(UroToday.com) The 67th American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco between September 28 and September 30 was host to the Session QP 13 - GU 7: Quick Pitch: Optimizing Treatment of Recurrent Prostate Cancer. Dr. Adam Eakin presented abstract 1074 - Implications on Radiation Treatment Planning of 18F-Fluciclovine PET/CT in Patients with Biochemical Recurrence of Prostate Cancer and a Negative PSMA PET/CT.
Dr. Eakin began by emphasizing that PSMA PET/CT has become the standard of care for localizing disease in biochemically recurrent (BCR) prostate cancer. However, he highlighted that 18F-fluciclovine (Axumin) PET/CT may be particularly useful in two scenarios: when PSMA PET/CT is negative, and in cases of local recurrence in the prostate bed where detection on PSMA PET/CT may be obscured by urinary activity. To explore this, he presented an ongoing prospective single-arm cohort study (NCT05722925).
In this study, 49 patients with biochemically recurrent (BCR) prostate cancer following definitive treatment were enrolled, including 42.9% who had undergone prostatectomy, 14.3% treated with radiotherapy (RT) alone, 36.7% who had both surgery and RT, and one patient (2%) treated with ADT alone.
All patients had PSA levels ≥0.2 ng/mL and had no definitive site of recurrence identified on PSMA PET/CT, despite all undergoing a PSMA PET scan. Within 30 days of the negative PSMA PET/CT and without receiving cancer treatment in between they underwent 18F-fluciclovine PET/CT. The results revealed that 18F-fluciclovine was positive in 57.1% of patients, identifying local recurrence in 50%, regional metastases in 18%, and distant metastatic disease in 32%.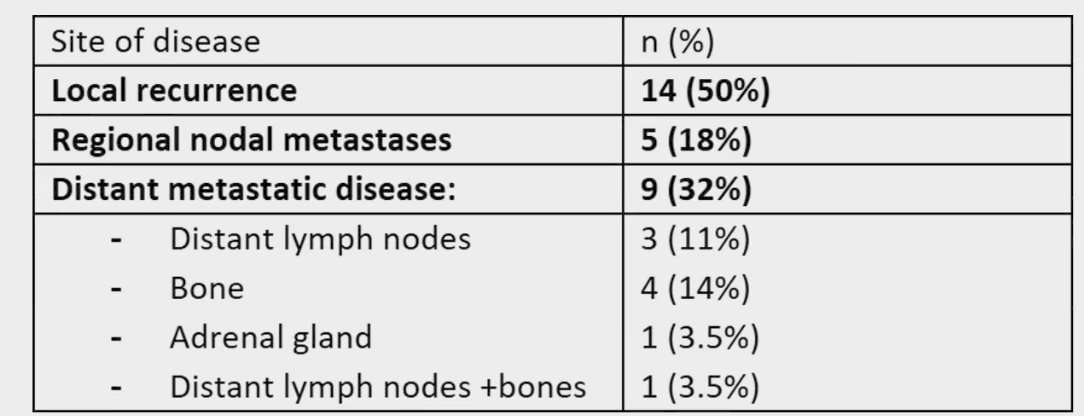
Notably, the investigators found no statistically significant difference in PSA levels between patients with positive and negative 18F-fluciclovine PET/CT scans (p=0.19). Among those with a positive scan, PSA ranged from 0.20–14.75 ng/mL with a median of 0.53 ng/mL, while in patients with a negative scan, PSA ranged from 0.21–4.28 ng/mL with a median of 0.41 ng/mL.
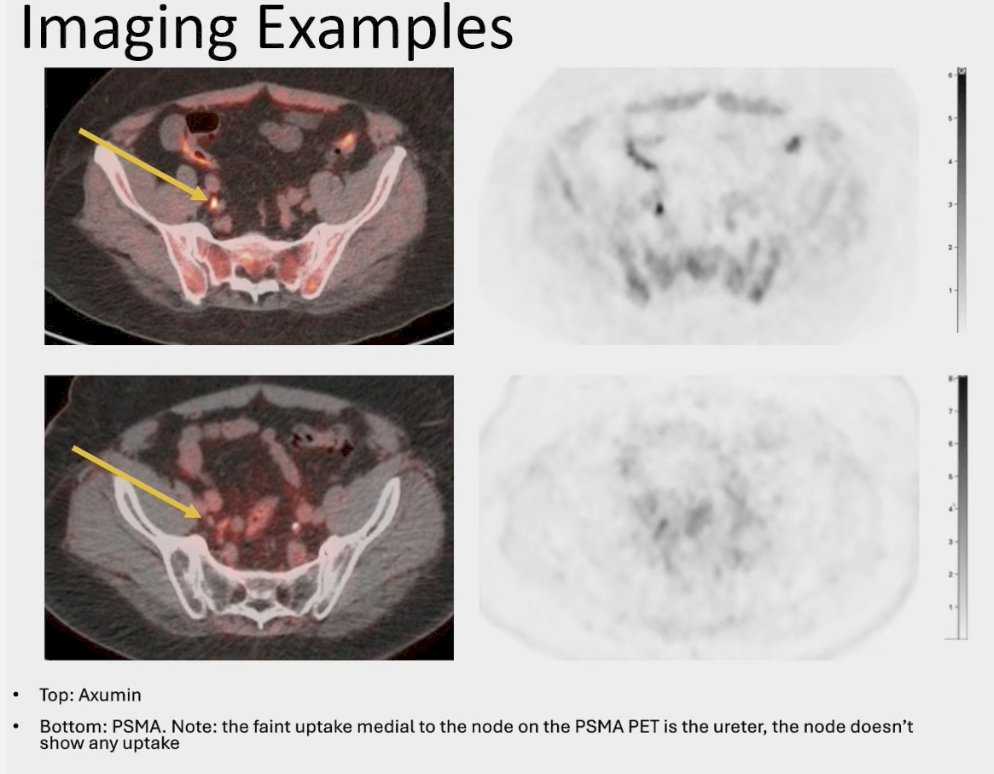
Dr. Eakin presented illustrative cases of patients with PET-avid lymph nodes detected on 18F-fluciclovine (Axumin) PET/CT but not identified on PSMA PET/CT. An example is shown below, with Axumin imaging on the top panel and PSMA PET/CT on the bottom, highlighting situations where fluciclovine may reveal disease sites missed by PSMA imaging.
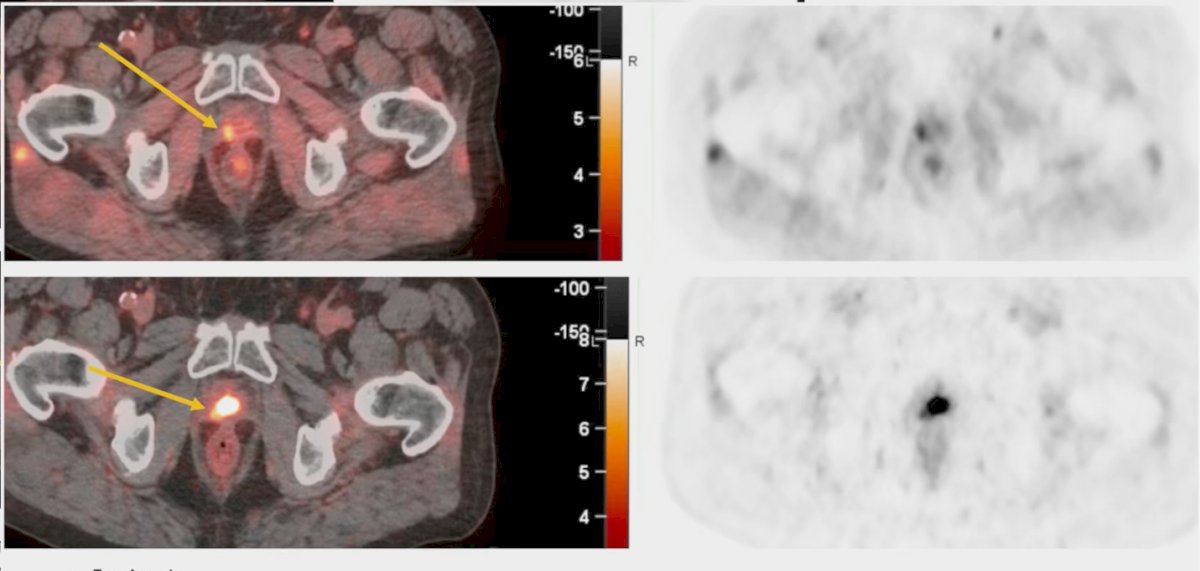
This figure highlights another advantage of 18F-fluciclovine (Axumin) PET/CT compared with PSMA PET/CT. Because Axumin is not excreted through the urine, it avoids the confounding effect of bladder activity, which can obscure local recurrence in the prostate bed. As shown in the case example, recurrent disease is clearly visible on Axumin PET/CT, whereas PSMA PET/CT, obscured by urinary tracer excretion, fails to detect the lesion.
The investigators conducted a subgroup analysis of patients considered for prostate fossa salvage RT after prostatectomy. Among the 20 patients in this group, 11 (55%) had a positive 18F-fluciclovine scan: 7 showed avidity in the prostate fossa, 2 in pelvic lymph nodes, 1 in a retroperitoneal node, and 1 in the ischium. Importantly, 4 of 20 patients (25%) were found to have disease outside of the planned prostate fossa salvage RT field, highlighting the value of 18F-fluciclovine in refining treatment planning and potentially avoiding geographic misses.
Dr. Eakin concluded his presentation by emphasizing the implications of this study. He highlighted that approximately 50% of patients with BCR prostate cancer and a negative PSMA PET/CT may still have disease detected by 18F-fluciclovine PET/CT. This underscores the potential role of fluciclovine PET/CT in refining treatment planning, particularly in patients being considered for post-prostatectomy salvage RT or in identifying oligometastatic disease.
Looking ahead, he noted that a multi-institutional trial is planned to evaluate how management may change when incorporating 18F-fluciclovine PET after a negative PSMA PET, with enrollment expected at around 150 patients.
Presented by: Adam Eakin, MD, PGY-3 resident in the Department of Radiation Medicine at Oregon Health and Science University, Portland, OR
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Cancer Treatment and Research Center (CTIC), Luis Carlos Sarmiento Angulo Foundation via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco between the 28th of September and the 30th of September.