(UroToday.com) The American Urological Association (AUA) 2025 Annual Meeting, held in Las Vegas, NV, between April 26th and 29th, 2025, was host to a non-invasive bladder cancer interactive poster session. Dr. Sam Chang presented the results of a multicenter study of a Computational Histology Artificial Intelligence (CHAI) biomarker to enhance the risk stratification of high-grade Ta non-muscle invasive bladder cancer (NMIBC).
Consensus is lacking regarding the appropriate risk classification for patients with HG Ta NMIBC, with conflicting definitions of risk across the AUA/SUO, EAU, and IBCG guidelines.1-3 Biomarkers accurately prognosticating risk of recurrence and progression for this heterogeneous patient population could have an immediate impact on personalized disease management.
A previous analysis of 944 patients with high-risk NMIBC treated with BCG demonstrated that signatures derived from histologic features analyzed with the Computational Histologic Artificial Intelligence (CHAI) platform identified patients at increased risk of recurrence, progression, and BCG-unresponsive disease.4 The study investigators hypothesized that the previously developed CHAI biomarkers could stratify the risks of recurrence and progression in patients with HG Ta NMIBC better than existing guideline risk groupings.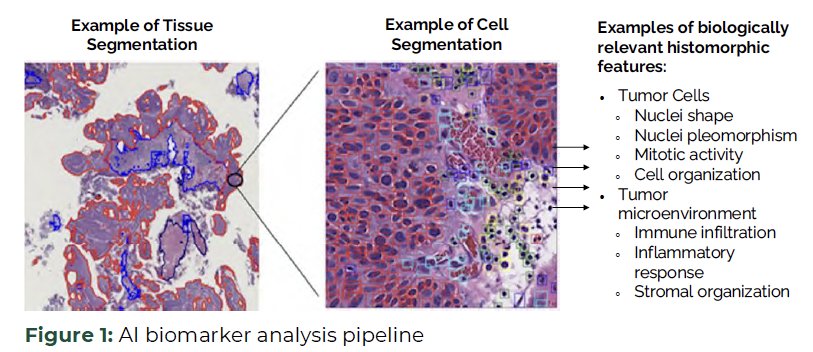
The study inclusion criteria were as follows:
- BCG-naive HG Ta NMIBC treated with adjuvant intravesical BCG post-TURBT between 2004 and 2024
- Available digital slide images from pre-treatment bladder tumor
- Never analyzed in CHAI biomarker development
The image processing was as follows:
- Whole slide images (WSI) were analyzed using the CHAI platform.
- HG recurrence-free survival (RFS) endpoint was assessed using the locked AI pathology biomarker component +/- multifocality.
- Muscle-invasive bladder cancer progression-free survival (MIBC-PFS) was assessed using the AI pathology component only.
From a statistical standpoint, Cox proportional hazards (CPH) models were used to evaluate the degree of association of each model’s risk grouping with the endpoints. Kaplan-Meier curves and corresponding log-rank statistics, as well as McNemar’s test for paired nominal data, were used.
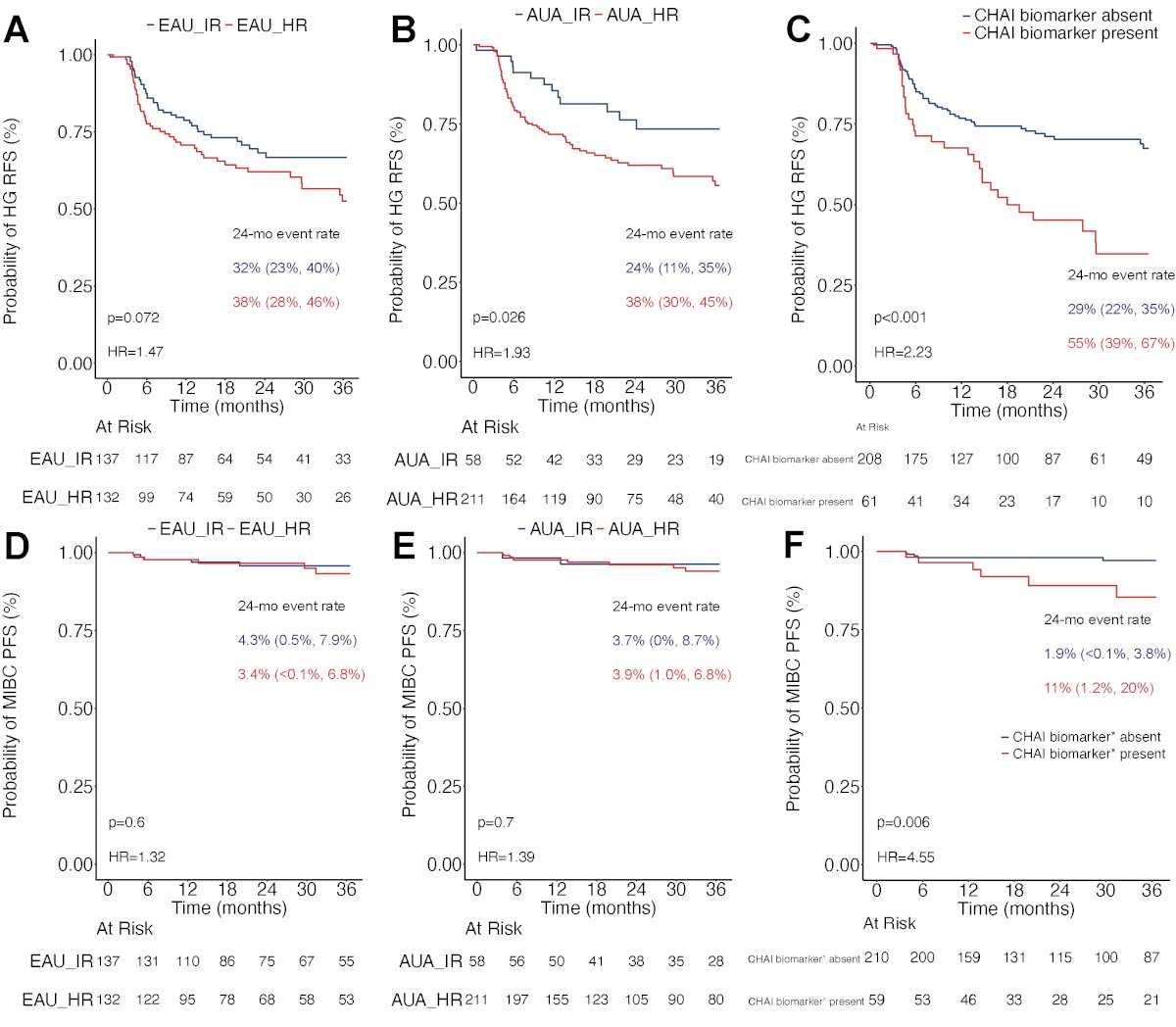
WSI from 269 patients with HG Ta NMIBC were included. The median follow-up was 32 months (IQR: 14–52). The summary results of HG-RFS and MIBC-PFS, stratified by AUA, EAU guidelines, and CHAI biomarkers, are illustrated below.
Briefly, the results are summarized as follows:
- EAU risk stratification was not significantly associated with HG-RFS (HR: 1.47, 95% CI: 0.96–2.23, p=0.074).
- AUA risk stratification was significantly associated with HG-RFS (HR: 1.93, 95% CI: 1.07– 3.48, p=0.029).
- CHAI biomarker was significantly associated with HG-RFS (HR: 2.23, 95% CI: 1.45–3.44, p<0.001).
- EAU risk stratification was not significantly associated with MIBC-PFS (HR: 1.32, 95% CI: 0.40–4.32, p=0.7).
- AUA risk stratification was not significantly associated with MIBC-PFS (HR: 1.39, 95% CI: 0.30–6.44, p=0.7).
- CHAI biomarker was significantly associated with MIBC-PFS (HR: 4.55, 95% CI: 1.39–14.92, p=0.012).
These results reaffirm that the HG Ta NMIBC patient population is heterogeneous, with a wide range of risks, treatment possibilities, and outcomes. Depending on which current guidelines are utilized in practice (e.g. AUA/SUO, EAU, IBCG), the risk stratification for patients with HG Ta NMIBC will vary, making guideline-concordant care difficult to administer.
This multicenter study evaluated AI-based histologic biomarkers previously validated in high-risk disease to prognosticate recurrence and progression risks for this borderline group. The presence of high-risk prognostic CHAI biomarkers indicated significantly higher risks of high-grade recurrence and muscle-invasive progression, outperforming existing AUA and EAU risk model groupings.
Study limitations included the retrospective design and comparison to an EAU risk stratification model focused on progression risk from a historical population that did not receive BCG maintenance therapy.
Dr. Chang concluded that CHAI biomarkers enable more personalized medicine in NMIBC, providing accurate prognostic scores to assess each patient’s risk of recurrence and progression, even in an HG Ta NMIBC population, where current guidelines disagree on the level of risk.
Presented by: Sam Chang, MD, MBA, Patricia and Rodes Hart Professor of Urologic Surgery, Department of Urology, Vanderbilt University Medical Center, Nashville, TN
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
References:
- Babjuk M, Burger M, Capoun O, Cohen D, Compérat EM, Dominguez-Escrig JL, et al. European Association of Urology Guidelines on Non–muscle-invasive Bladder Cancer (Ta, T1, and Carcinoma In Situ) – 2022 Update. Eur Urol. 2022;81(1):75–94.
- Holzbeierlein J, Weizer A, Smith A, Carroll P, Porter M, Chang SS, et al. Contemporary Management of Muscle-Invasive Bladder Cancer. J Urol. 2024;211(4):533–8.
- Tan WS, Sridhar SS, Huddart R, Cathomas R, Choudhury A, Siefker-Radtke A, et al. Neoadjuvant and Adjuvant Systemic Therapy for Muscle-invasive Bladder Cancer. Eur Urol Oncol. 2022;5(5):505–16.
- Lotan Y, Galsky MD, Kamat AM, Pal SK, Rosenberg JE, Shore ND, et al. Bladder Cancer: A Review of Non–muscle-invasive and Muscle-invasive Disease. J Urol. 2025;213(2):192–204.