(UroToday.com) The 2025 ASTRO annual meeting featured a localized prostate cancer session and a presentation by Dr. Alexander Goglia discussing results of a prospective phase II trial of a short course androgen deprivation, pelvic stereotactic body radiotherapy, and brachytherapy boost for NCCN high-risk prostate cancer with low-intermediate risk Decipher genomic score. The NCCN high risk category accounts for roughly 30% of all newly diagnosed cases of localized prostate cancer. While these patients are at higher risk of recurrence, distant metastasis, and death, more than 70% of high risk patients treated with definitive radiotherapy and ADT never develop metastatic disease. These findings suggest that there is a group of high risk patients whose disease biology does not match their NCCN risk category and are thus being over-treated. Pitfalls with the NCCN risk groups include (i) that the T-stage relies on DRE, (ii) shortcomings of PSA, (iii) subjectivity of Gleason scoring, and (iv) inadequacy of imaging for staging. The Decipher genomic classifier is a gene expression-based assay commonly used as an additional risk stratification tool, with prognostic value that has been retrospectively validated but has not yet been studied prospectively. The objective measures to identify patients who are fit for de-intensification are as follows:
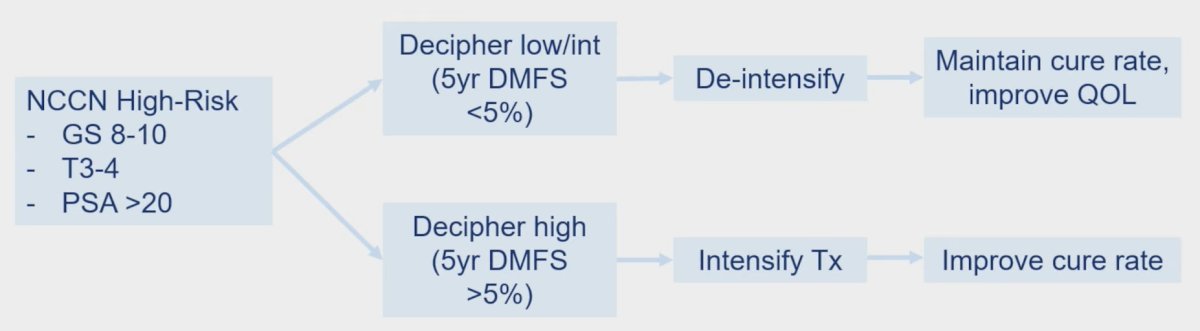
Dr. Goglia and colleagues hypothesized that low/intermediate risk Decipher genomic classifier scores could identify patients with NCCN high-risk prostate cancer that are suitable for de-intensification of ADT (ie. 6 months) and a compressed course of radiation therapy (ie. 15 Gy HDR boost + hypofractionated pelvic external beam radiotherapy, 25 Gy / 5fx).
This single arm, phase II prospective study enrolled 50 patients with a Decipher genomic classifier score <=0.6 and localized, high-risk prostate cancer defined as Gleason grade group 4 or 5, PSA > 20 ng/mL, or cT3-4N0M0. Patients were treated with 6 months of neoadjuvant/concurrent/adjuvant ADT (leuprolide + bicalutamide) combined with a single 15 Gy Ir-192 HDR brachytherapy implant followed by 25 Gy in 5 daily fractions whole pelvis stereotactic body radiotherapy:

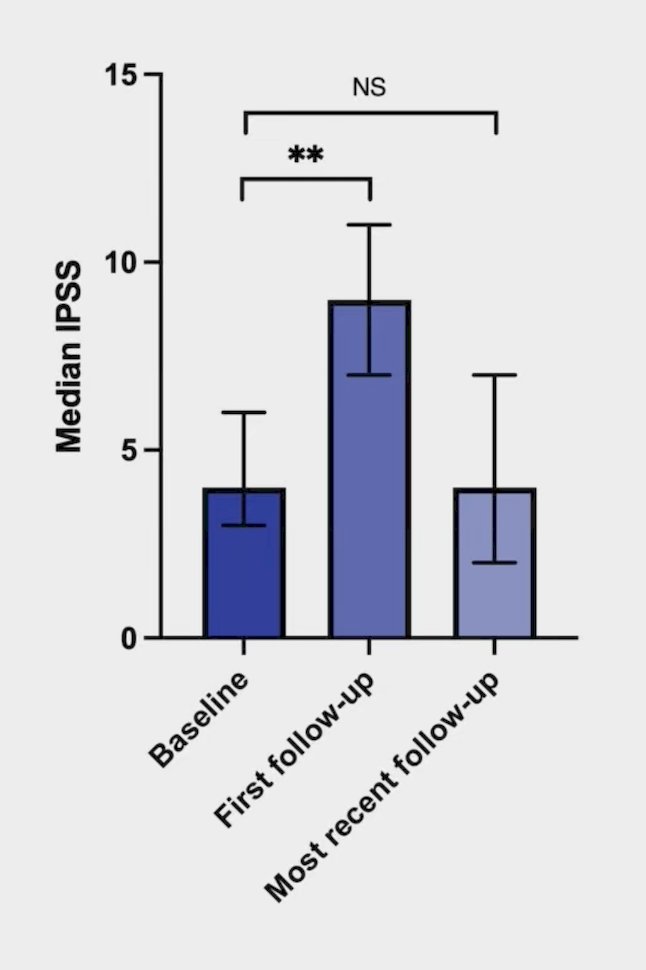
The primary endpoint was 3-year metastasis rate. Only early toxicity (CTCAE v5.0), International Prostate Symptom Score (IPSS), and biochemical recurrence rate (defined as PSA nadir + 2 ng/mL) are reported.
The median age of enrolled patients was 68.5 years old, with a median Decipher genomic classifier score of 0.405 (95% CI 0.361 – 0.433), and median baseline PSA of 6.83 (95% CI 5.98 - 8.77) ng/mL. Pre-treatment MR imaging showed PIRADS 4 or 5 lesions in 84% of enrolled patients (42/50), and pre-treatment biopsies showed Gleason grade group 4 or 5 disease in 64% of patients (32/50). The median follow-up across all enrolled patients was 22 months (95% CI 19.69 – 23.55), and thus, only early secondary endpoint outcomes are reported. Median baseline IPSS was 4.0 (95% CI 3.93 - 6.15), while median IPSS at first follow up was 9.0 (95% CI 7.73 - 11.35) and at most recent follow up was 4.0 (95% CI 4.33 - 7.15):
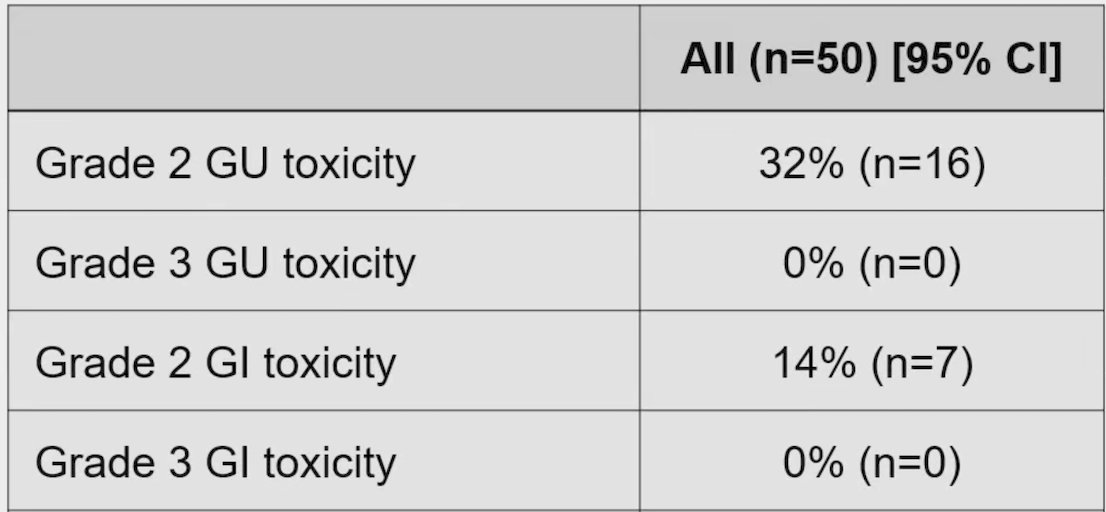
Grade 2 genitourinary toxicity was seen in 32% of patients (16/50), while grade 2 gastrointestinal toxicity was seen in 14% of patients (7/50). No grade 3 or higher toxicities were seen:
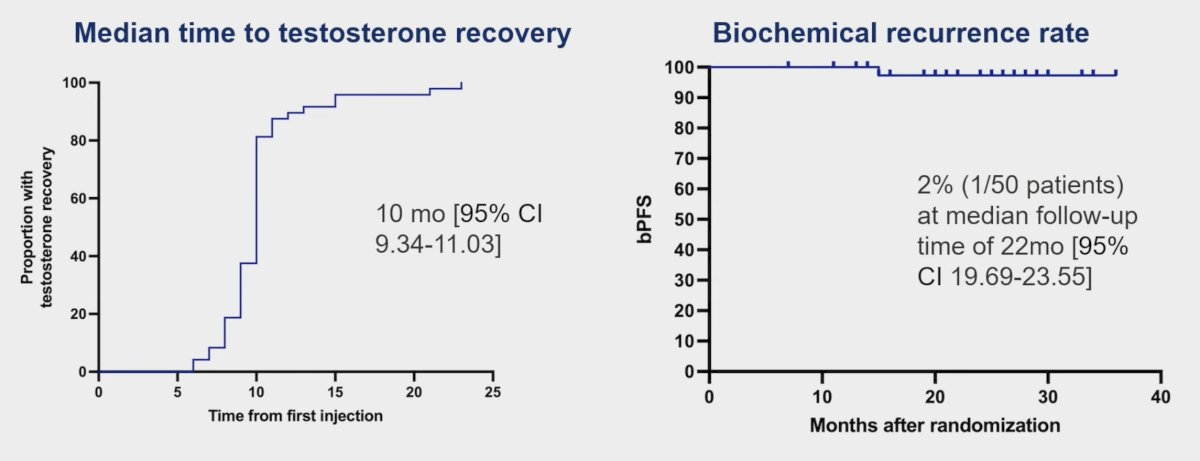
The median time to testosterone recovery was 10 months (95% CI 9.34 - 11.03), and the rate of biochemical recurrence was 2% (1/50):
Dr. Goglia concluded his presentation discussing results of a prospective phase II trial of a short course androgen deprivation, pelvic stereotactic body radiotherapy, and brachytherapy boost for NCCN high-risk prostate cancer with low-intermediate risk Decipher genomic score, with the following take home points:
- Thus far, this trial has observed low genitourinary/gastrointestinal toxicity, preserved genitourinary quality of life, and encouraging early oncological outcomes with a shorter course of ADT and radiotherapy for genomically lower risk, NCCN high-risk prostate cancer patients
- Longer follow-up is needed to report the primary endpoint of 3-year metastasis-free survival
Presented by: Alexander Goglia, MD, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, September 28th – 30th, 2025.