(UroToday.com) The 2025 ASTRO annual meeting featured a biomarker breakthroughs in prostate cancer session and a presentation by Dr. Abdenour Nabid discussing testosterone recovery post ADT in intermediate risk prostate cancer patients. For patients with unfavorable intermediate-risk prostate cancer undergoing primary radiotherapy to the prostate, a short course of ADT often accompanies radiotherapy. Both testosterone recovery rates and outcomes amongst those who do and do not recover their testosterone are limited. Using data from a randomized phase III trial in intermediate risk prostate cancer, the investigators compared overall survival between two different doses of prostate radiotherapy by patients stratified with or without testosterone recovery after ADT.
From October 2000 to January 2008, 600 patients with intermediate risk prostate cancer were randomized to 6 months of ADT + radiotherapy 76 Gy or radiotherapy 70 Gy vs radiotherapy alone (76 Gy). The 400 patients treated with ADT were selected for this analysis. Serum testosterone was measured at baseline, then regularly. Testosterone recovery was defined as a return of testosterone to within the normal range value. Overall, 19 patients were excluded: 2 not receiving exactly 6 months of ADT, 5 not receiving 70 or 76 Gy, and 12 with no testosterone available at baseline or during follow-up. Over a period of 23 years, 4,779 testosterone measurements were available. Using log rank test, overall survival was compared between patients with or without testosterone recovery and between patients receiving 70 or 76 Gy with or without testosterone recovery. Multivariable analysis to predict overall survival included dose of radiotherapy, recovered testosterone, age, Zubrod performance status, comorbidities, baseline PSA, Gleason score, and stage.
There were 381 patients receiving ADT who had proper testosterone data available and were included in the analysis. There were 196 and 185 patients who received 70 Gy or 76 Gy, respectively. The median age was 71 years (IQR 66-74), with the two groups being well-balanced, except for a higher PSA >10 ng/ml in patients treated with 70 Gy radiotherapy (59.2% versus 46.5%, p = 0.013). With a median follow-up of 15.3 years, 291 patients (76.4%) recovered testosterone to normal level with no difference between the 70 Gy or 76 Gy cohorts (76.5% versus 76.2%, p = 0.94). The median time to testosterone recovery was 1.64 (IQR 1.41-2.28) years, similar between 70 Gy (1.6 (IQR 1.4-2.1) or 76 Gy 1.7 (IQR 1.4-2.6), p = 0.084: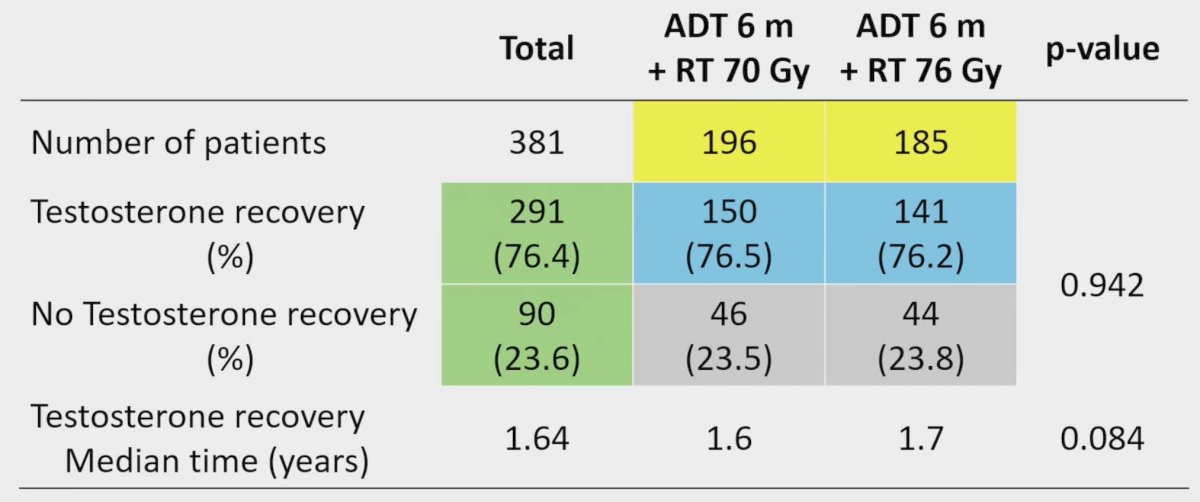
There was no difference seen in overall survival between patients receiving 76 Gy compared to 70 Gy (HR 1.06, 95% CI 0.80-1.39, p = 0.70):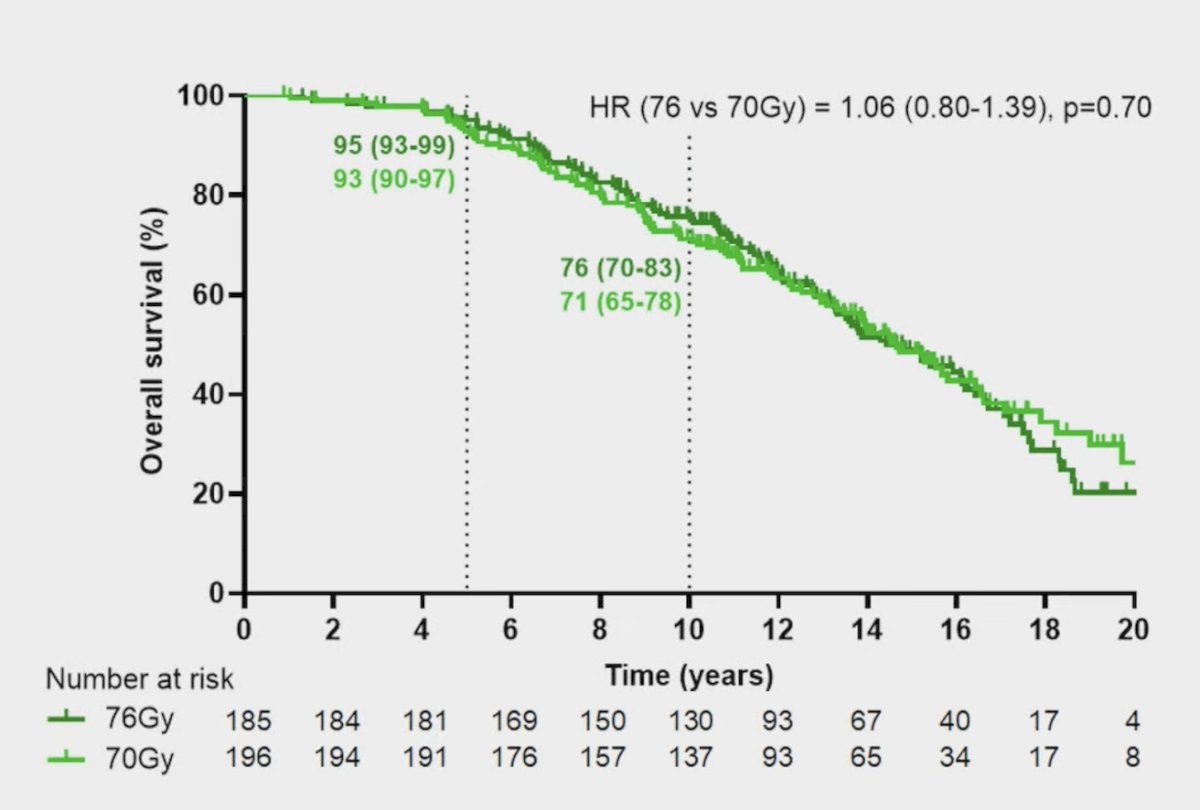
A significantly lower risk of death favored patients recovering testosterone (HR 0.53, 95% CI 0.39-0.73, p < 0.001):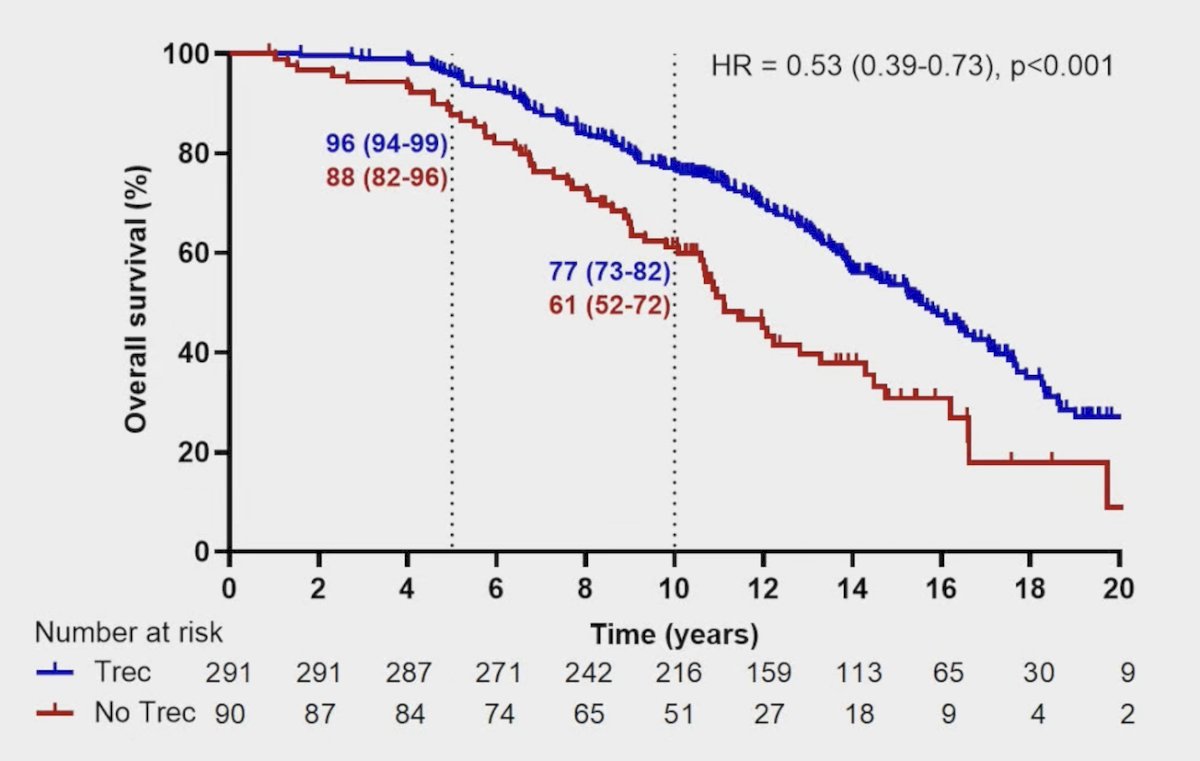
No significant difference was seen in overall survival between patients receiving 76 Gy or 70 Gy with testosterone recovery (HR 0.94, 95% CI 0.68-1.30, p = 0.72):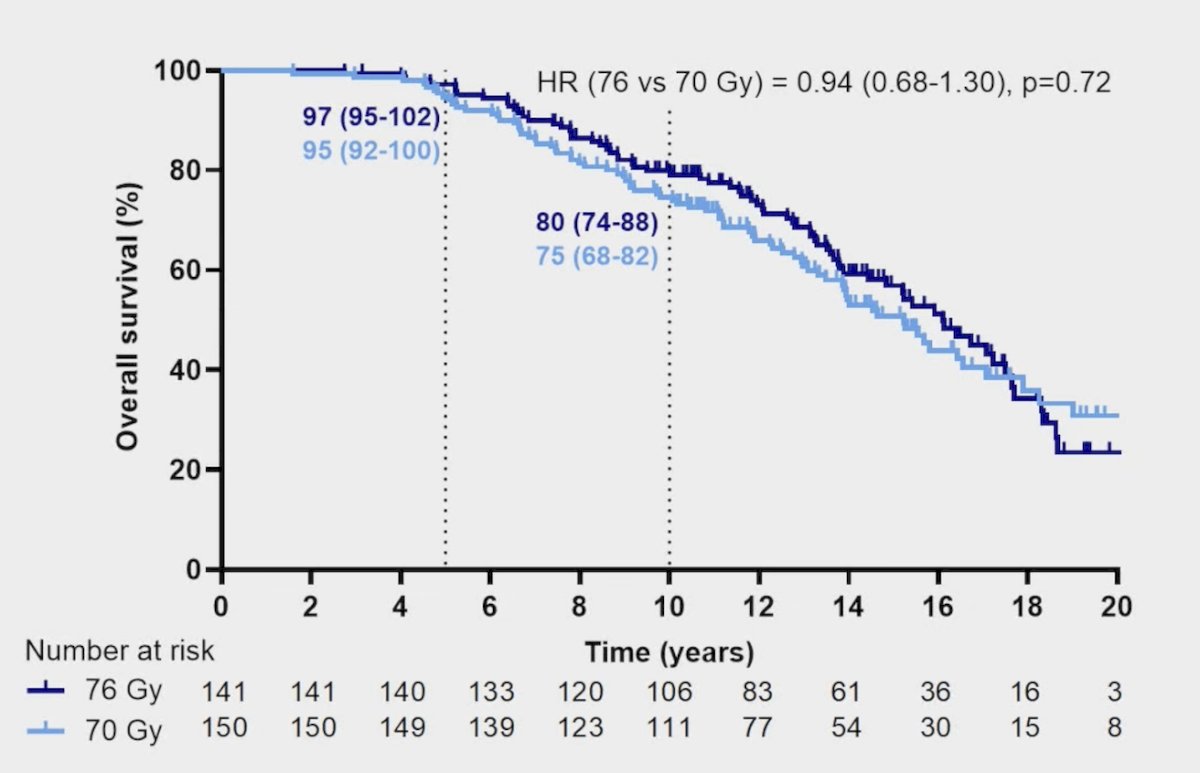
Similarly, there was no significant difference seen in overall survival between patients receiving 76 Gy or 70 Gy without testosterone recovery (HR 1.46, 95% CI 0.86-2.47, p = 0.16):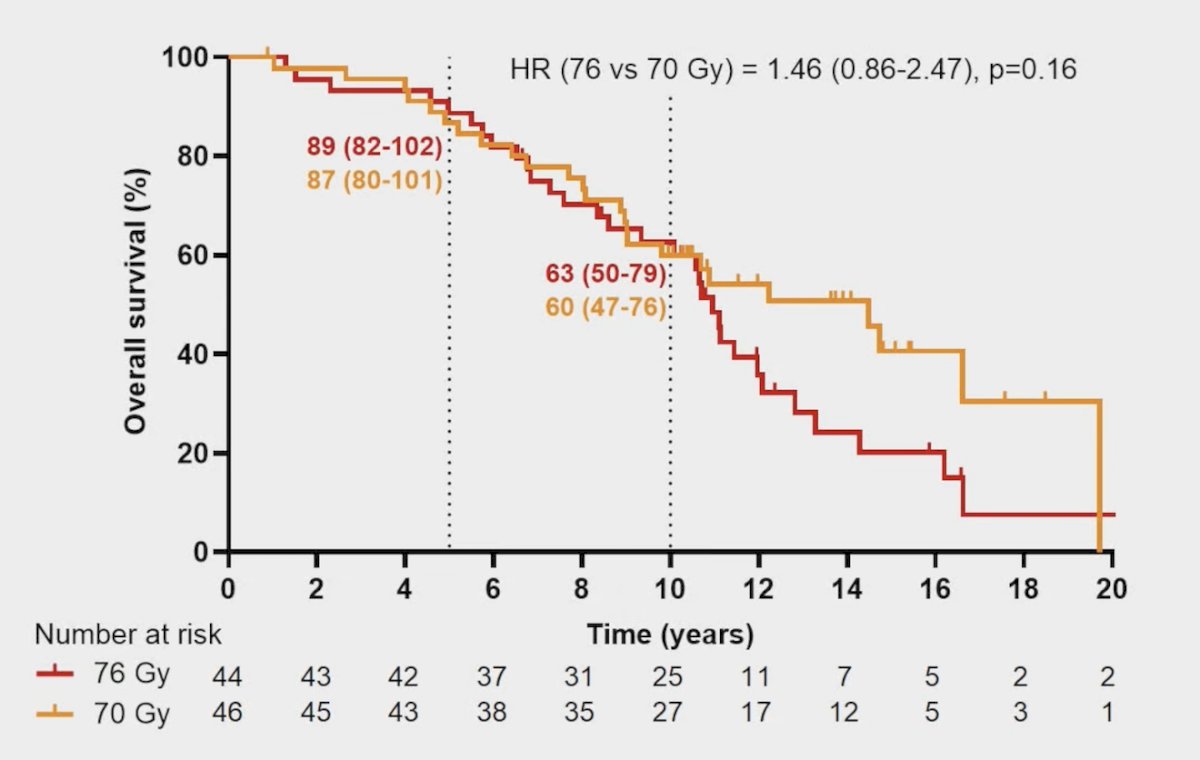
On multivariable analysis, dose of radiotherapy remained non-significant for overall survival (HR 1.00, 95% CI 0.76-1.33). Testosterone recovery (HR 0.63, 95% CI 0.45-0.87, p = 0.006), as well as Zubrod (HR 1.93, 95% CI 1.20-3.10), age (HR 1.04, 95% CI 1.02-1.07), COPD (HR 1.82, 95% CI 1.17-2.82) and baseline PSA > 10 ng/mL (HR 1.48, 95% CI 1.05-2.07) played a significant role in overall survival:
Dr. Nabid concluded this presentation discussing testosterone recovery post ADT in intermediate risk prostate cancer patients with the following take-home points:
- In intermediate risk prostate cancer patients randomized to short-term ADT and either 70 Gy or 76 Gy, testosterone recovery to normal level is associated with a significant improvement in overall survival, likely by protecting patients from the ill effects of persistent castration
- Delivering a higher dose of radiotherapy to the prostate had no impact on overall survival, regardless of testosterone status
Dr. Nabid noted that this study was recently accepted to the Red Journal for publication.
Presented by: Abdenour Nabid, MD, CHUS, Sherbrooke, Quebec, Canada
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, Sat, Sept 27 – Wed, Oct 1, 2025.