(UroToday.com) The American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, Nevada, was host to the Society of Urologic Oncology (SUO) Session. Dr. Bernard Bochner delivered the Whitmore Lecture: The Evolving Role of Surgery for Bladder Cancer - The Surgeon Can Make a Difference.
Dr. Bochner began his presentation by highlighting that we owe a great debt of gratitude to Dr. Donald Skinner, a founding member of the SUO, for establishing the surgical principles for radical cystectomy. It is largely through his intuition, innovation, and dedication to advancing surgical standards that we are witnessing the ongoing improvements in patient outcomes today.
Bladder cancer is having its moment. We are witnessing remarkable progress in systemic therapy for the first time since the introduction of cisplatin in the 1980s. Whether through the use of checkpoint inhibitors combined with chemotherapy in the perioperative setting, or antibody-drug conjugates like enfortumab vedotin paired with immune checkpoint inhibitors in the advanced setting, we are seeing dramatic improvements in patient survival as shown in the survival curves below.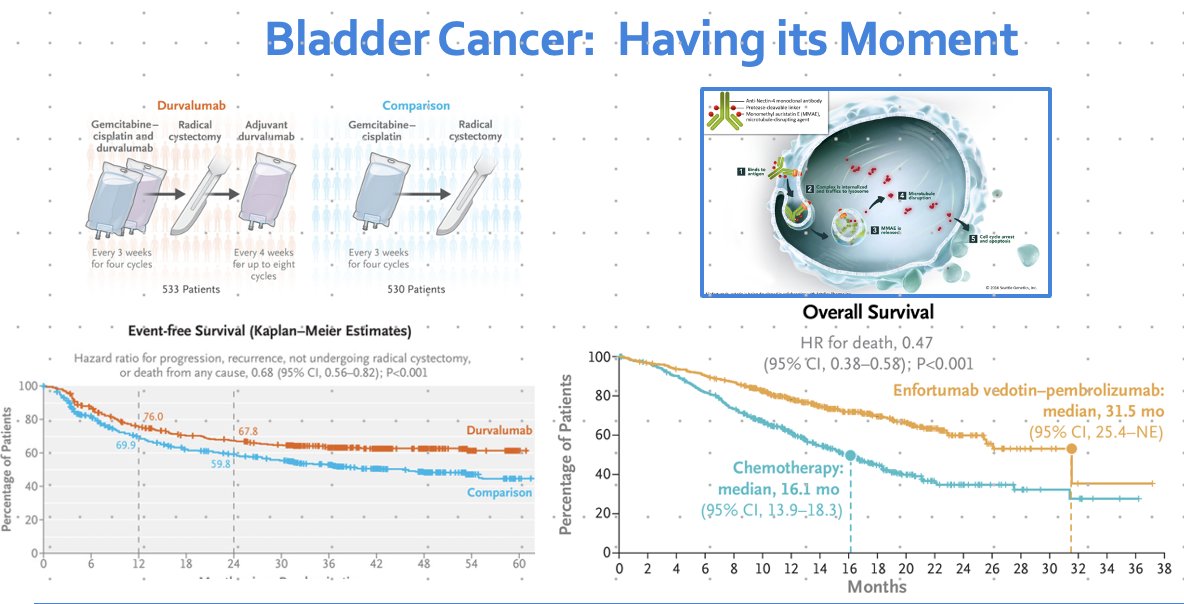
What is the state of surgery for the management of bladder cancer in 2025?
Dr. Bochner highlighted that the probability of remaining recurrence-free after radical cystectomy varies significantly among different pathological stage groups, with patients who have lymph node involvement showing the poorest recurrence-free survival compared to those with organ-confined disease, as illustrated below. But the most important thing is that some of these patients can be rendered disease-free by surgery alone.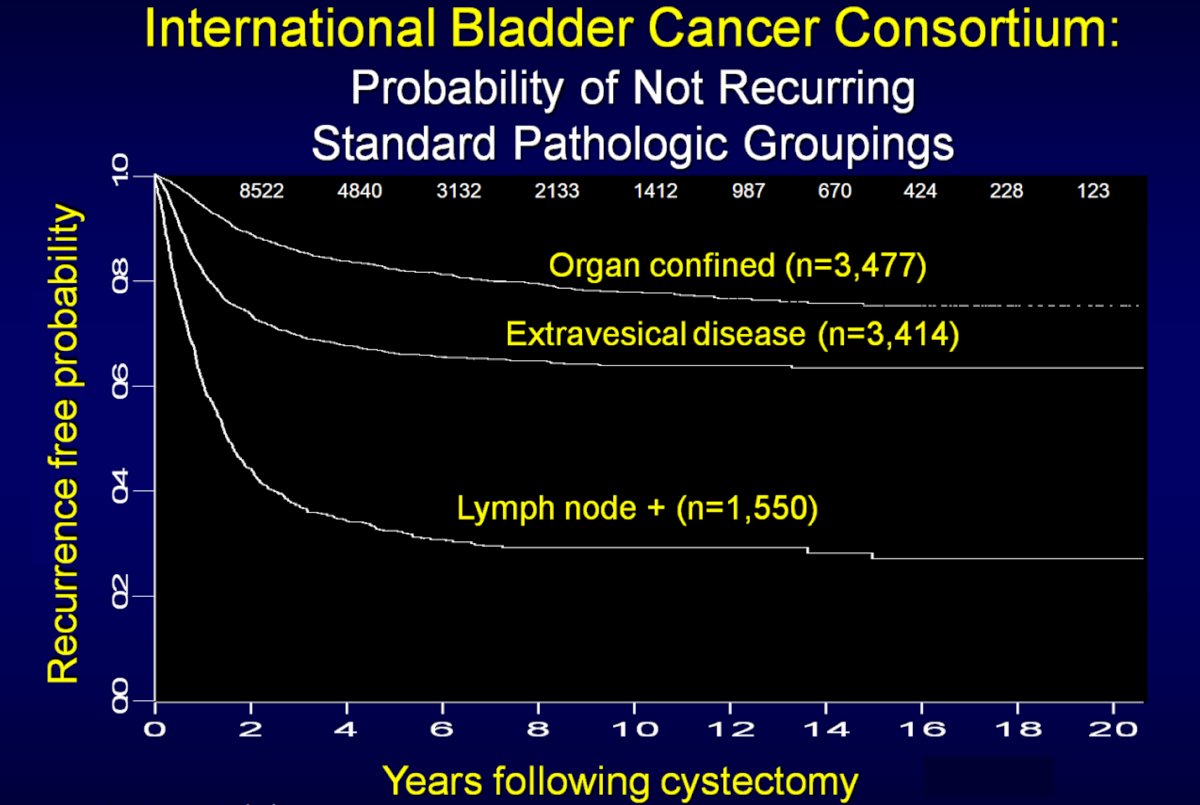
A study by Dr. Almassi and colleagues evaluated trends in management and outcomes among patients with urothelial carcinoma undergoing radical cystectomy at Memorial Sloan Kettering between 1995 and 2015. The study included 2,740 patients, and patient characteristics have remained consistent over the last decades. In this cohort, patients were male, with a median age of 68 years; notably, 41% had variant histology. Positive soft tissue surgical margins were reported in 5.1% of patients, positive urothelial margins in 11%, and lymph node involvement in 20%. Over the two decades analyzed, the incidence of clinical non–muscle-invasive disease remained relatively stable between 30–35%, and no significant stage shift was observed, as illustrated below.1

Notably, the use of neoadjuvant chemotherapy (NAC) in muscle-invasive bladder cancer (MIBC) increased significantly over time, with NAC administered to 34% of all MIBC patients between 1995–2015, rising to 57% among patients treated from 2010–2015. It is well-established that pre-surgical chemotherapy improves cure rates, increasing absolute overall survival by 5–7% compared to surgery alone, and decreases the risk of bladder cancer–specific death by approximately one-third.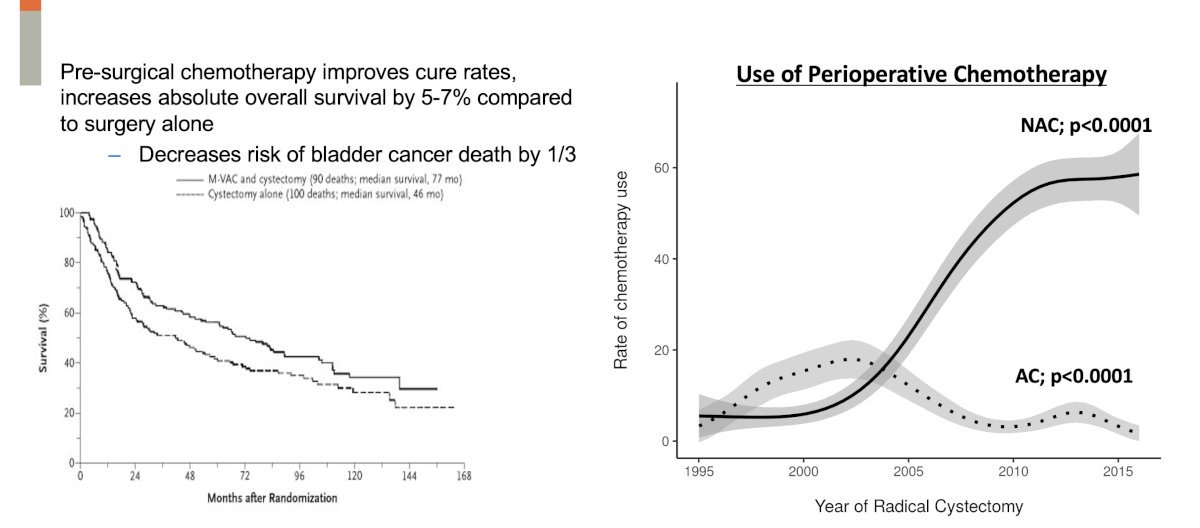
In this cohort, the overall pT0N0 rate among patients receiving neoadjuvant chemotherapy was 22%. Additionally, the incidence of positive soft tissue surgical margins significantly decreased over time, from 10% in 1995 to 2% in 2015, as illustrated below.
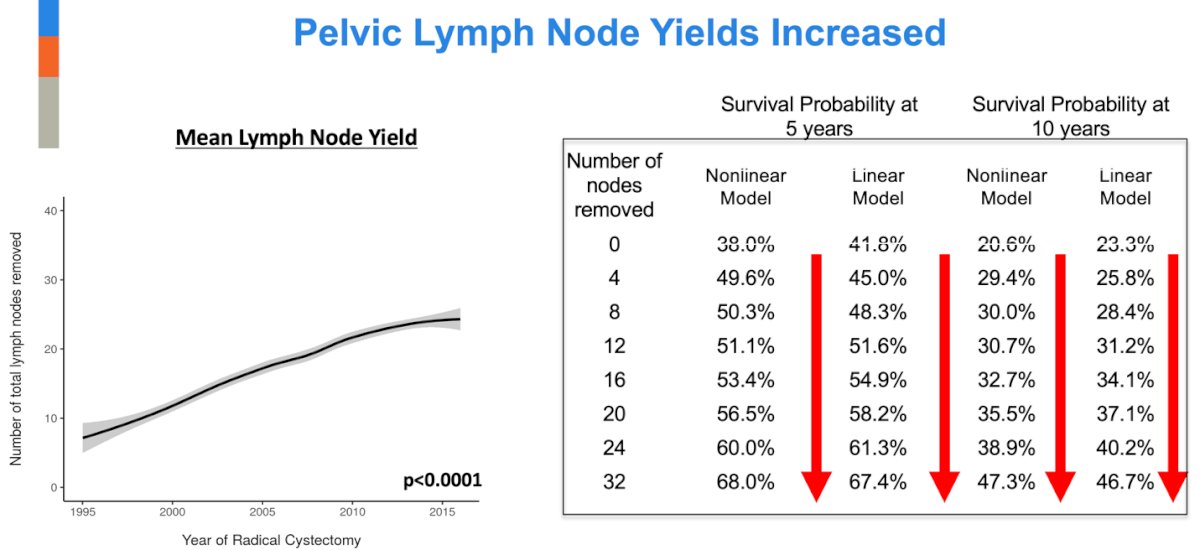
Similarly, the mean lymph node yield increased significantly from 7 nodes in 1995 to 24 nodes in 2015. Importantly, the number of lymph nodes removed was directly predictive of survival at both 5 and 10 years, in both nonlinear and linear models.1
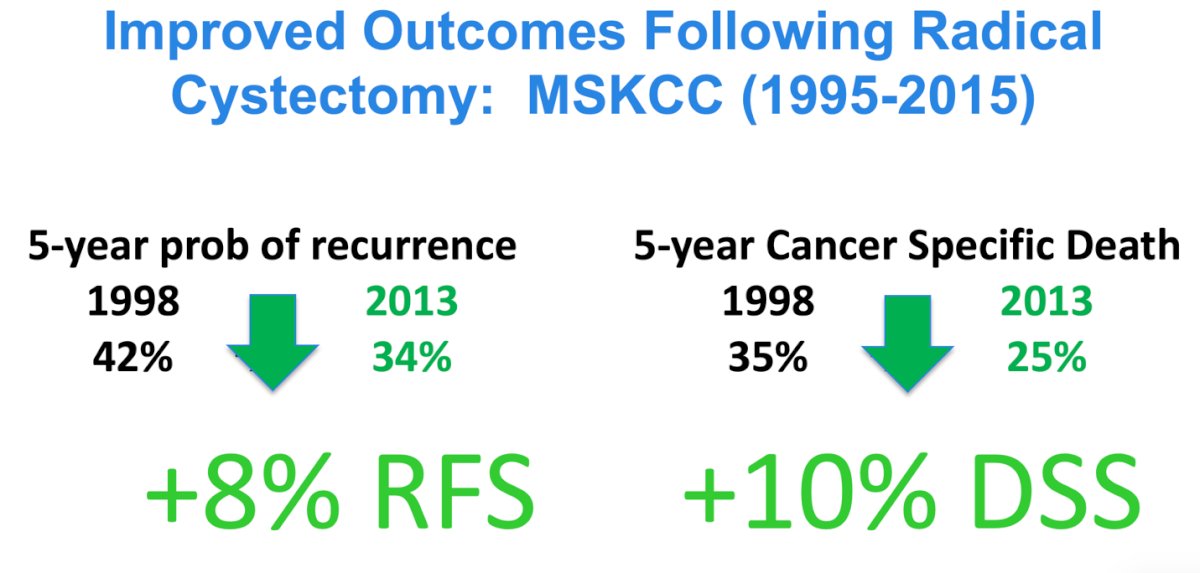
Notably, Dr. Bochner and colleagues observed improved outcomes following radical cystectomy at MSKCC between 1995 and 2015. The 5-year probability of recurrence decreased from 42% in 1998 to 34% in 2013, reflecting an 8% absolute reduction. Similarly, the 5-year probability of cancer-specific mortality declined from 35% to 25% over the same period, corresponding to a 10% improvement in cancer-specific survival. In terms of overall survival (OS), the 5-year OS improved from 50% in 1998 to 62% in 2013 with an absolute improvement of 12%.
There is significant early morbidity following radical cystectomy, as shown in the MSKCC series from 1995 to 2005. In this cohort, 1,142 consecutive patients (median age 68 years) were prospectively entered into a complication database, with retrospective review for accuracy. All complications within 90 days of surgery were analyzed and graded according to the MSKCC complication grading system. Overall, 64% (three quarters) of patients experienced a complication within 90 days (67% during hospitalization and 58% following discharge). Gastrointestinal complications were the most common, followed by infectious and wound-related events. The 30-day mortality rate was 1.5%. Notably, while surgical morbidity after radical cystectomy is considerable, 80% of all complications were graded as mild to moderate (grade 1–2).2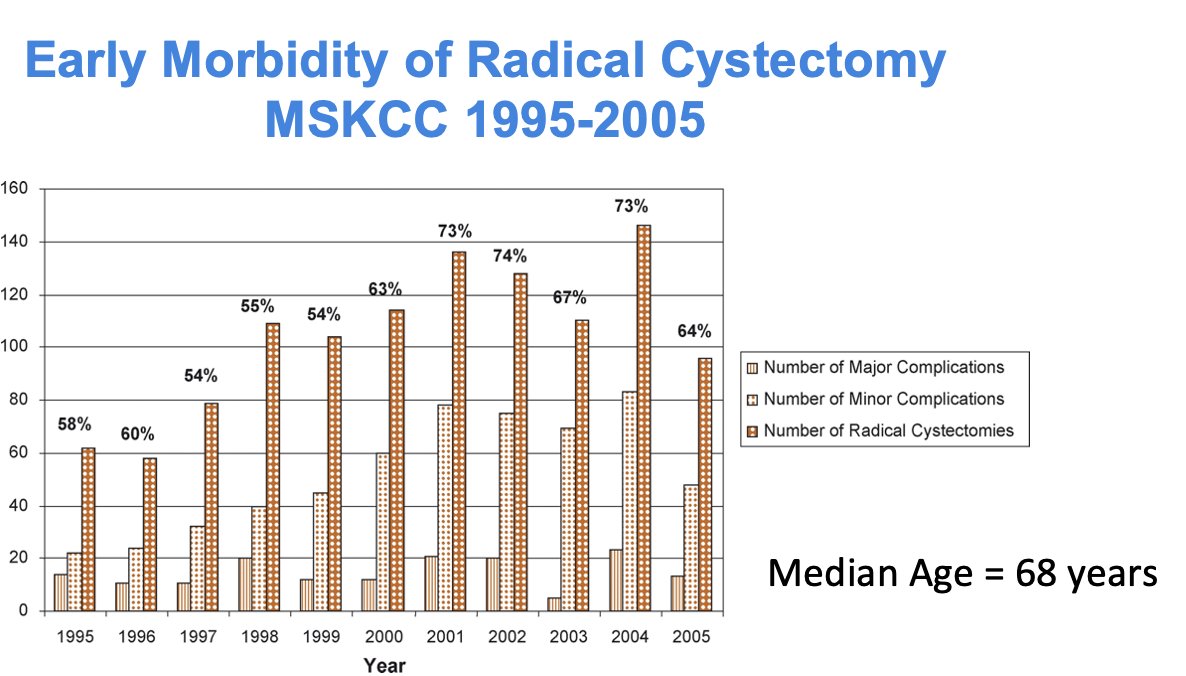
Dr. Bochner presented a comparison of Grade 3/4 complications in patients undergoing either robot-assisted radical cystectomy (RARC) or open radical cystectomy (ORC), as well as in patients undergoing standard pelvic lymph node dissection (PLND) versus extended PLND (ePLND). No significant differences were observed in complication rates across these groups, based on data from the landmark trials shown below. However, in the SWOG S1011, there was an absolute difference of 10% in Grade 3/4 complications between ePLND and sPLND.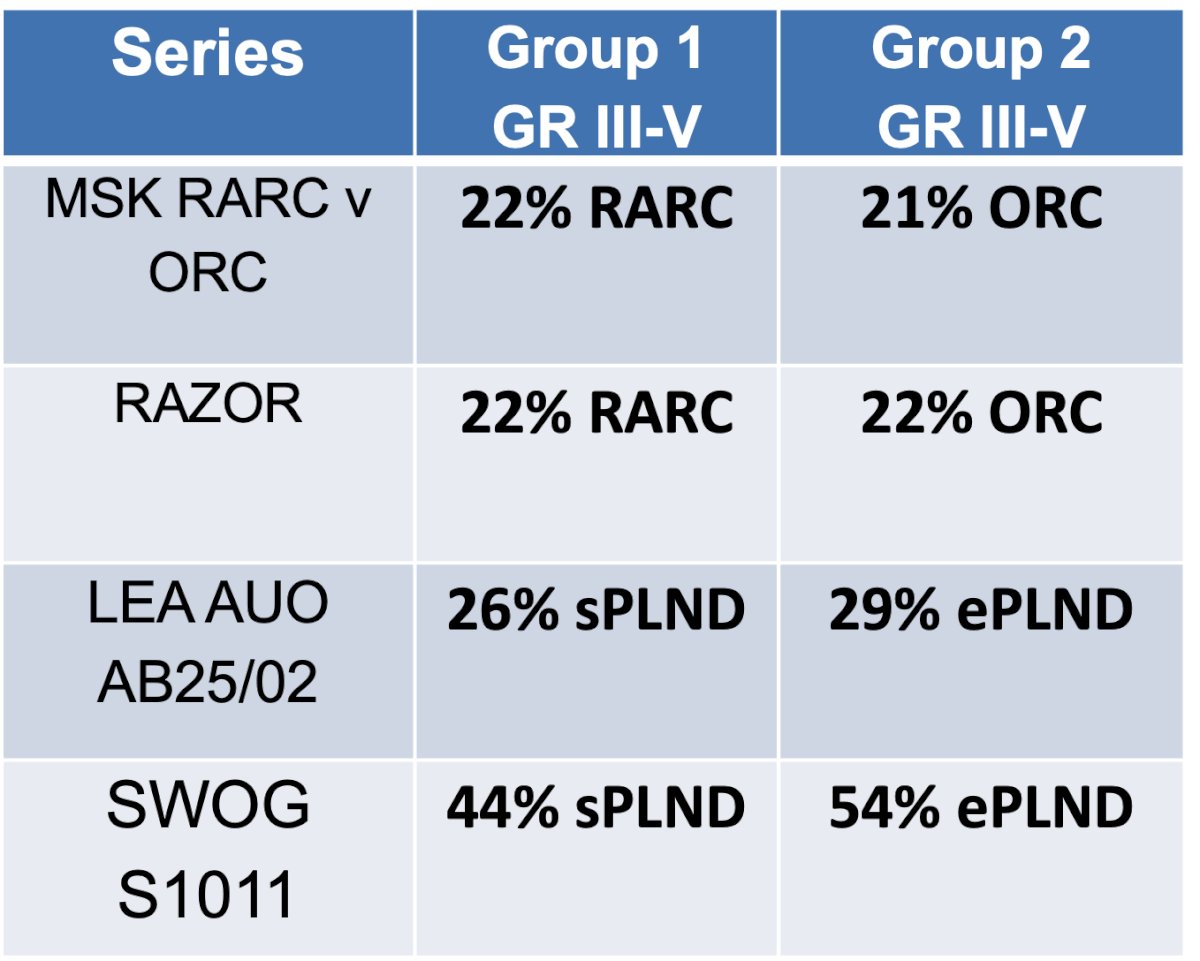
Patient reported quality of life outcomes following radical cystectomy and urinary diversion
Perceptions of quality of life (QOL) changes after radical cystectomy demonstrate that declines are often sustained, may worsen over time, and can result in a dramatic long-term decrease in QOL. Elderly patients are at the greatest risk for experiencing large and persistent declines. These concerns about QOL have led both physicians and patients to increasingly seek non-cystectomy treatment options whenever appropriate.
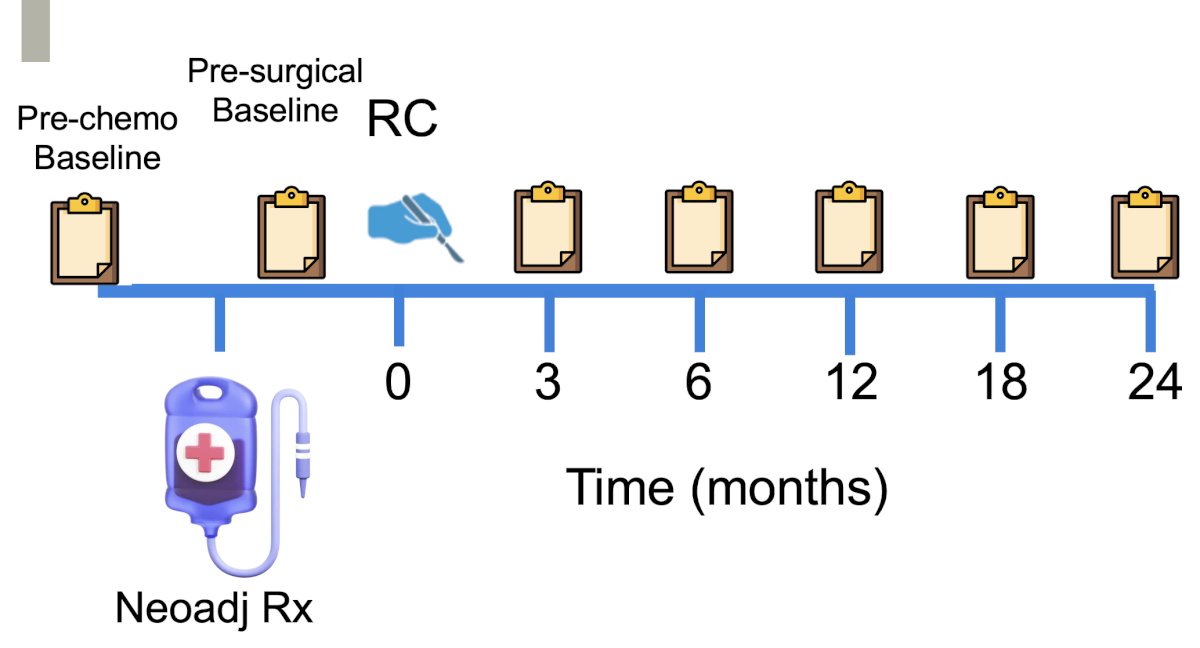
A single-center prospective study (NCT00745355) conducted at MSKCC between 2008 and 2014 enrolled 550 patients, of whom 462 M0 patients were eligible for analysis. Patients scheduled for radical cystectomy, with or without preoperative chemotherapy, were included. The choice of urinary diversion was made per standard of care. Patient-reported QOL was assessed at multiple time points, beginning with pre-chemotherapy baseline and pre-surgical baseline, followed by serial measurements at 3, 6, 12, 18, and 24 months after surgery.3
Patient-reported quality of life (PRO-QOL) was assessed using several questionnaires, evaluating multiple domains related to quality of life through serial assessments.

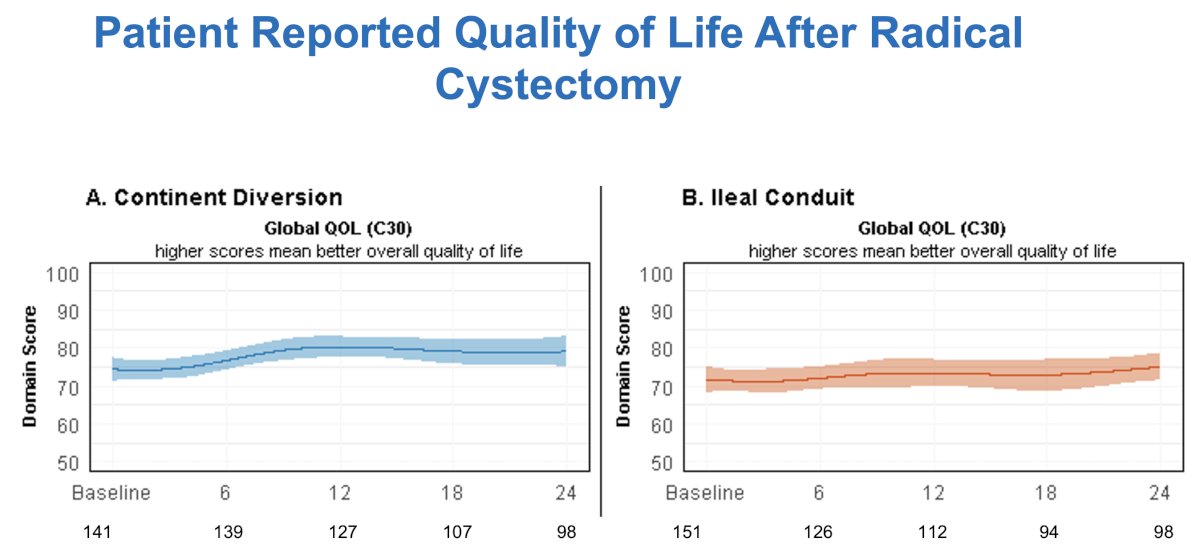
Notably, no dramatic decreases in global quality of life were observed, even in the early postoperative period, with recovery to baseline by 12 months and maintenance through 2 years, without significant differences between continent diversion and ileal conduit.
At both the 3- and 12-month time points, the curve for patients aged 80 and older was similar to that of younger patients, with most recovering well to their baseline by 12 months. Notably, among patients aged 80 and older, the baseline mean score was 71, 69 at 3 months, and 73 one year after radical cystectomy.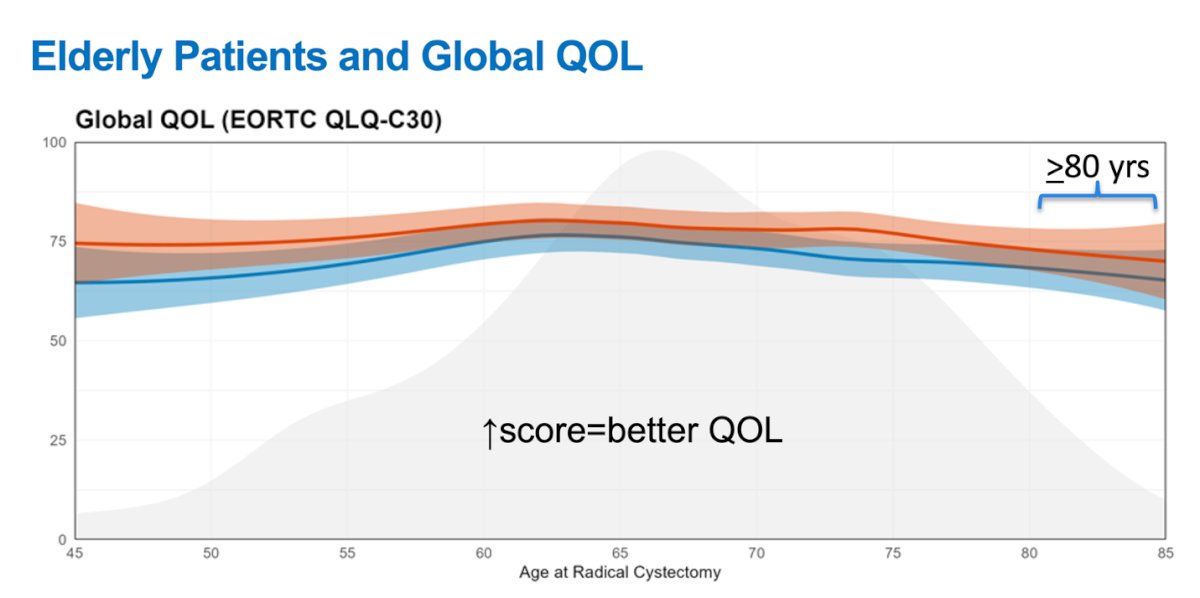
Regarding physical functioning after radical cystectomy, patients receiving ileal conduits experienced a more marked decline compared to those with continent diversions, and this difference was maintained up to 2 years.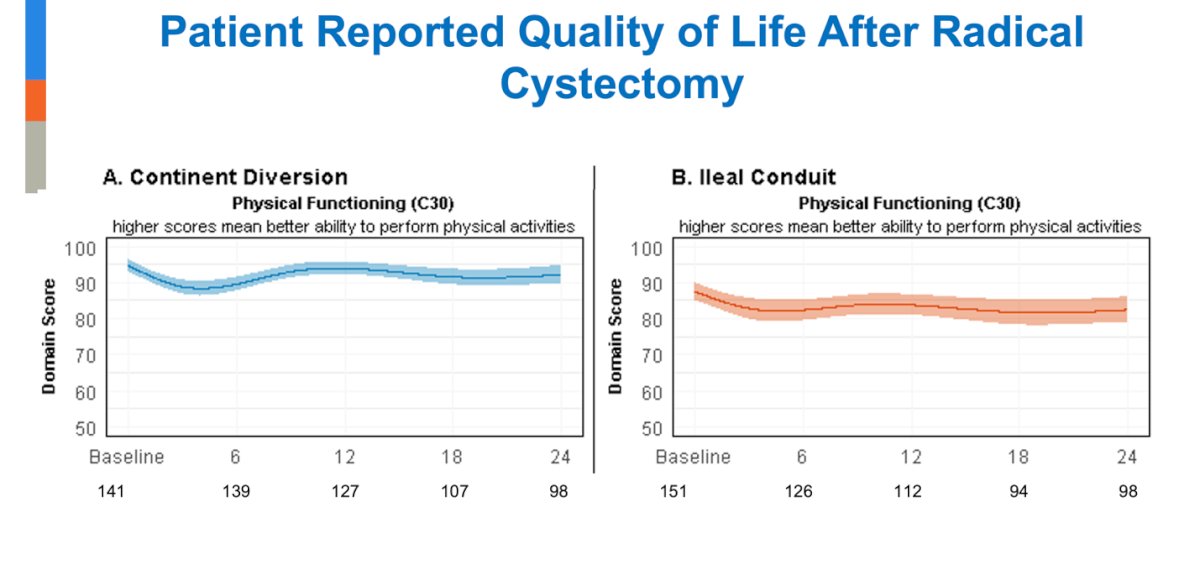
Dr. Bochner highlighted that, in a few domains, some notable age-associated differences were observed in the older group. Physical functioning improved from the 3-month to the 12-month time point for all patients. However, at 12 months, the oldest patients had worse mean physical functioning, with a 10-point difference between an 80-year-old (83) and a 60-year-old (93), despite similar preoperative baselines of 92 as shown below.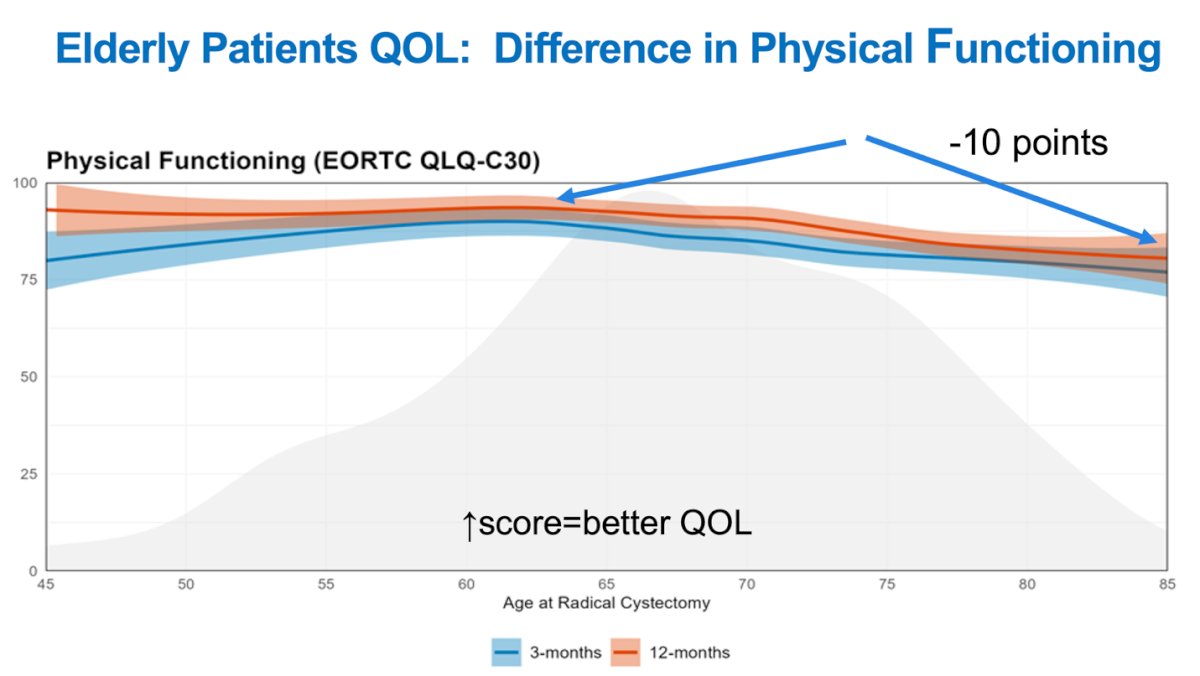
Erectile function recovery after radical cystectomy was generally low and largely depended on whether a nerve-sparing approach was performed. However, among patients without erectile dysfunction at baseline who underwent neobladder diversion and the neurovascular bundles were spared, two-thirds remained free of erectile dysfunction at 24 months post-cystectomy.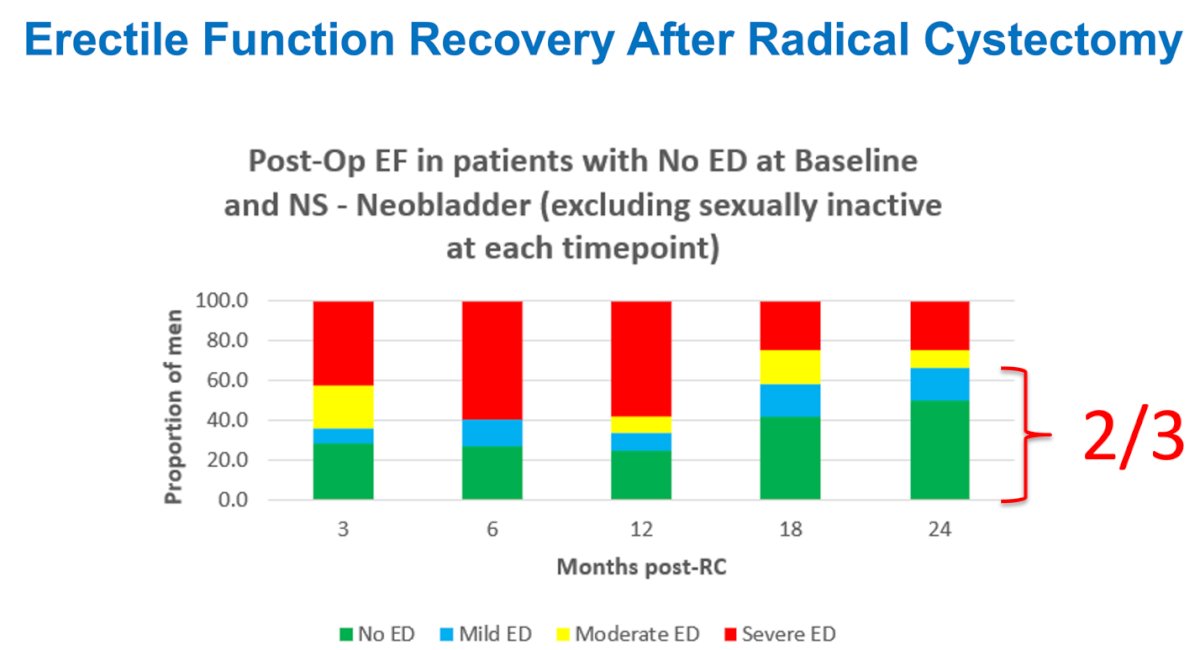
Another domain that does not recover very well after RC is body image. Younger patients, particularly those under 60 years, reported greater body image concerns at both 3 and 12 months.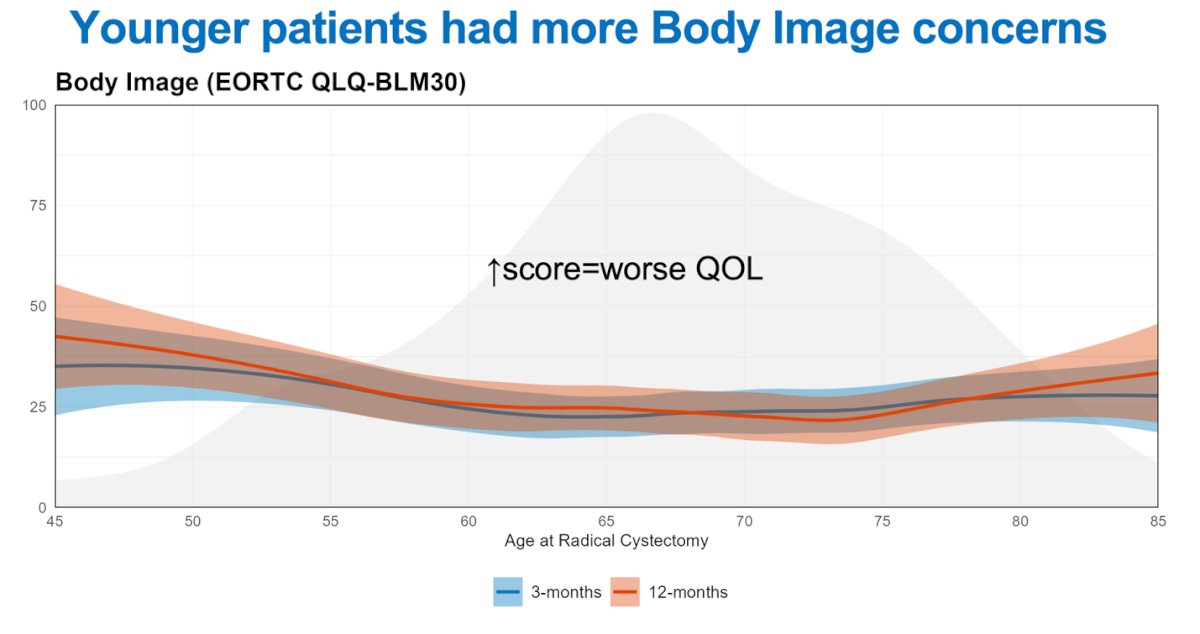
The urostomy domain, which encompasses care of the urostomy, was evaluated only in patients aged 60 and older due to the small number of younger patients who received an ileal conduit. Scores were similar across patients aged 60 to 85, indicating that older patients did not struggle with urostomy care, as illustrated below.
Moreover, Dr. Bochner discussed that despite advancements in bladder cancer surgery, the rate of continent urinary diversion in the United States remained stable from 2006 to 2014, with 11,837 patients receiving continent diversions during that period. In contrast, 38,516 patients underwent continent diversion in Germany, where it has historically played a major role in bladder cancer surgery, although its use has declined over the past decade.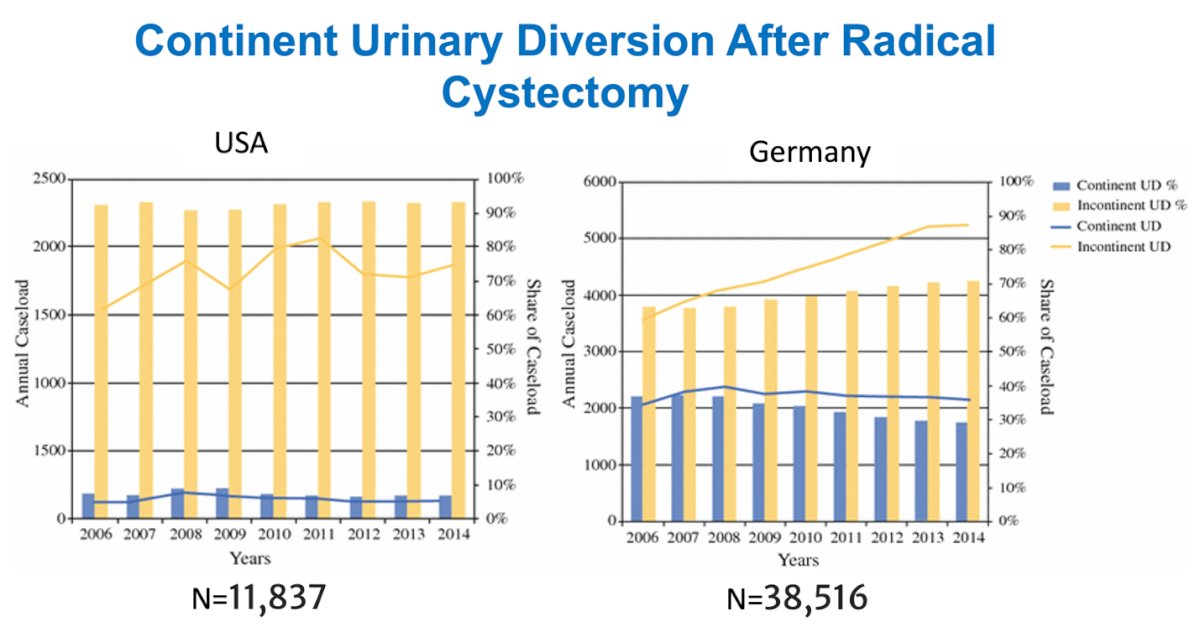
Urinary quality of life appeared to improve over time, whether in the urostomy symptoms domain among ileal conduit patients or across various measures of urinary quality of life in orthotopic neobladder patients as shown in the graphics below.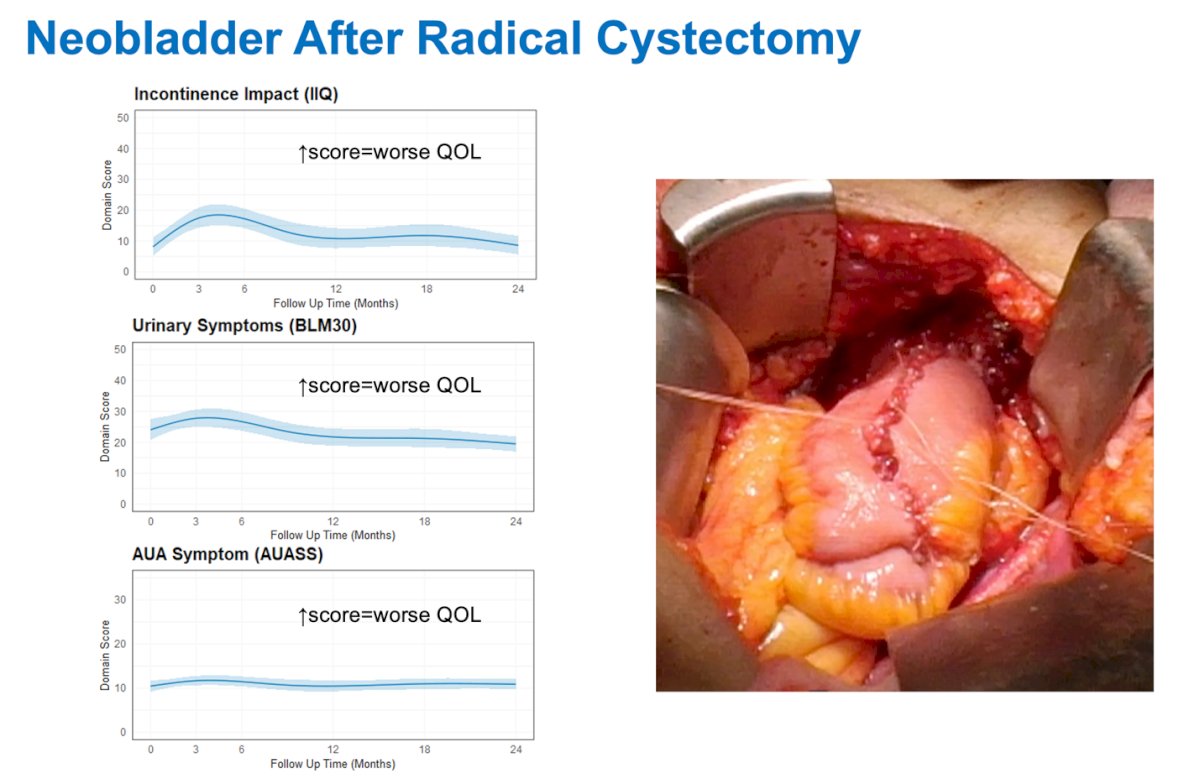
Comparing the urinary symptoms domain between male and female patients who underwent neobladder reconstruction after radical cystectomy, urinary quality of life appeared similar between sexes and improved over time.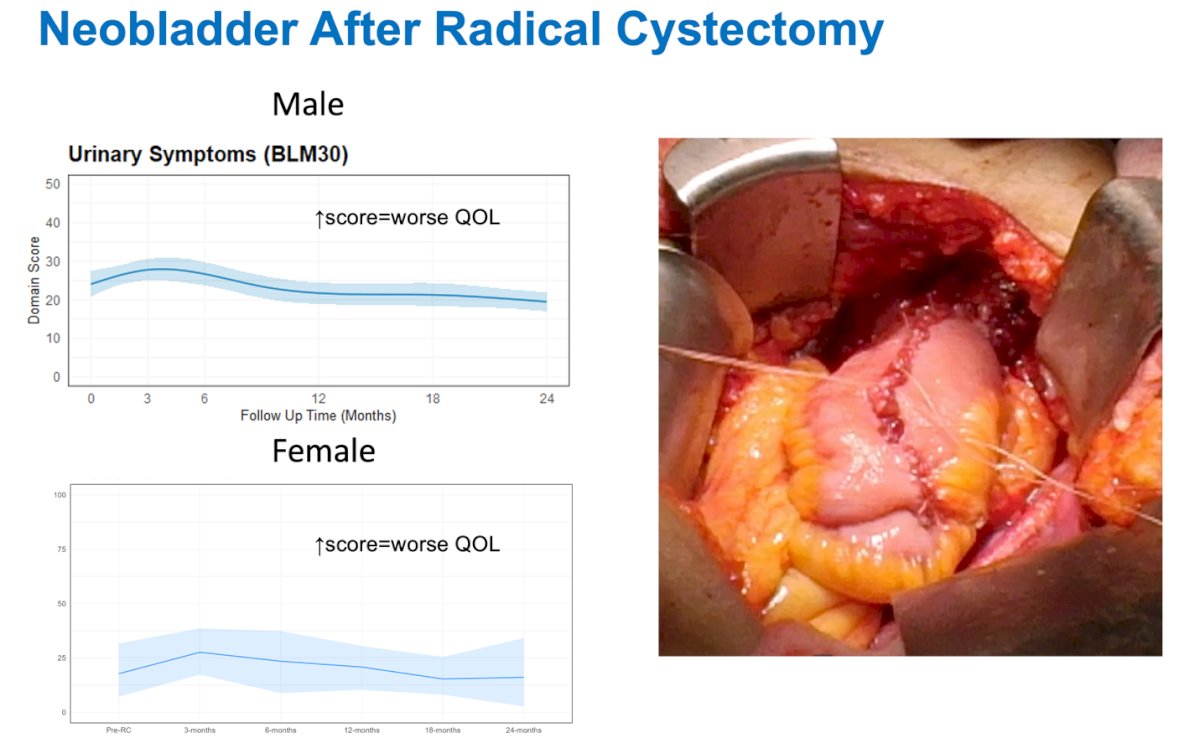
What is the future role of radical surgery for invasive, high risk bladder cancer?
Dr. Bochner noted that bladder preservation is possible with neoadjuvant chemotherapy alone. He presented data from three patient cohorts with mid- and long-term follow-up, showing overall survival rates ranging from 68% to 75% and bladder-intact survival in more than half of the patients. We should remember that the bar is set very high for bladder preservation strategies. He also highlighted that in the SWOG 8710 trial, 85% of patients with pT0 disease who underwent cystectomy were alive after 2 years.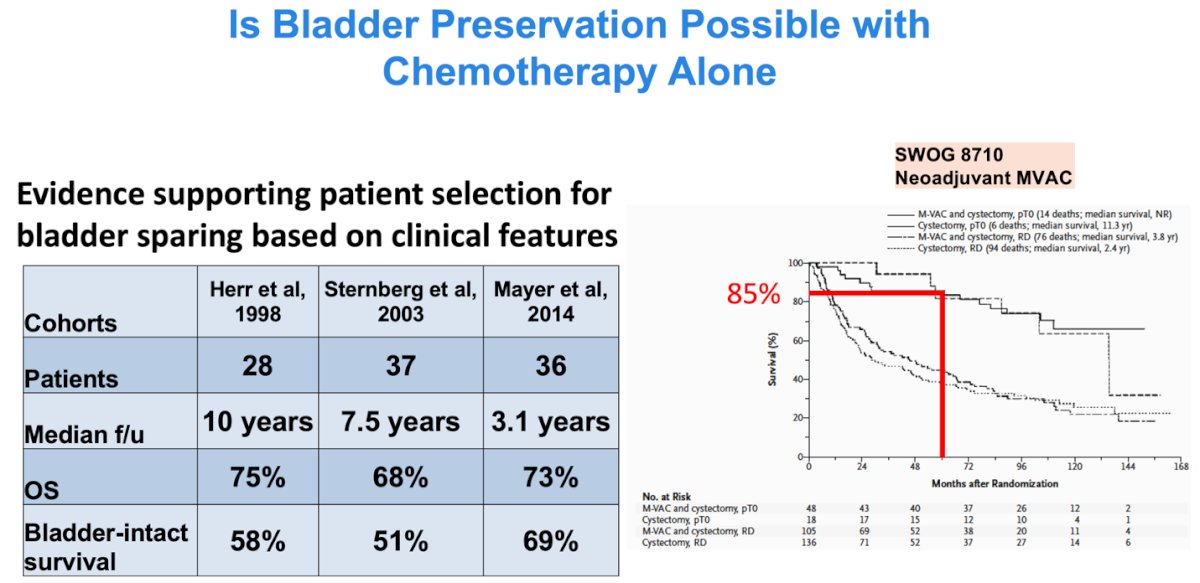
The question raised was whether clinical and molecular features can be used to carefully select a subset of MIBC patients who could be managed with systemic therapy alone, without definitive local therapy. It was highlighted that certain molecular features, such as DNA damage repair (DDR) alterations, have been associated with long-term disease control both within and outside the bladder.
The Alliance A031701 (NCT03609216) bladder preservation trial is aiming to answer this question. The protocol incorporates genetic sequencing of TURBT specimens, and if DDR alterations are present and a cT0 or CIS response is achieved after chemotherapy, patients are offered bladder-sparing management. The primary endpoint is 3-year recurrence-free survival (RFS), defined as any recurrence leading to radical cystectomy or any distant (M1) recurrence. The study design is shown below.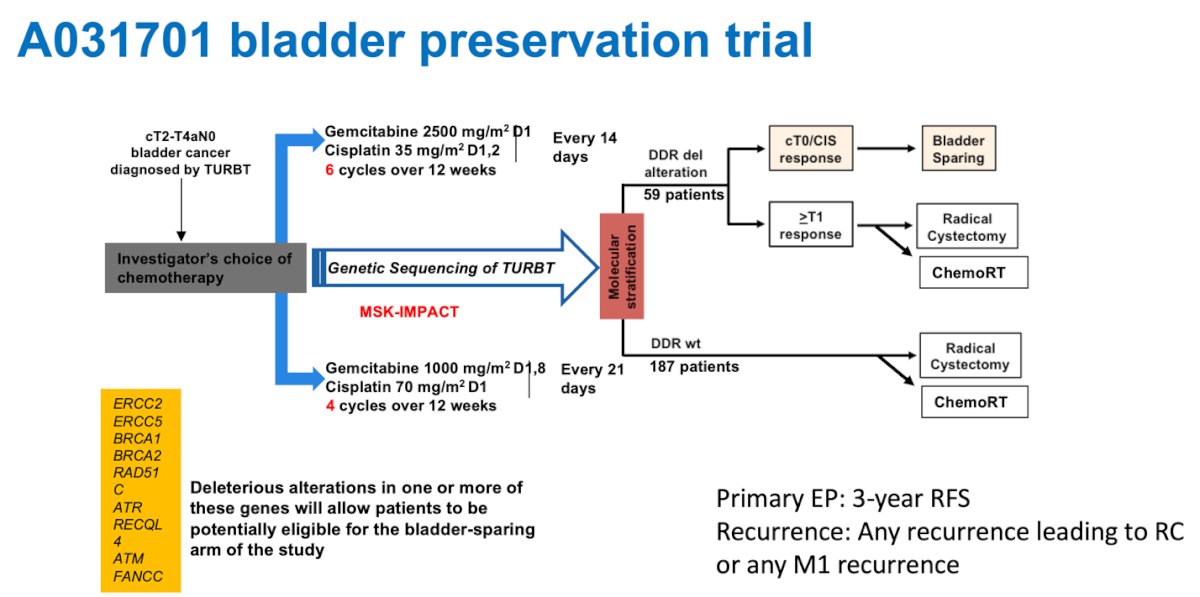
Moreover, Dr. Bochner briefly discussed the perioperative NIAGARA trial, which evaluated durvalumab combined with chemotherapy in the perioperative setting. The pathological complete response (pCR) rate was 37%, and he noted that as more effective upfront systemic therapies are developed, there may be an increasing number of candidates for bladder preservation.4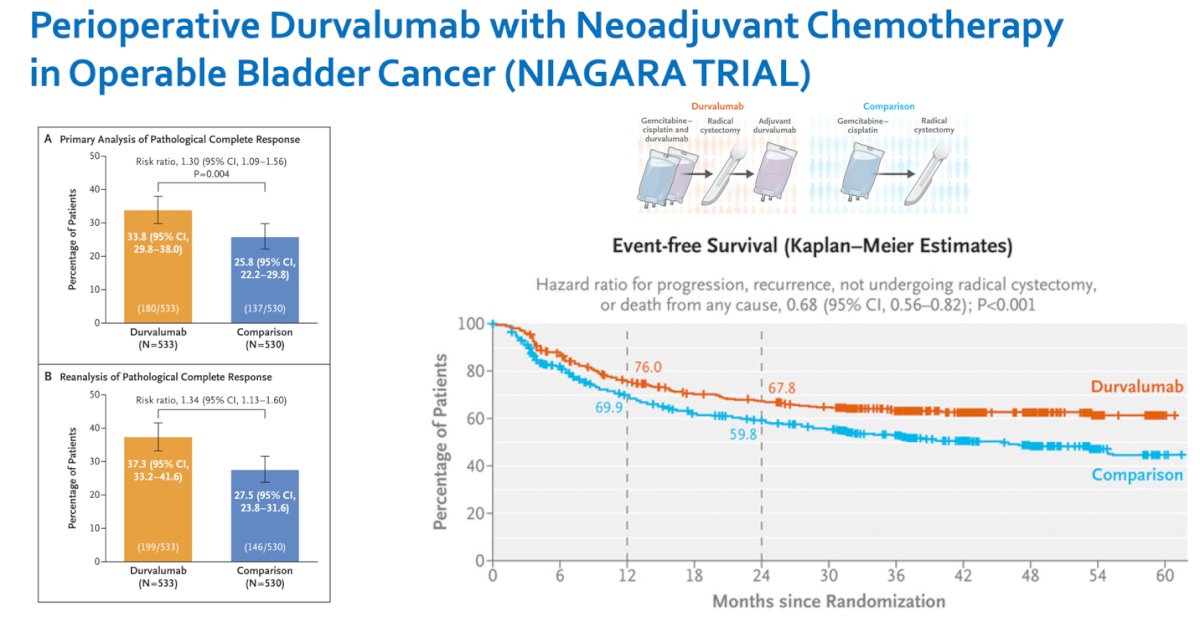
In the advance setting, antibody-drug conjugates (ADCs) such as enfortumab vedotin a fully human antibody targeting Nectin-4 conjugated to monomethyl auristatin E (MMAE), have shown dramatic improvements in survival for patients with metastatic disease when combined with checkpoint inhibitors. Median survival with enfortumab vedotin is now approaching 3 years. As patients live longer, new tumors or progressive local disease are emerging in the setting of controlled distant disease. Surgery will likely begin to play an increasing role in the overall management of these fortunate patients.

Dr. Bochner concluded the Whitmore Lecture with several key messages. He emphasized that surgery can provide unmatched tumor control while maintaining patient quality of life. He outlined the keys to successful patient outcomes: proper preoperative evaluation and patient selection, thorough preparation for surgery, delivery of optimal surgical care, and strong postoperative support.
He closed by underscoring that surgical quality matters, stating, "Every job is a self-portrait of the person who did it. And encourage us to “Autograph your work with excellence."
Presented by: Bernard Bochner, MD, FACS, Sir Murray Brennan Endowed Chair in Surgery at the Memorial Sloan Kettering Cancer Center (MSKCC) and Clinical lead of the urothelial disease management team at MSKCC. New York, NY.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025 in Las Vegas, NV.
References- Almassi N, Cha EK, Vertosick EA, Huang C, Wong N, Dason S, McPherson V, Dean L, Benfante N, Sjoberg DD, Rosenberg JE, Bajorin DF, Herr HW, Dalbagni G, Bochner BH. Trends in Management and Outcomes among Patients with Urothelial Carcinoma Undergoing Radical Cystectomy from 1995 to 2015: The Memorial Sloan Kettering Experience. J Urol. 2020 Oct;204(4):677-684. doi: 10.1097/JU.0000000000001071. Epub 2020 Apr 15. PMID: 32294398; PMCID: PMC7483392.
- Shabsigh A, Korets R, Vora KC, Brooks CM, Cronin AM, Savage C, Raj GV, Bochner BH, Dalbagni G, Herr HW, Donat SM. Defining early morbidity of radical cystectomy for patients with bladder cancer using a standardized reporting methodology. European Urology. 2009 Jan;55(1):164-74. doi:10.1016/j.eururo.2008.07.031.
- Clements T, Porteous AJ, Noon AP, Catto JWF. Quality of Life After Radical Cystectomy and Urinary Diversion: A Systematic Review. European Urology. 2021 Mar;79(3):508-520. doi:10.1016/j.eururo.2020.10.019.
- Powles T, Catto JWF, Galsky MD, et al. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. New England Journal of Medicine. 2024;391(19):1773–1786