(UroToday.com) The American Urological Association's 2025 Annual Meeting, in Las Vegas, Nevada, was host to the Plenary Session: Paradigm-Shifting, Practice-Changing Clinical Trials in Urology. Dr. Mark Tyson presented BOND-003 Cohort C, a Phase 3, Single-Arm Study of Intravesical Cretostimogene Grenadenorepvec for High-Risk BCG-Unresponsive Non-Muscle Invasive Bladder Cancer with Carcinoma in Situ.
Cretostimogene grenadenorepvec is a conditionally replicating, highly immunogenic adenovirus regulated by the human E2F-1 promoter, enabling selective targeting of tumors with RB-E2F pathway alterations. It also encodes the GM-CSF transgene. The virus binds to the Coxsackie adenovirus receptor (CAR), which is expressed across all stages of bladder cancer. As an oncolytic immunotherapy, it exerts a dual mechanism of action: viral replication induces tumor lysis and stimulates a robust immune response.1,2

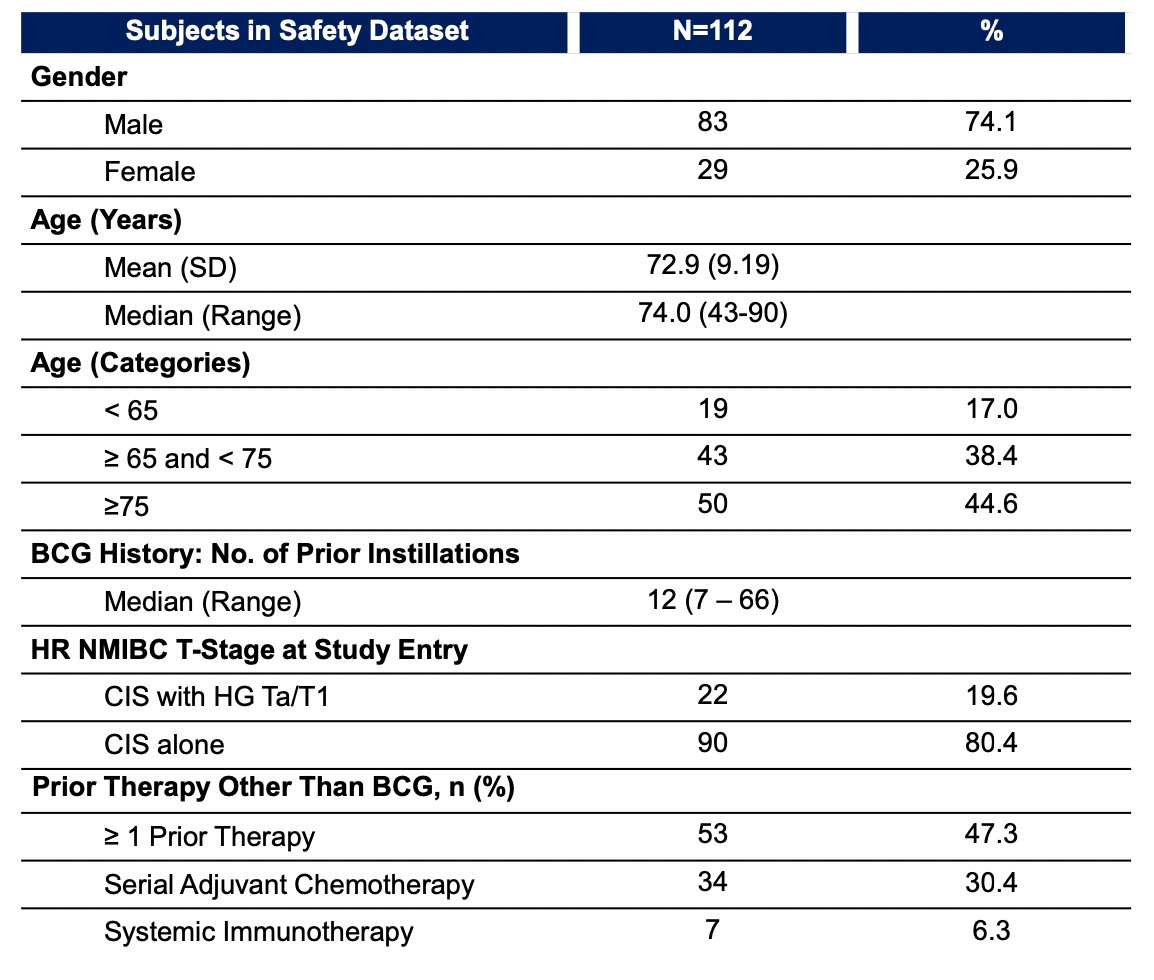
BOND-003 (NCT04452591) is a phase 3 study evaluating cretostimogene grenadenorepvec monotherapy in patients with high-risk BCG-unresponsive NMIBC with CIS. A total of 112 patients were enrolled, all with pathologically confirmed high-risk BCG-unresponsive NMIBC with CIS, with or without high-grade Ta/T1 disease. All high-grade Ta/T1 tumors were resected prior to treatment. Patients received an induction course of cretostimogene administered weekly for six weeks, with a second induction course offered to non-responders. Maintenance therapy was given weekly for three weeks every three months during the first year, and every six months during years two and three. The primary endpoint was complete response (CR) at any time. Key strengths of the study included a central pathology review and the requirement for mandatory biopsies at 12 months. Study schema is shown below:

Dr. Tyson highlighted that the majority of patients enrolled were male (74%), white (62%), and over 65 years of age (83%). While the trial included some underrepresented minorities, most participants were from the United States (63.4%). This was a highly pretreated population, with 41% of patients having received prior chemotherapy.
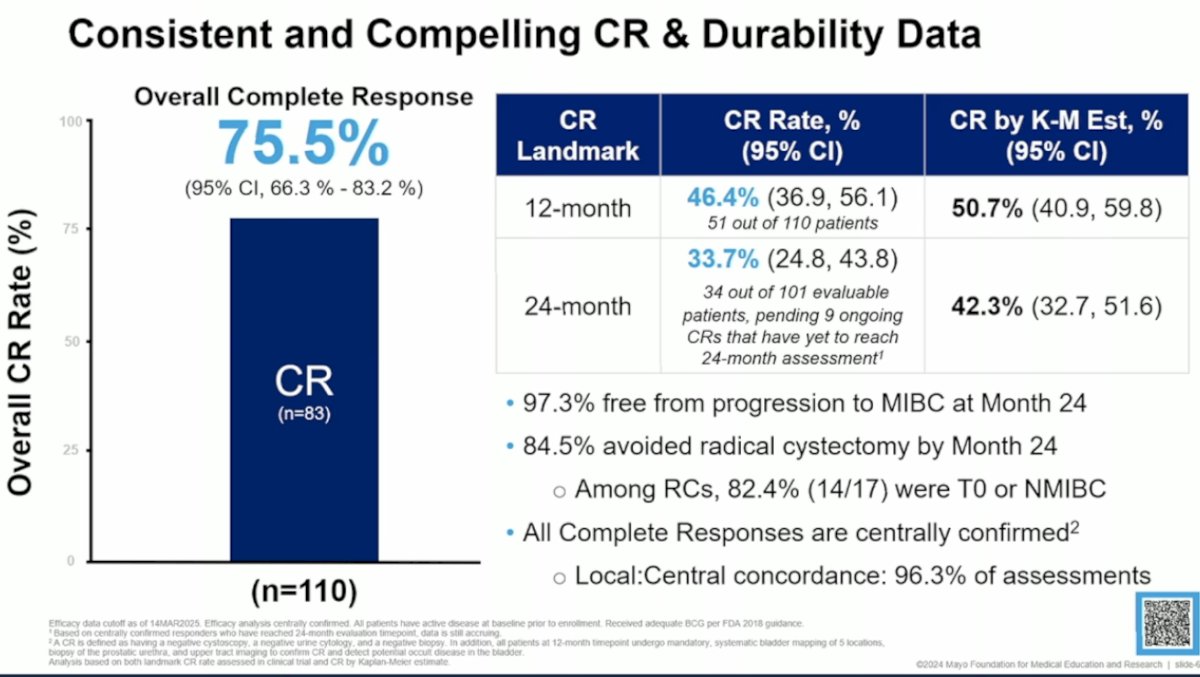
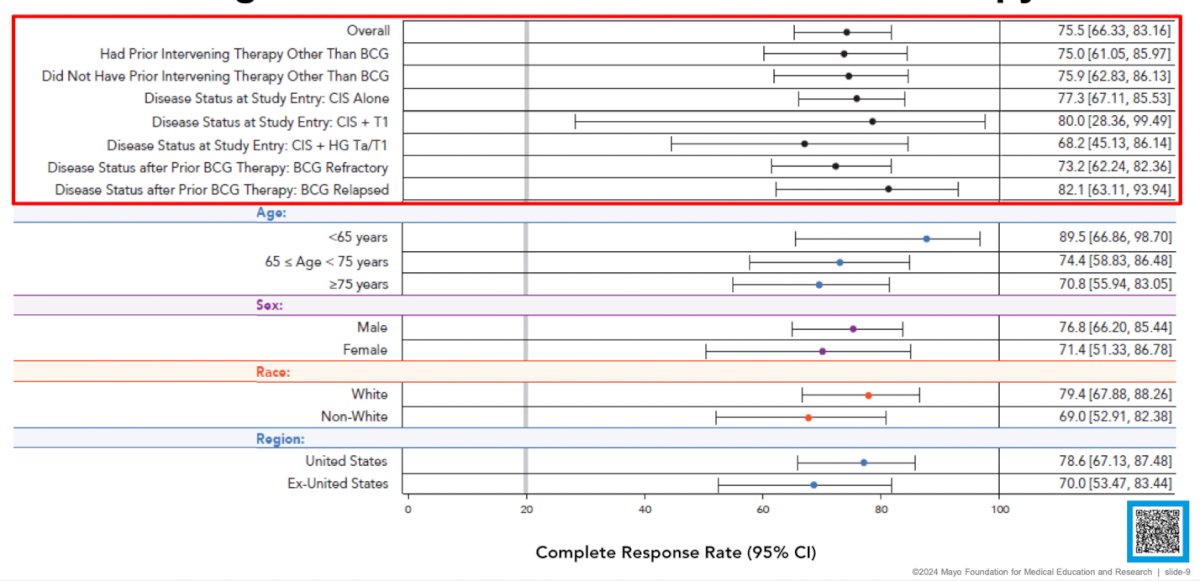
The overall complete response (CR) rate was 75.5%, with 46.4% of patients maintaining a CR at 1 year and 33.7% at 2 years. At 24 months, 97.3% of patients were free from progression to muscle-invasive bladder cancer (MIBC), and 84.5% had avoided radical cystectomy, highlighting the bladder-sparing potential of cretostimogene. Among patients who underwent radical cystectomy, 82.4% (14 out of 17) had either pT0 or non–muscle-invasive disease. All complete responses were centrally confirmed, and there was a high concordance with central pathology review, supporting the strong trial execution and validity of the findings.
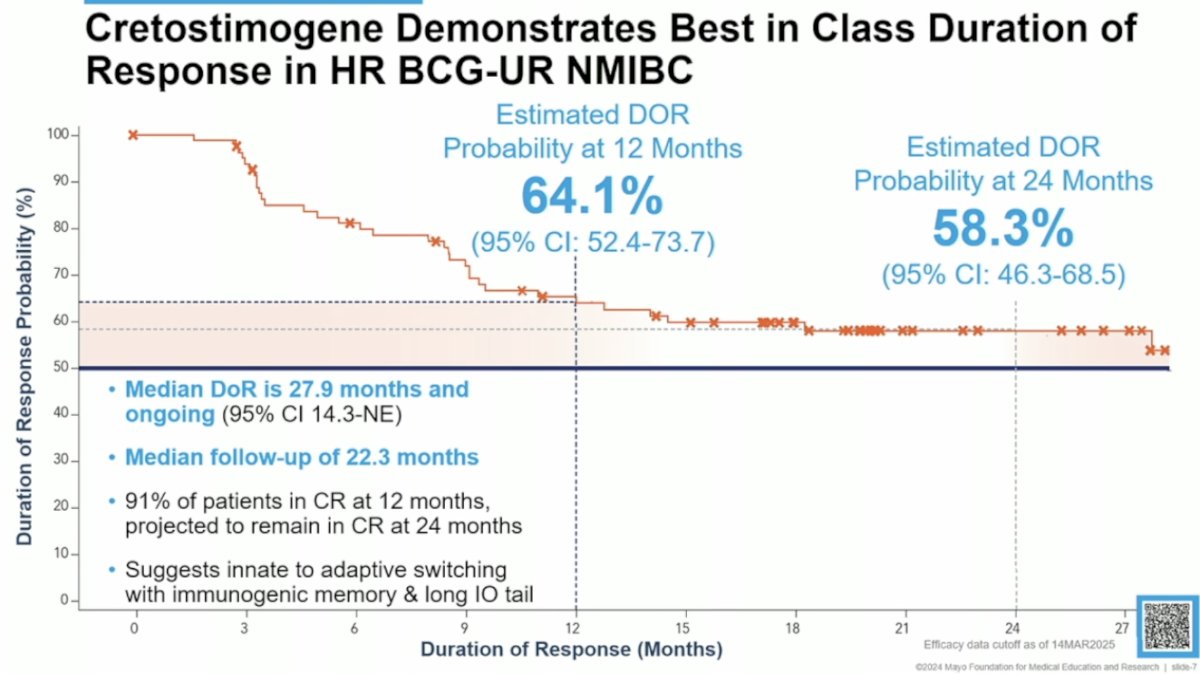
At 1 year, 64.1% of patients maintained their response, and 58.3% maintained it at 2 years. The median duration of response (DoR) was 27.9 months and ongoing (95% CI: 14.3–not estimable). The median follow-up was 22.3 months. Among patients who achieved a complete response at 12 months, 91% were projected to remain in CR at 24 months. These results suggest a durable immunological response, with a potential switch from innate to adaptive immunity and the development of immunologic memory, supporting the observation of a long "tail" in outcomes.
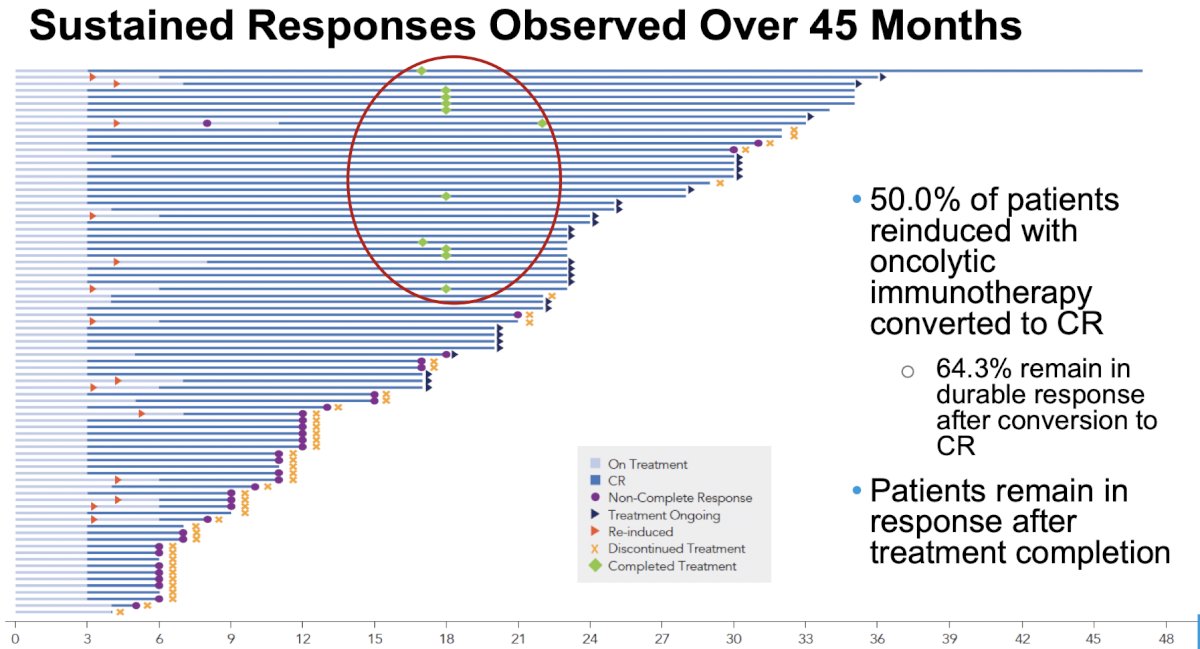
Among patients who were reinduced with oncolytic immunotherapy, 50.0% converted to a CR, and 64.3% of those maintained a durable response after conversion. Notably, many patients remained in response even after completing treatment, as illustrated by the green bars representing patients who finished therapy.
There was minimal variation in CR rates, with high CR rates consistent across patient subgroups, including those previously treated with chemotherapy, those with an exhausted tumor microenvironment, and those with high-risk T1 tumors.
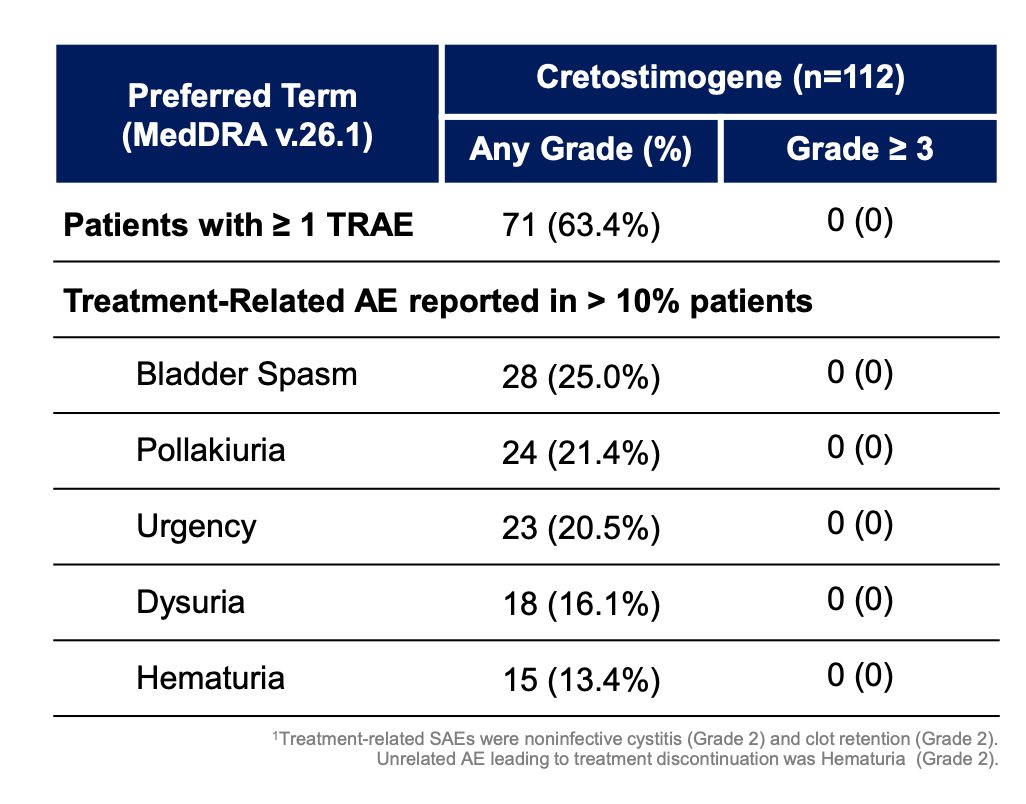
Treatment was favorable and well tolerated, with most adverse events (AEs) being grade 1–2. There were no grade ≥3 treatment-related adverse events (TRAEs) or treatment-related deaths. The median time to TRAE resolution was just 1 day, and no patients discontinued treatment due to adverse events. Only 1.8% (n=2) experienced serious treatment-related AEs (both grade 2). Overall, 97.3% of patients received all protocol-defined treatments.
The investigators assessed viral replication and transgene expression, finding that cretostimogene replication and GM-CSF expression are closely linked. Urine levels of the virus peaked immediately after instillation and were locally sustained for 4–5 days, demonstrating effective payload delivery. No systemic viral shedding was detected at any timepoint, and blood levels of the virus (BLOD) remained undetectable. A stable antibody response, including anti-I5 antibodies, correlated with positive clinical outcomes and reinforced observations from the earlier V-0046 phase 1 study
Sneak peak data from cohort P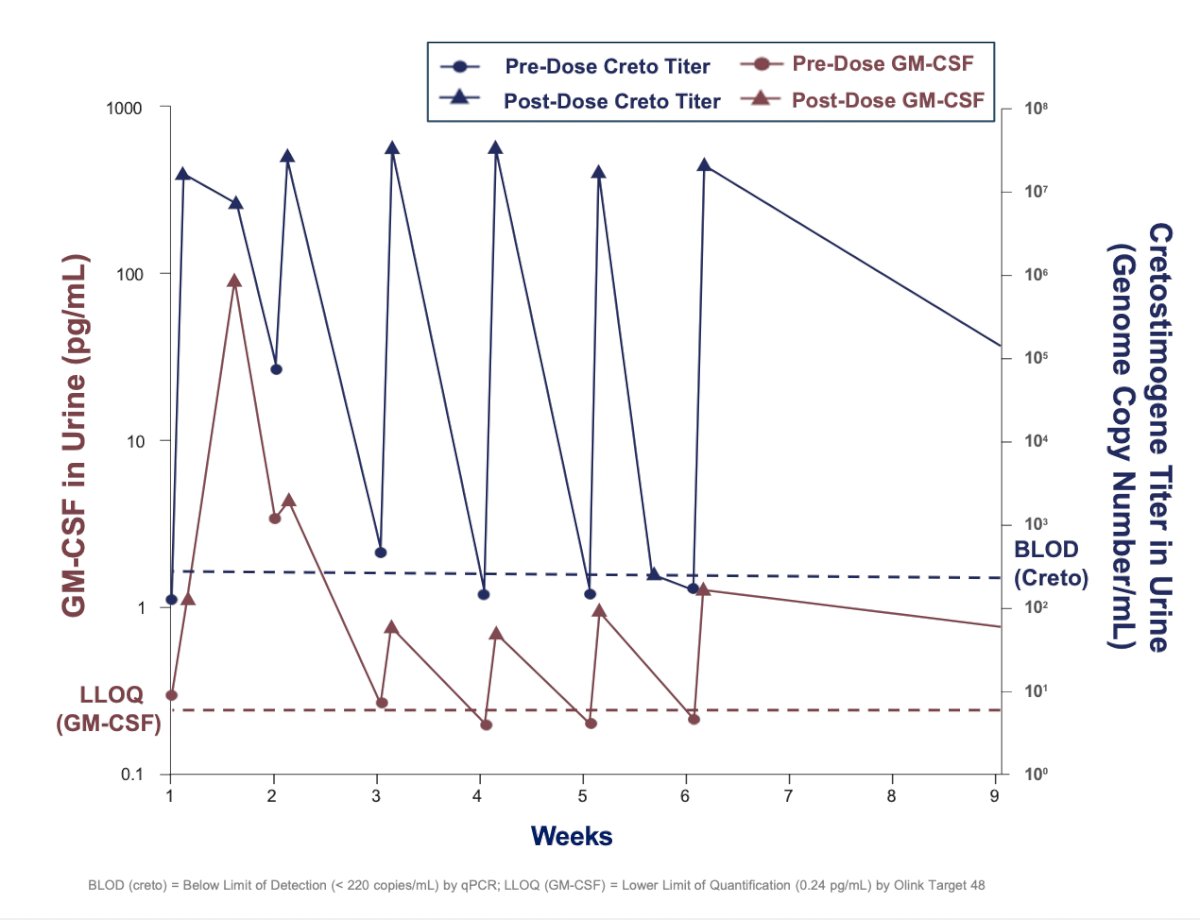
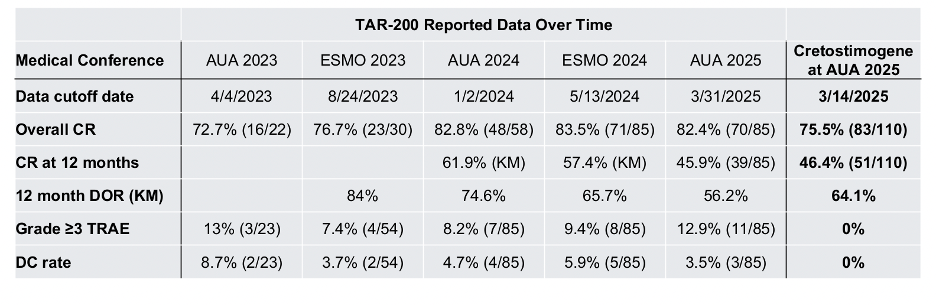
In addition to the updated cretostimogene data presented at AUA, updated data from TAR-200 were also presented with the following side by side comparison: 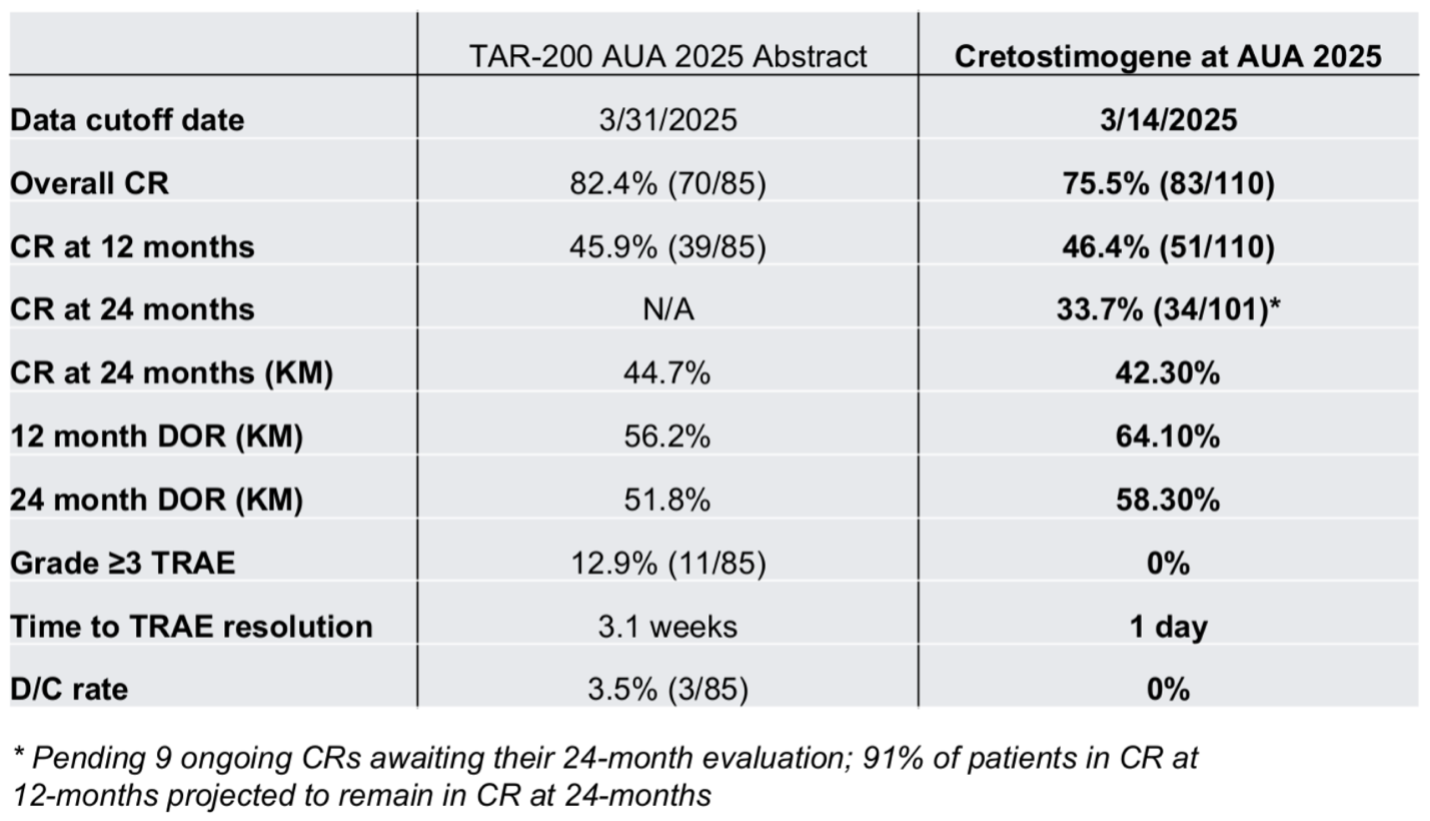
A timeline of TAR-200 and cretostimogene reported data was presented at AUA 2025, highlighting comparable overall complete response rates and a higher 1-year duration of response for Cretostimogene, as shown below.
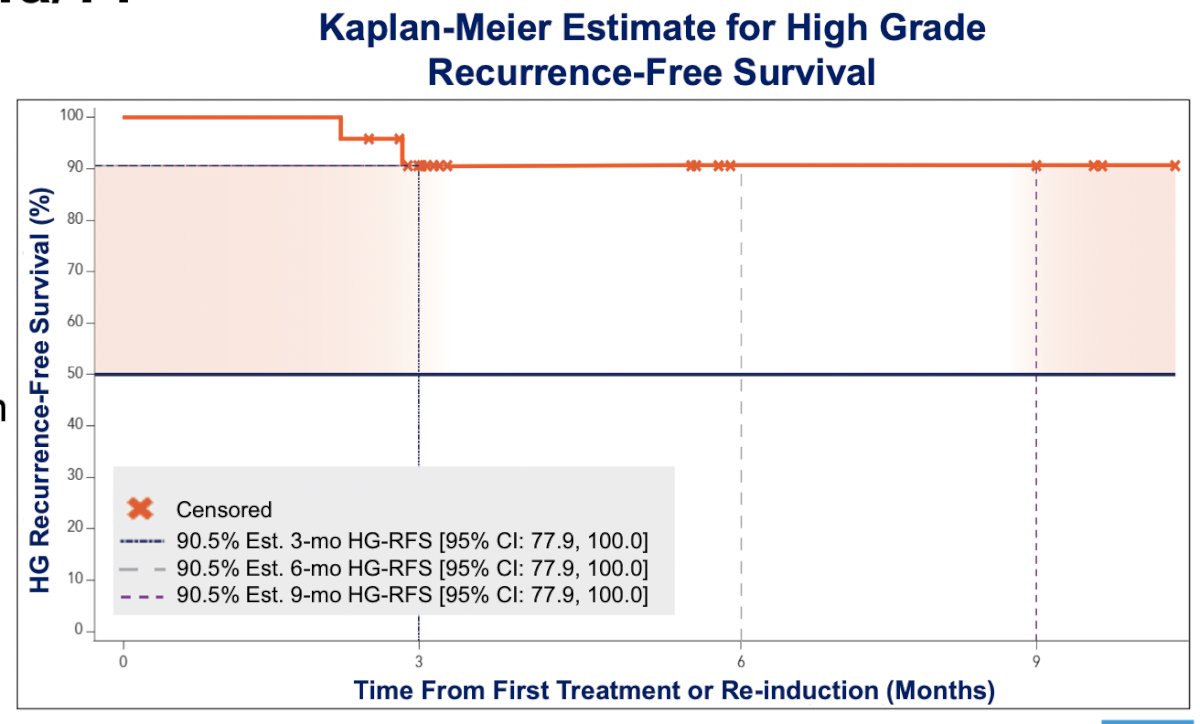
Dr. Tyson provided a sneak peek at the first results from the BOND-003 Cohort P, which included patients with high-risk NMIBC who were BCG-unresponsive with high-grade Ta/T1 disease. Data from the first 24 treated patients showed strong early responses, with a 90.5% high-grade recurrence-free survival (HG-RFS) rate (95% CI: 77.9–100%) at both 3 and 9 months. The regimen was very well tolerated, with a consistent safety profile, no SAEs related to cretostimogene, and no treatment discontinuations due to cretostimogene.
Dr. Tyson wrapped up his presentation with the following key takeaways:
- Cretostimogene grenadenorepvec demonstrated a highly effective and very well-tolerated treatment regimen
- Showed best-in-class durability and tolerability among therapies for BCG-unresponsive NMIBC
- Induced a robust and stable anti-tumor immune response
- Effective even in a heavily pretreated BCG-unresponsive CIS-containing cohort
- Easily integrated into clinical workflows, administered by medical assistants and nurses
- Future and ongoing trials are evaluating cretostimogene both as monotherapy and in rational combinations as a backbone therapy for NMIBC
Presented by: Mark Tyson II, MD, MPH, urologic oncologist and Associate Professor of Urology with the Mayo Clinic Alix School of Medicine in Scottsdale, Arizona, United States.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
Related content: BOND-003 Cohort C Trial Results for Cretostimogene Grenadenorepvec in BCG-Unresponsive Bladder Cancer - Mark Tyson
References:
- Burke JM, Lamm DL, Meng MV, et al. A first in human phase 1 study of CG0070, a GM-CSF expressing oncolytic adenovirus, for the treatment of nonmuscle invasive bladder cancer. J Urol. 2012; 188(6):2391-7.
- Sachs MD, Rauen KA, Ramamurthy M, et al. Integrin αv and coxsackie adenovirus receptor expression in clinical bladder cancer. Urology. 2002; 60(3):531-6.