(UroToday.com) At the 2025 AUA Annual Meeting in Las Vegas, Dr. Jethro C.C. Kwong, from the University of Toronto, presented a retrospective international cohort study addressing a pressing controversy in the risk stratification of non-muscle invasive bladder cancer (NMIBC). Specifically, the study questioned whether primary, solitary, and small (< 3 cm) high-grade (TaHG) tumors without carcinoma-in-situ (CIS) should be classified as intermediate-risk (IR) or high-risk (HR) disease in light of differences in urologic guidelines.
Current guidelines vary on this categorization. While the American Urological Association (AUA) and some others allow for primary, solitary, small TaHG tumors to be considered IR, other groups, such as the International Bladder Cancer Group, argue that all TaHG tumors, regardless of size or number, should be treated as HR. The European Association of Urology (EAU) guidelines further allow TaHG tumors with up to one risk factor (age >70, multiple tumors, or tumor size ≥3 cm) to remain classified as IR. Given these conflicting stances, Dr. Kwong and colleagues aimed to clarify this by analyzing the progression risk associated with these tumors in a large, international, multi-institutional cohort.
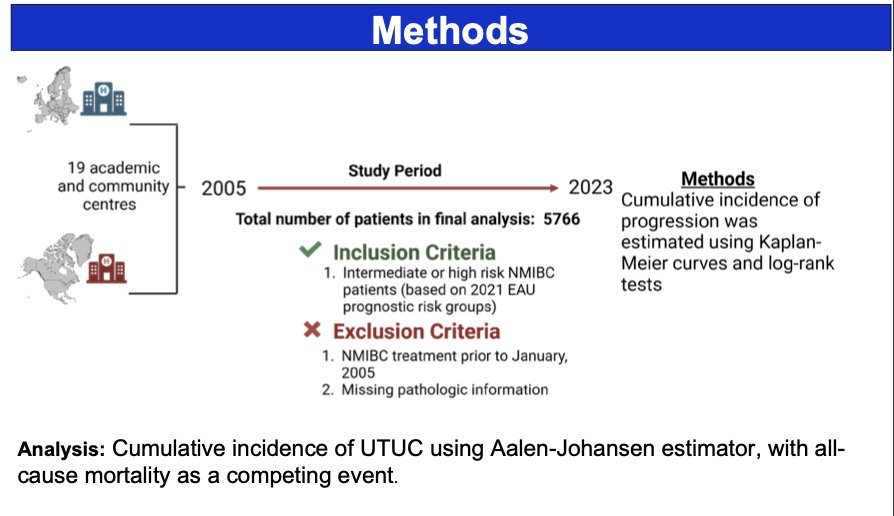
The team retrospectively collected clinicopathologic data from 19 institutions across North America and Europe, enrolling patients treated between 2005 and 2023. Patients were categorized based on the 2021 EAU prognostic risk groups. The primary outcome was time to progression, defined as the development of muscle-invasive or metastatic disease. Kaplan-Meier analyses and log-rank tests were employed to compare progression rates between groups.
Among 5,774 patients included:
- 1,070 (19%) had IR low-grade (LG) tumors
- 620 (11%) had primary, solitary, <3 cm TaHG without CIS
- 572 (10%) had other IR TaHG (with one risk factor)
- 834 (14%) had HR TaHG (with ≥2 risk factors)
- 2,678 (46%) had HR T1HG disease
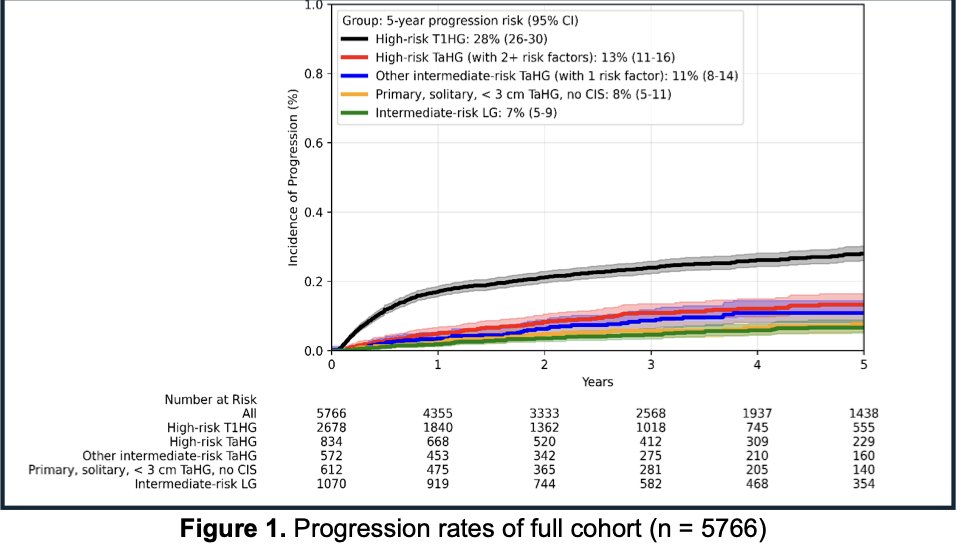
With a median follow-up of 3.0 years (IQR 1.4-5.4), the estimated 5-year progression risks were:
- 7% for IR LG tumors
- 8% for primary, solitary, <3 cm TaHG without CIS
- 11% for other IR TaHG
- 13% for HR TaHG
- 28% for HR T1HG tumors
Importantly, no significant difference was observed in time to progression between the IR LG group and the primary, solitary, < 3 cm TaHG without CIS group (p = 0.16), suggesting that these TaHG tumors behave similarly to traditional IR tumors. Conversely, other IR TaHG tumors (with one risk factor) displayed a statistically significantly worse prognosis compared to IR LG (p = 0.002).
A notable limitation highlighted by the presenter was the lack of data regarding Bacillus Calmette-Guérin (BCG) maintenance therapy for all patients, which may have influenced progression outcomes.
The study concluded that primary, solitary, small (<3 cm) TaHG tumors without CIS align more closely with intermediate-risk disease rather than high-risk disease. However, other TaHG tumors, including those with even one additional risk factor, should be considered high-risk. This clarification holds significant clinical implications for the appropriate risk stratification, counseling, and management of patients with NMIBC.
Following the presentation, moderator Dr. Karim Chami asked, “Were these patients treated like high-risk? Were they receiving BCG, were they receiving gemcitabine?” Dr. Kwong responded, “in terms of intravesical chemotherapy usage, it is not very much, at least for patients included in this cohort” and went on to highlight, “for those that received BCG 7%, if you didn’t receive BCG 8%” in regard to 5-year progression risk and the insignificance between these groups.
Presented by: Jethro C.C. Kwong, MD, University of Toronto, Toronto, Canada
Written by: Mark Sarwat Hana, Assistant Research Specialist, Department of Urology, University of California, Irvine, during the American Urological Association's 2025 Annual Meeting, between April 26 – 29, 2025, in Las Vegas, NV.