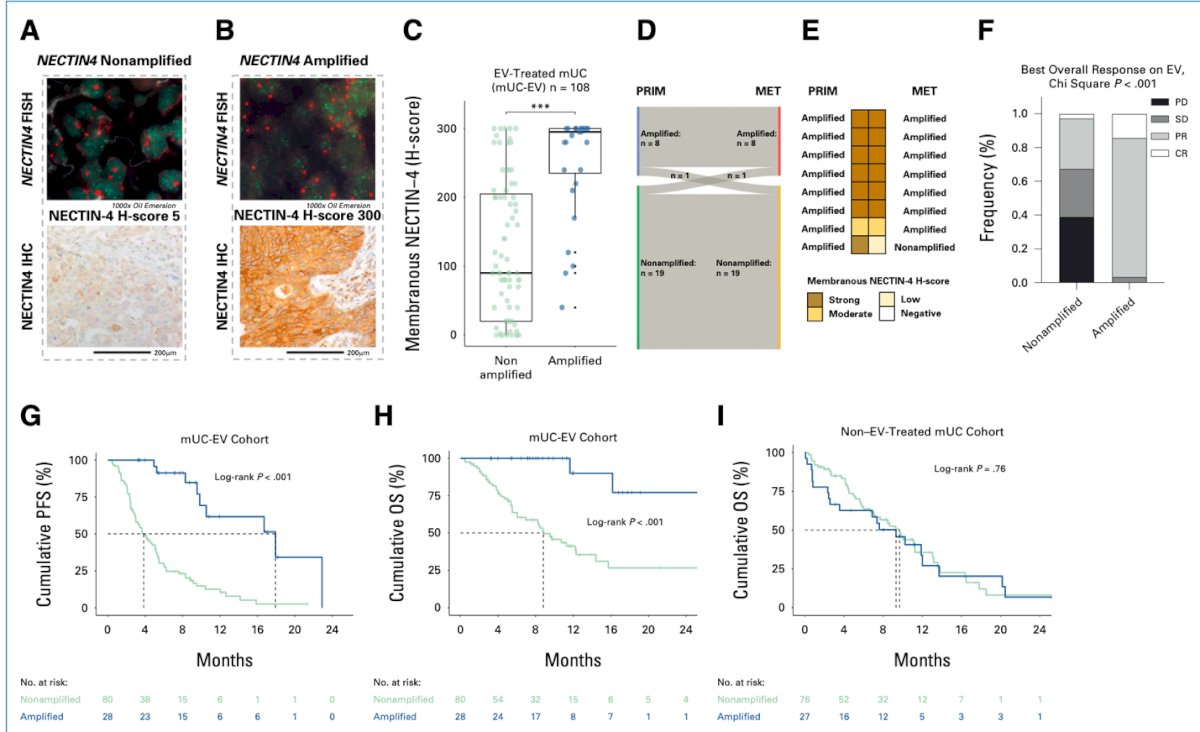
Moreover, Dr. Meeks highlighted the role of membranous Nectin-4 in urothelial cancer. NECTIN4 amplification is a frequent genomic event, observed in approximately 17% of cases in the TCGA muscle-invasive bladder cancer (MIBC) dataset and about 26% in metastatic urothelial cancer (mUC) cohorts. In patients treated with enfortumab vedotin (EV) for metastatic disease (mUC-EV), NECTIN4 amplification represents a stable genomic alteration during metastatic progression and is associated with enhanced membranous NECTIN4 protein expression. Importantly, NECTIN4 amplifications have been linked to objective responses to EV, with a hazard ratio (HR) of 0.08 (95% CI: 0.02–9.34).1
Dr. Meeks also discussed the VESTA study, which used AI-based pathology to predict BCG response. This study included 944 cases (303 in the discovery cohort and 641 in the validation cohort) and was conducted across multiple institutions. AI models developed for predicting BCG response outperformed traditional clinical models. Further validation in the SWOG S1602 trial confirmed these findings: in the validation cohort, patients classified as "high recurrence risk" had significantly inferior high-grade recurrence-free survival compared to "low recurrence risk" patients (HR 2.08, P < .0001). Similarly, "high progression risk" patients experienced poorer progression-free survival (HR 3.87, P < .001) compared to "low progression risk" patients, as illustrated below.2

Dr. Meeks highlighted the importance of CxBladder, a widely available and clinically validated urine assay. He noted that CxBladder has been endorsed by the AUA guidelines, which state that in appropriately counseled intermediate-risk patients who wish to avoid cystoscopy and are willing to accept the risk of forgoing direct visual inspection of the bladder urothelium clinicians may offer urine cytology or validated urine-based tumor markers to aid in decision-making regarding the need for cystoscopy.
Similarly, Dr. Meeks discussed the SWOG S1605 study, a single-arm Phase II registration trial that enrolled 135 patients with histologically confirmed BCG-unresponsive high-risk NMIBC. Patients received atezolizumab (1200 mg IV) every three weeks for one year. In a substudy conducted at Vancouver, investigators utilized the UroAmp test — a non-invasive genomic urine assay designed to detect, monitor, and predict the risk of urothelial cancer recurrence or progression. UroAmp MRD testing was performed at baseline and again three months after initiation of atezolizumab to assess early molecular response and predict outcomes.
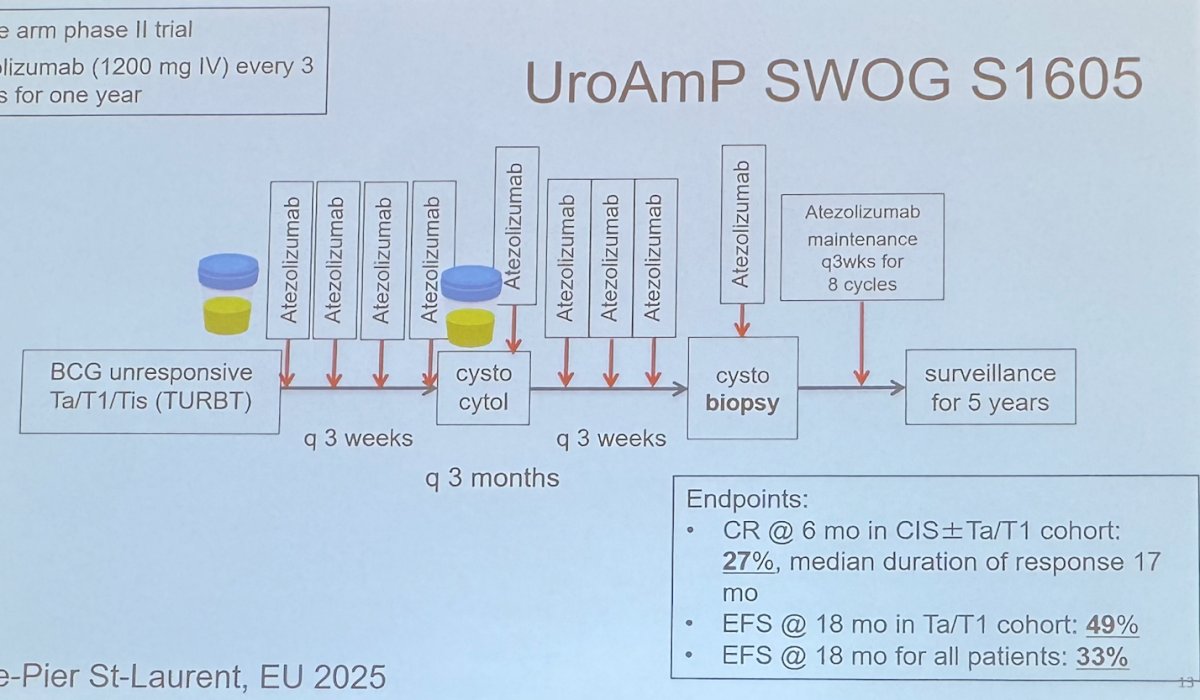
The investigators found a highly variable alteration count at baseline among patients. UroAmp status at baseline was associated with event-free survival (EFS) in the 89 patients analyzed. Patients with a positive UroAmp test at baseline had a 12-month EFS of 26%, compared to 67% among those with a negative UroAmp test.
The current limitations of urine-based biomarkers include issues with collection and storage (a processing problem) and challenges in managing the urothelial cancer (UC) field effect, which affects the signal-to-noise ratio and represents a computational problem. He emphasized that a major challenge remains determining how best to use urine biomarkers, particularly how to handle anticipatory positives situations that may be even more problematic than a positive FISH test. Dr. Meeks also highlighted the broader "cancer field" computational problem, noting that significant work will be needed to resolve these challenges moving forward.
Blood based biomarkersThe clinical applications of circulating tumor DNA (ctDNA) are expanding significantly. ctDNA can be used for early cancer detection, surveillance, detection of metastatic relapse, and assessing response to neoadjuvant therapy, among other applications. It is important to understand that minimal residual disease (MRD) refers to persistent cancer after treatment that remains undetectable by conventional imaging tools, representing occult metastatic disease. Tracking ctDNA dynamics allows for real-time assessment of disease burden and can help inform treatment decisions throughout the continuum of care.
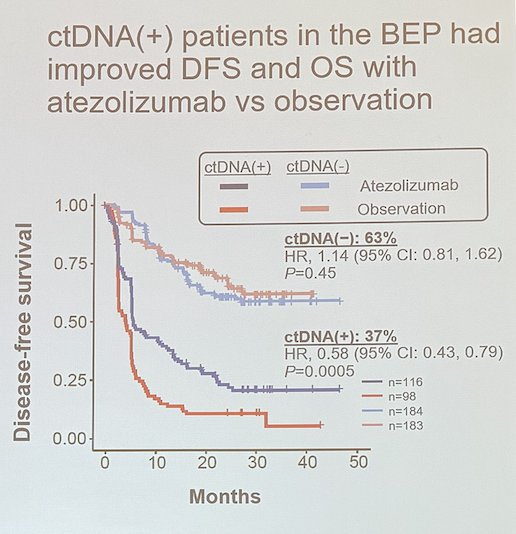
IMvigor010 was a randomized controlled trial (RCT) evaluating adjuvant atezolizumab in urothelial cancer. Although the trial was negative overall, it provided important insights: in a post-hoc analysis, patients who were ctDNA-positive at baseline (BEP) experienced improved disease-free survival (DFS) and overall survival (OS) with atezolizumab compared to observation.3
A study led by Dr. Sfakianos in New York evaluated 112 patients, including 53 with positive ctDNA before radical cystectomy (RC). The study demonstrated that detectable ctDNA prior to definitive therapy was predictive of nodal involvement, locally advanced disease, and disease recurrence in patients with bladder cancer. Precystectomy ctDNA burden, measured in mutant tumor molecules per milliliter (MTM/mL), was able to stratify patients into distinct risk groups with different oncologic outcomes. Given the high likelihood of rapid progression in patients with high-burden ctDNA (with a 3-month recurrence-free survival [RFS] of only 58.3%), the authors suggested that treatment intensification should be considered for these high-risk individuals.
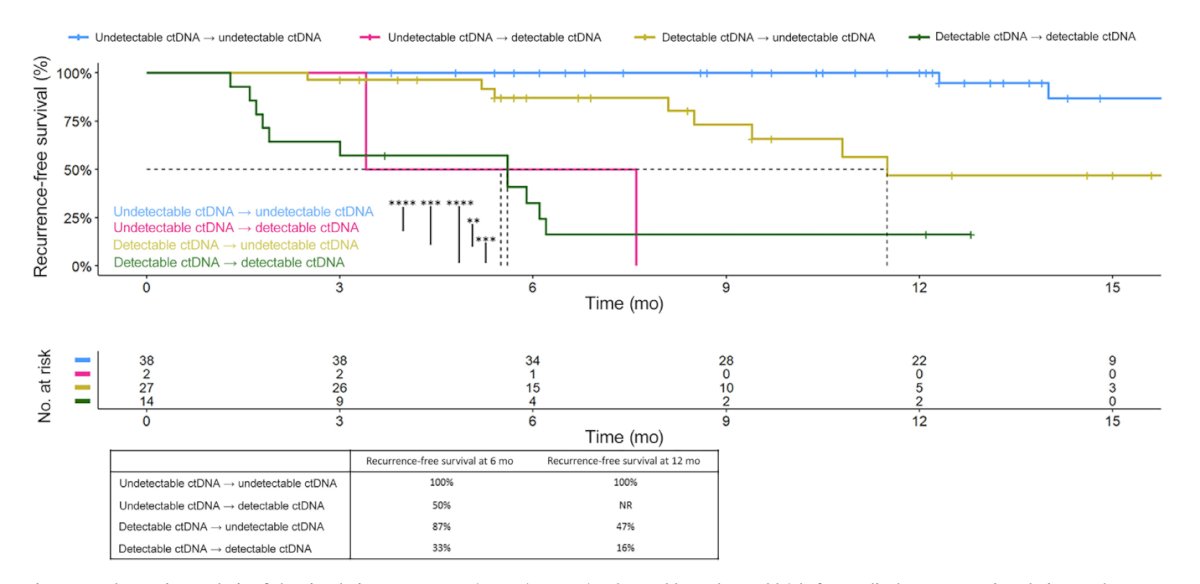
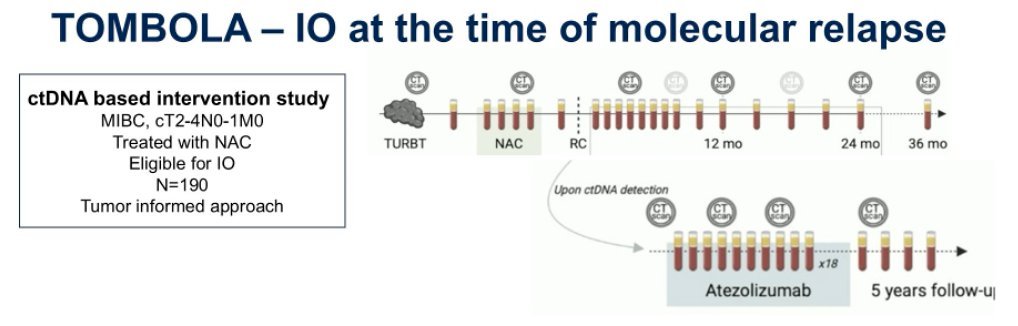
The TOMBOLA study is a ctDNA-based intervention trial evaluating the use of immunotherapy at the time of molecular relapse. It is enrolling patients with muscle-invasive bladder cancer (MIBC; cT2–T4N0–N1M0) who have received neoadjuvant chemotherapy (NAC) and are eligible for adjuvant immunotherapy. TOMBOLA is the first prospective trial using an integral biomarker-directed treatment change. Conducted across five centers in Denmark.
In the trial, patients with detectable ctDNA after cystectomy received atezolizumab for 12 months. Preliminary findings showed that 55% of ctDNA-positive patients converted to ctDNA-negative status and remained free of disease recurrence on imaging. Among ctDNA-negative patients, only 2 out of 66 experienced relapse. Additionally, imaging and ctDNA findings revealed that 10 out of 40 patients were ctDNA-positive but had negative imaging, whereas only 2 out of 40 had positive imaging but were ctDNA-negative.
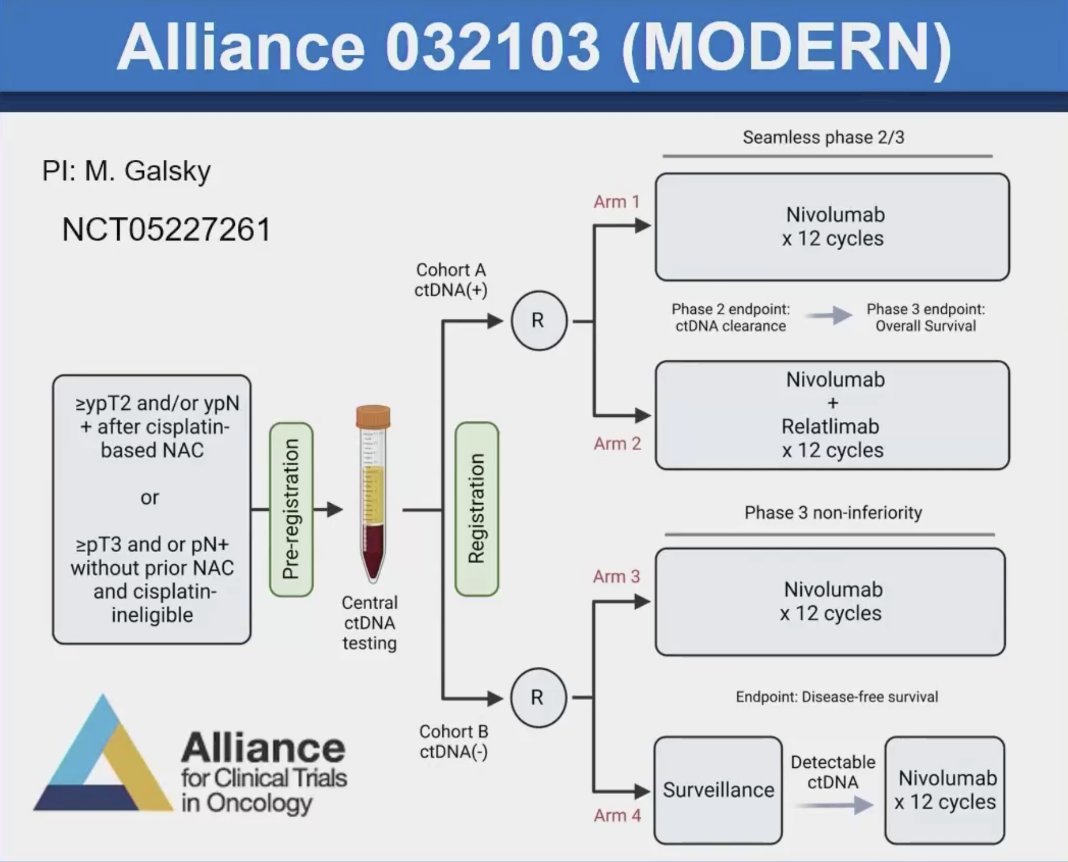
Dr. Meeks highlighted that the future is already taking shape with adaptive design trials using ctDNA as an integral biomarker, including studies such as IMvigor011 and MODERN.
Meeks highlighted that FGFR3 alterations are present in up to 30% of patients with non–muscle-invasive bladder cancer (NMIBC). He emphasized that FGFR3 is now considered a bona fide therapeutic target in NMIBC.
TAR-210 is a novel intravesical drug delivery system designed to provide local, continuous release of targeted therapy, including erdafitinib, directly within the bladder while minimizing systemic toxicity. The device is inserted via a dedicated urinary placement catheter and removed by cystoscopy; the entire procedure can be performed in the office setting and takes approximately 2–3 minutes.
In a study evaluating TAR-210 in patients with NMIBC harboring select FGFR alterations, 31 patients were evaluable for response. Results showed a 90% complete response (CR) rate, with 28 out of 31 patients achieving CR at week 12. Overall, 100% of patients achieved a clinical response (either CR or non-CR/non-progression). A consistent CR rate was observed across both dosing levels, and 86% (24 of 28) of CRs were ongoing at the time of clinical cutoff.

Dr. Meeks concluded his presentation with the following key messages:
- Urine biomarkers are evolving and continue to show promise.
- ctDNA is now available and can be used to identify high-risk patients, although it may not yet be ready to fully guide treatment decisions.
- AI-driven pathology is emerging and holds significant potential for the future.
- FGFR3 is a validated target in urothelial cancer, and precision therapy is becoming a reality.
Presented by: Joshua Meeks, MD, PhD, Associate Professor of Urology, Biochemistry and Molecular Genetics at the Northwestern University Feinberg School of Medicine and Section Chief of Robotic Surgery at the Jesse Brown VA Medical Center. Chicago, IL.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
References:
- Klümper N, Tran NK, Zschäbitz S, Hahn O, Büttner T, Roghmann F, Bolenz C, Zengerling F, Schwab C, Nagy D, Toma M, Kristiansen G, Heers H, Ivanyi P, Niegisch G, Grunewald CM, Darr C, Farid A, Schlack K, Abbas M, Aydogdu C, Casuscelli J, Mokry T, Mayr M, Niedersüß-Beke D, Rausch S, Dietrich D, Saal J, Ellinger J, Ritter M, Alajati A, Kuppe C, Meeks J, Vera Badillo FE, Nakauma-González JA, Boormans J, Junker K, Hartmann A, Grünwald V, Hölzel M, Eckstein M. NECTIN4 Amplification Is Frequent in Solid Tumors and Predicts Enfortumab Vedotin Response in Metastatic Urothelial Cancer. J Clin Oncol. 2024 Jul 10;42(20):2446-2455. doi: 10.1200/JCO.23.01983. Epub 2024 Apr 24. PMID: 38657187; PMCID: PMC11227306.
- Lotan Y, Krishna V, Abuzeid WM, Launer B, Chang SS, Krishna V, Shingi S, Gordetsky JB, Gerald T, Woldu S, Shkolyar E, Hayne D, Redfern A, Spalding L, Stewart C, Eyzaguirre E, Imtiaz S, Narayan VM, Packiam VT, O'Donnell MA, Li R, Baekelandt L, Joniau S, Zuiverloon T, Fernandez MI, Schultz M, Hensley PJ, Allison D, Taylor JA, Hamza A, Kamat A, Nimgaonkar V, Sonawane S, Miller DL, Watson D, Vrabac D, Joshi A, Shah JB, Williams SB. Predicting Response to Intravesical Bacillus Calmette-Guérin in High-Risk Nonmuscle-Invasive Bladder Cancer Using an Artificial Intelligence-Powered Pathology Assay: Development and Validation in an International 12-Center Cohort. J Urol. 2025 Feb;213(2):192-204. doi: 10.1097/JU.0000000000004278. Epub 2024 Oct 9. PMID: 39383345.
- Powles T, Assaf ZJ, Davarpanah N, et al. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2021 Jan;22(1):107-117. doi:10.1016/S1470-2045(20)30541-6
- Ben-David R, Tillu N, Cumarasamy S, Alerasool P, Rich JM, Kaufmann B, Elkun Y, Attalla K, Mehrazin R, Wiklund P, Sfakianos JP. Longitudinal Tumor-informed Circulating Tumor DNA Status Predicts Disease Upstaging and Poor Prognosis for Patients Undergoing Radical Cystectomy. Eur Urol Oncol. 2024 Oct;7(5):1105-1112. doi: 10.1016/j.euo.2024.03.002. Epub 2024 Mar 22. PMID: 38521660.