(UroToday.com) The American Urological Association (AUA) 2025 Annual Meeting, held in Las Vegas, NV, was host to a non-invasive bladder cancer podium session. Dr. Vignesh Packiam presented a study of an artificial intelligence-powered predictive biomarker for response to intravesical BCG versus gemcitabine + docetaxel in high-grade, non-muscle invasive bladder cancer (NMIBC) patients.
EA-8212 (BRIDGE) is evaluating BCG versus gemcitabine and docetaxel in BCG-naïve, high-risk NMIBC patients,1 though existing studies in treatment-naïve patients suggest that sequential intravesical gemcitabine + docetaxel shows promising results in the BCG-naive setting.2 Biomarkers predicting response to BCG versus gemcitabine and docetaxel could have a significant impact on disease management. Recently, Dr. Packiam and colleagues presented a computational histology artificial intelligence (CHAI) assay that predicts response to BCG using digital images of H&E pathology slides from pre-treatment TURBT specimens:

Presence of the biomarker conferred an increased risk of recurrence, progression, and BCG unresponsive disease.3Dr. Packiam and colleagues aimed to assess if this biomarker was predictive of treatment response to BCG versus gemcitabine + docetaxel.
Pre-treatment TURBT-derived digital whole slide images and clinical data were obtained for patients with AUA high-risk, BCG-naïve NMIBC diagnosed between 2011 and 2021 and who were treated with BCG or gemcitabine + docetaxel. Whole slide images were analyzed using the CHAI assay, incorporating histologic features previously shown to be predictive of the development of BCG-unresponsive disease. Those with “biomarker-present” were previously shown to have a shorter time to BCG-unresponsive disease compared to those with “biomarker-absent”.
High-grade recurrence-free survival between BCG and gemcitabine + docetaxel was compared in the pre-defined biomarker-present and absent groups. A test for a statistical interaction between the biomarker and treatment type was assessed via Cox proportional hazards regression and likelihood ratio tests.
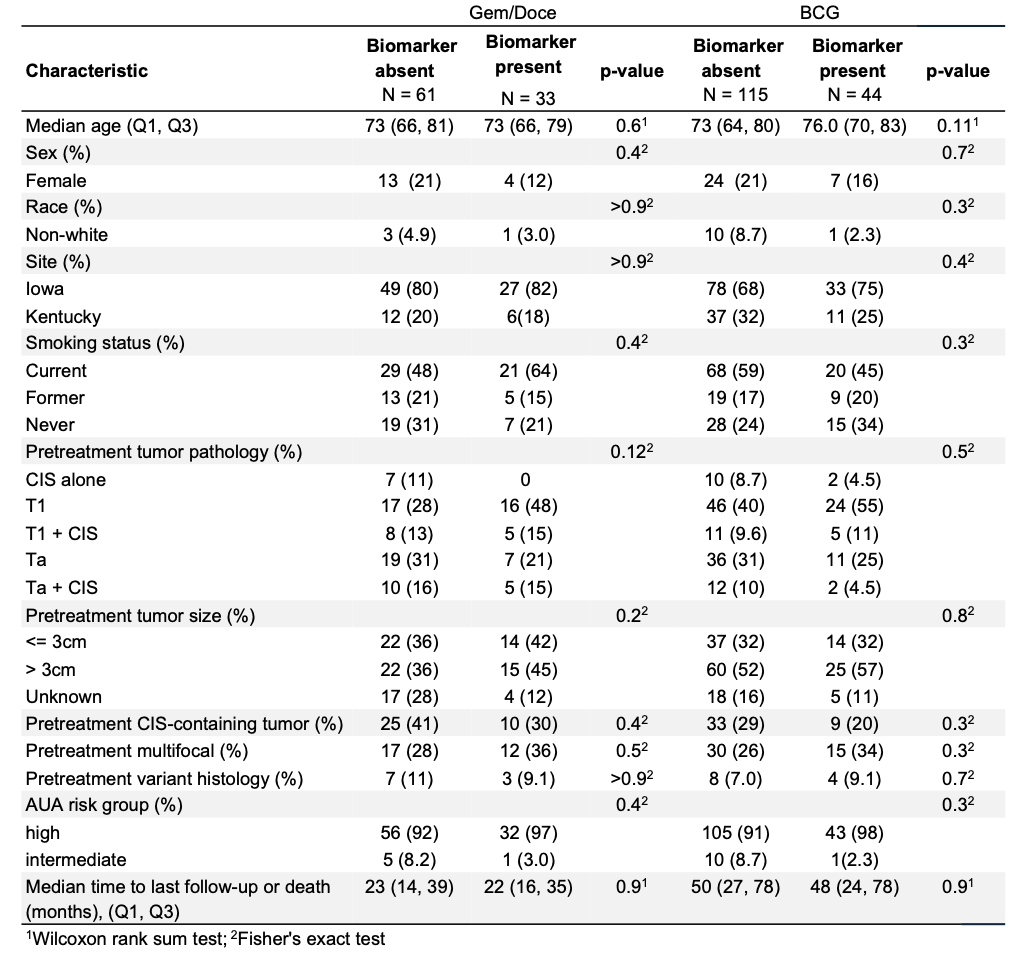
There were 253 patients with high-risk NMIBC, of whom 63% received BCG and 37% received gemcitabine + docetaxel at one of two centers. The median follow-up was 35 months. 77 (30%) were CHAI biomarker-present, and 176 (70%) were biomarker-absent. Demographic and tumor characteristics were balanced across treatment groups and CHAI biomarker status.
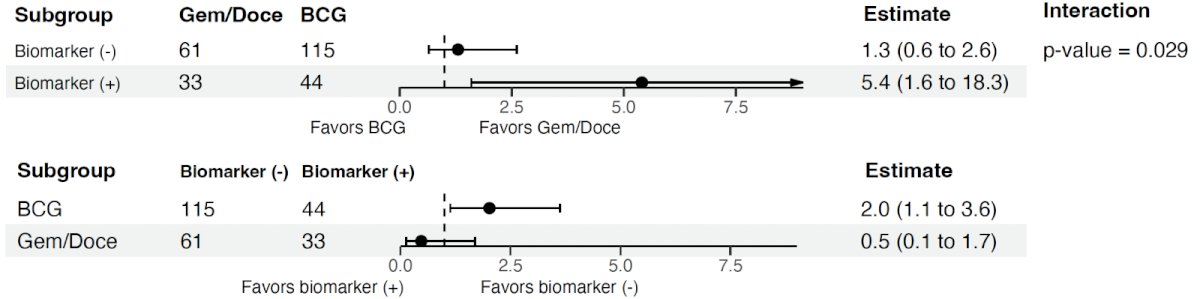
Among CHAI biomarker-present cases, gemcitabine + docetaxel-treated patients had superior high-grade recurrence-free survival, compared to BCG-treated patients (HR: 5.4; p=0.007). The 24-month high grade recurrence-free survival in gemcitabine + docetaxel-treated cases was 90% versus 56% in those receiving BCG (p=0.002).

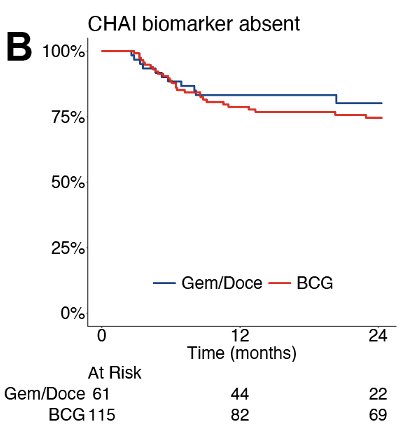
Among CHAI biomarker-absent cases, there was no significant difference in high grade recurrence-free survival between gemcitabine + docetaxel and BCG treated cases (HR: 1.2, p=0.50).
The likelihood ratio test for the biomarker treatment interaction term was statistically significant (p=0.029)m even after adjusting for AUA and EAU risk groups, indicating that the CHAI is a predictive biomarker:
Dr. Packiam concluded his presentation discussing an artificial intelligence powered model to predict response to intravesical BCG versus gemcitabine + docetaxel for high-risk NMIBC with the following take home messages:
- In the treatment-naïve setting for high grade NMIBC, BCG is the “gold standard”. However, the ongoing shortage limits patient access to BCG, and there is an unmet need for predictors of response to alternate therapies.
- Intravesical gemcitabine + docetaxel has increasing evidence supporting its viability as a BCG alternative
- This study is the first to evaluate an artificial intelligence-based histologic biomarker to predict clinical response to different intravesical therapies in high grade NMIBC
- The CHAI biomarker is statistically predictive of treatment benefit. CHAI biomarker positivity conferred superior high-grade recurrence-free survival in patients treated with gemcitabine + docetaxel, as compared to BCG
- The CHAI biomarker potentially enables a more personalized approach to the treatment of NMIBC patients, predicting clinical response to BCG versus gemcitabine + docetaxel, and thus sparing unnecessary delays and toxicity in patients unlikely to benefit from alternate therapies
Presented by: Vignesh Packiam, MD, Associate Professor, Department of Urology, Rutgers Cancer Institute of New Jersey, New Brunswick, NJ
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
Related content: Biomarkers for Gemcitabine Docetaxel in Non-Muscle Invasive Bladder Cancer - Vignesh Packiam
References:
- Kates M, Chu X, Hahn N, et al. Background and update for ECOG-ACRIN EA8212: a randomized phase 3 trial of intravesical Bacillus Calmette-Guérin (BCG) versus intravesical docetaxel and gemcitabine treatment in BCG-naïve high-grade non–muscle-invasive bladder cancer (BRIDGE). Eur Urol Focus. 2023; 9(5): 1054–61.
- McElree IM, Steinberg RL, Mott SL, et al. Comparison of sequential intravesical gemcitabine and docetaxel vs bacillus Calmette-Guérin for the treatment of patients with high-risk non–muscle-invasive bladder cancer. JAMA Netw Open. 2023; 6(2): e230849.
- Lotan Y, Bostrom PJ, Hernandez V, et al. Predicting response to intravesical Bacillus Calmette-Guérin in high-risk nonmuscle-invasive bladder cancer using an artificial intelligence-powered pathology assay: development and validation in an international 12-center cohort. Eur Urol. 2023; 84(4): 424–32.