(UroToday.com) The 67th American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco between September 28 and September 30 was host to the Session EDU 34 - ROBIN Oligometastasis (OligoMET) Center: Using Biomarker Correlates from a Prostate Cancer Clinical Trial to Improve Future Outcomes. Dr. Philip Sutera discussed the role of digital pathology-based Multimodal Artificial Intelligence Biomarker Models in Oligometastatic Castration-sensitive Prostate Cancer.
Dr. Sutera opened his talk by outlining that he would divide his presentation into three parts: first, defining MMAI; second, discussing its application in oligometastatic prostate cancer; and third, exploring the concept of “opening the black box” to better understand its potential.
What is MMAI?MMAI is a CLIA/CAP-certified, digital pathology–based multimodal artificial intelligence (AI) prognostic biomarker, developed and validated in localized prostate cancer treated with definitive radiation. The MMAI score is derived from H&E slide image features integrated with clinical data such as PSA, T stage, and age. Pathology slides are broken into image patches that are processed through a pretrained, self-supervised machine learning model to generate feature vectors, which are then combined with clinical variables in a neural network to output the MMAI score. Developed about 18 months ago, MMAI has since gained traction as a novel biomarker platform.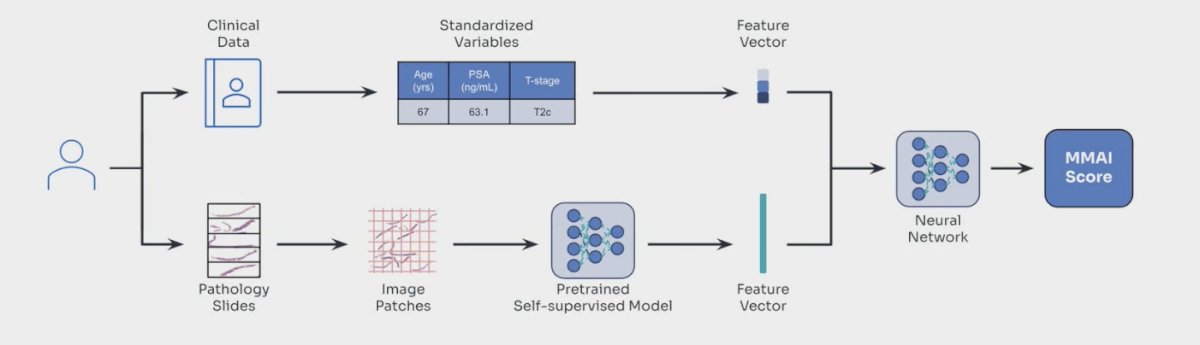
The MMAI biomarker has emerged as a powerful prognostic tool, demonstrating superior risk stratification compared to NCCN grouping across multiple clinically relevant outcomes, including distant metastasis, biochemical failure, PCSS, and OS. (1) It is the only predictive biomarker currently recommended by NCCN in localized prostate cancer and is supported by Simon Level IB evidence. Importantly, it is CMS reimbursed, reinforcing its clinical applicability. As shown in the validation data, MMAI consistently improved AUC across short- and long-term endpoints, while the meta-analysis in high-risk men (N=1088) highlights its ability to separate outcomes, with a 32% vs 10% prostate cancer–specific mortality risk at 15 years, underscoring its prognostic utility.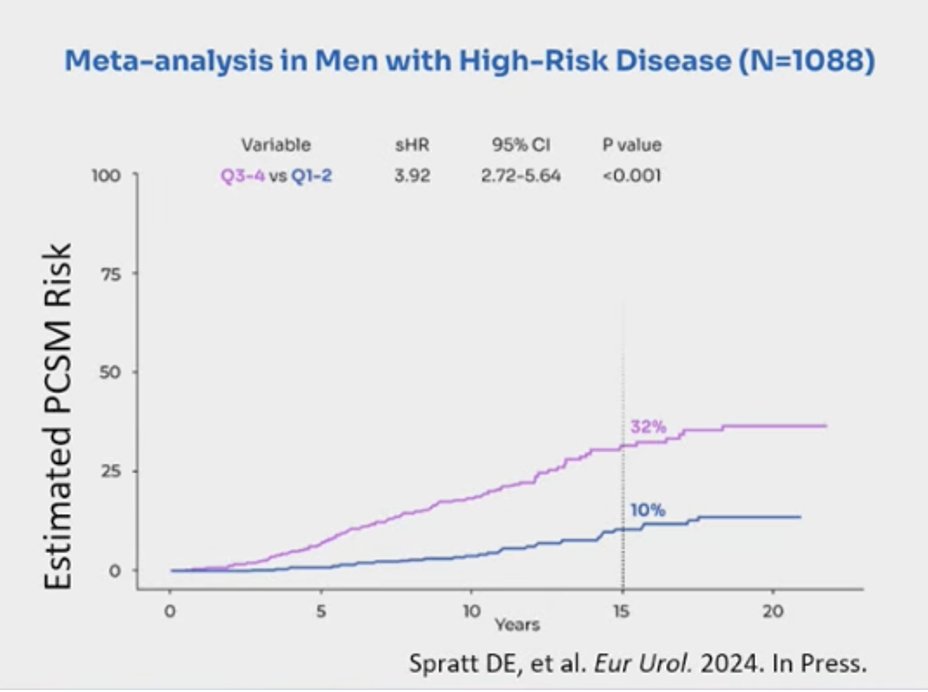
MMAI in the Oligometastic Prostate Cancer Setting
Dr. Sutera presented data evaluating MMAI in the oligometastatic CSPC setting, drawing on patients from the STOMP and ORIOLE trials. Among 222 men with ≤5 metastases, those with higher MMAI scores had significantly higher PSA levels at diagnosis and at the time of metastasis, were more likely to have Gleason Grade Group ≥4, and more often presented with synchronous or de novo disease compared to those with lower MMAI scores. These findings suggest that MMAI can discriminate biological risk in oligometastatic disease, potentially identifying patients with more aggressive disease biology.2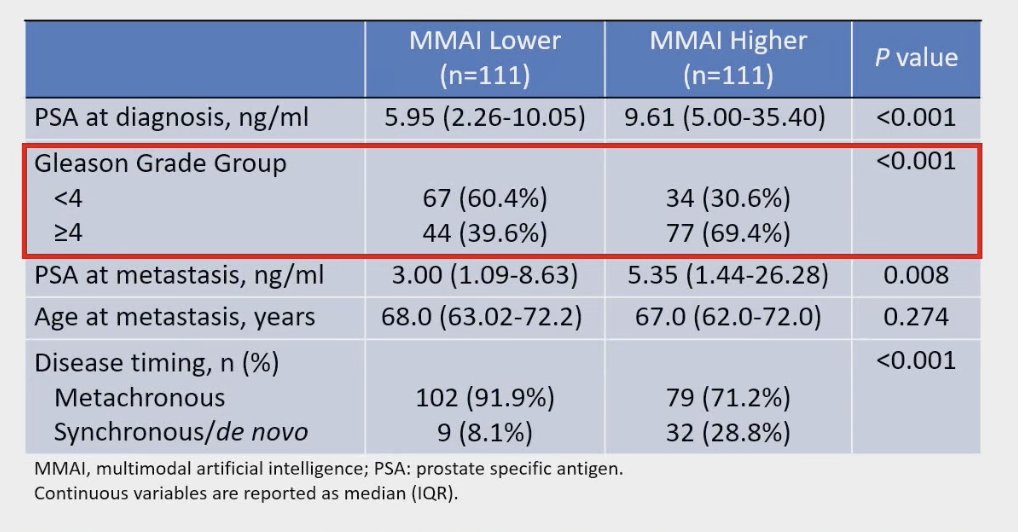
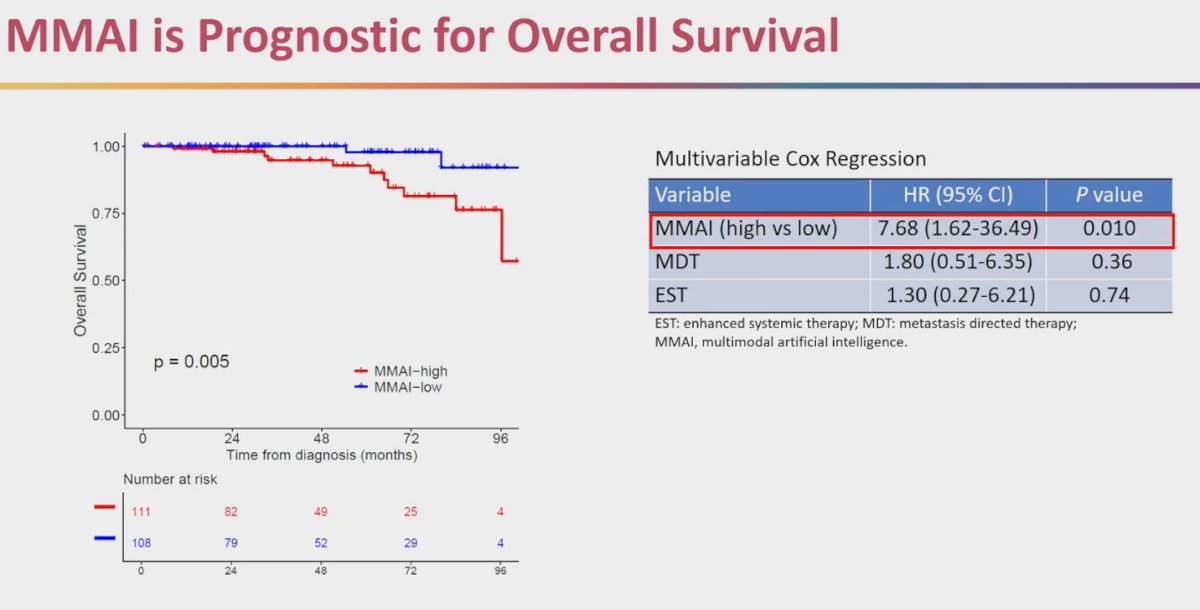
MMAI is also prognostic in the oligometastatic setting. In a multi-institutional retrospective analysis of patients from the STOMP and ORIOLE trials, those with higher MMAI scores had worse overall survival. Importantly, when adjusting for known covariates such as receipt of MDT or enhanced systemic therapy, MMAI remained independently prognostic, with a hazard ratio of 7.68. This reinforces the role of MMAI as a strong biomarker to stratify patients beyond traditional clinical features.2
Dr. Sutera highlighted that an elegant way to test whether MMAI predicts benefit from MDT was through subset analyses of patients enrolled on the STOMP and ORIOLE trials. (3) In these studies, patients were randomized to MDT versus observation, and the primary endpoint was metastasis-free survival (MFS). Importantly, predictive testing focused on whether the differential benefit of MDT on MFS varied according to MMAI score, stratified by the median. While overall survival was not assessed due to too few events.
The data demonstrated that patients with higher MMAI scores derived significant benefit from MDT, with markedly improved MFS compared to observation. In contrast, those with lower MMAI scores did not show the same level of differential benefit, suggesting that for these patients, MDT could potentially be deferred. This highlights MMAI’s potential role in identifying patients who require immediate MDT versus those in whom a delayed approach may be reasonable.3

Dr. Sutera emphasized the importance of opening the “black box” of MMAI. The first black box reflects the AI model interpreting pathology image patches, and the second integrates these image-derived features with clinical data to generate the final MMAI score. He noted three key reasons for looking inside: first, to provide clinicians confidence that the AI’s predictions are rooted in interpretable biology rather than “smoke and mirrors”; second, to reveal underappreciated aspects of prostate cancer biology and mechanisms of metastasis; and third, to satisfy a natural scientific curiosity in better understanding how these features drive outcomes.
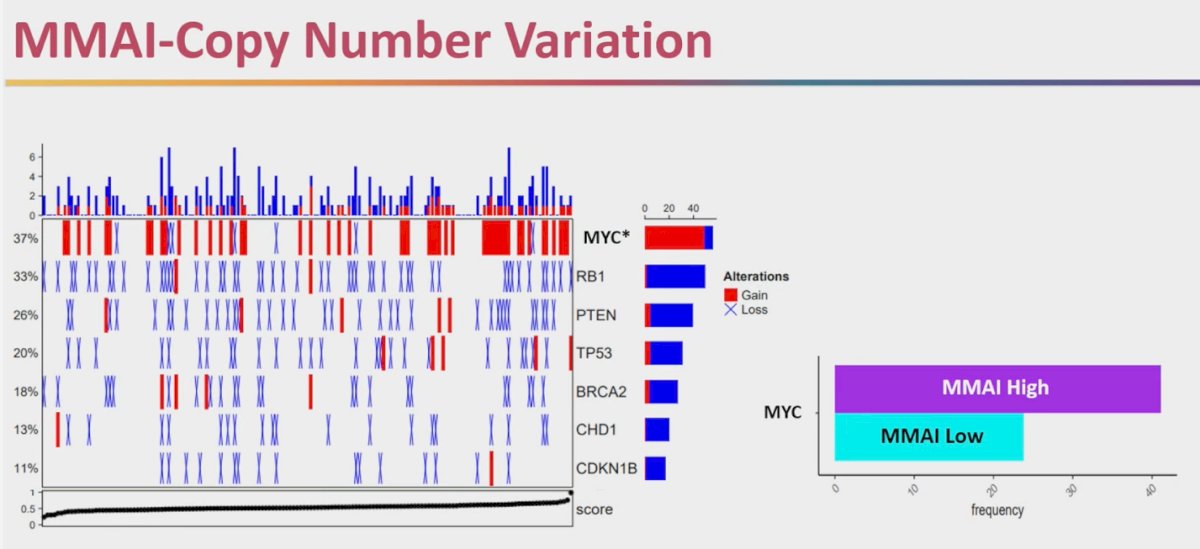
Dr. Sutera presented exploratory work examining the association between MMAI and genomics. In a cohort of 227 patients who underwent somatic DNA panel sequencing, pathogenic nonsynonymous mutations and copy number variants were identified and classified using established pipelines. The team then assessed whether higher MMAI scores correlated with an increased frequency of these alterations.
Dr. Sutera presented exploratory data linking MMAI scores with underlying genomic alterations in a cohort of 227 patients who underwent somatic DNA panel sequencing. Specifically, higher MMAI scores were significantly associated with MYC copy number gain, observed in 42% of patients, while other alterations such as RB1, PTEN, TP53, BRCA2, CHD1, and CDKN1B did not show a meaningful difference, as illustrated below. This finding suggests that MYC amplification may contribute to the aggressive biology captured by higher MMAI scores, reinforcing its potential role as a prognostic and biologically relevant biomarker
To peek inside the “image” black box, the team clustered slide patches from the self-supervised model and mapped them with UMAP. Several clusters aligned with recognizable histology—benign glands, smooth muscle/vessels, small, scattered tumor glands, and cribriform/Gleason pattern 4—while a large gray region reflected image features pathologists can’t yet label, hinting at novel or composite signals. Shapley analysis showed the MMAI score is driven predominantly by image features (~64%), with smaller contributions from T stage (~22%), PSA (~11%), and age (~3%). Net: MMAI’s prognostic power comes mainly from morphology the network extracts; some of it matches what we already recognize, and some of it may represent underappreciated biology worth interrogating.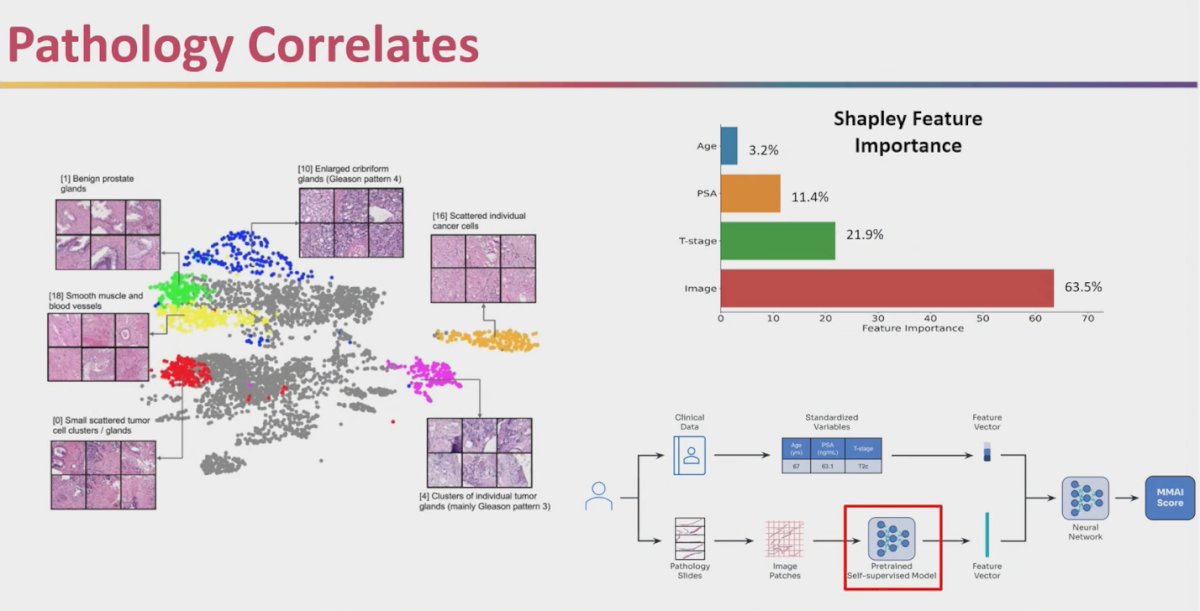
Dr. Sutera emphasized that the AI-driven MMAI model is not pinpointing isolated foci of aggressive disease but is instead focusing on the tumor as a whole. As illustrated in the heat maps, areas of highest attention are concentrated within the malignant tissue, while benign glands and stromal components are largely ignored. This suggests that the AI is capturing biologically relevant features of the tumor itself, rather than being misled by surrounding non-malignant structures.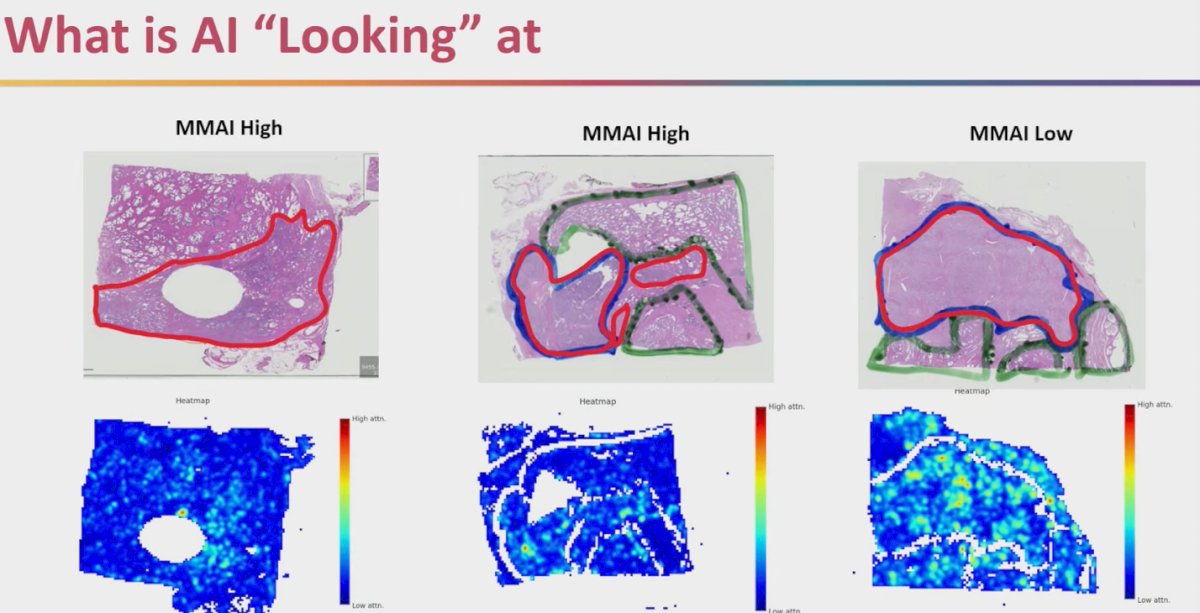
Dr. Sutera went on to describe efforts using spatial transcriptomics to overlay H&E pathology with gene expression data. This approach helps evaluate “hotspots” of AI attention and interrogates what biological features may be driving the MMAI signal. By combining U-map clustering with transcriptomic overlays, investigators can begin to understand not just where AI is focusing within tumors, but also what genomic programs might underlie these regions of interest. This adds a biologic rationale to the MMAI score and moves closer toward deciphering the black box of AI-driven pathology.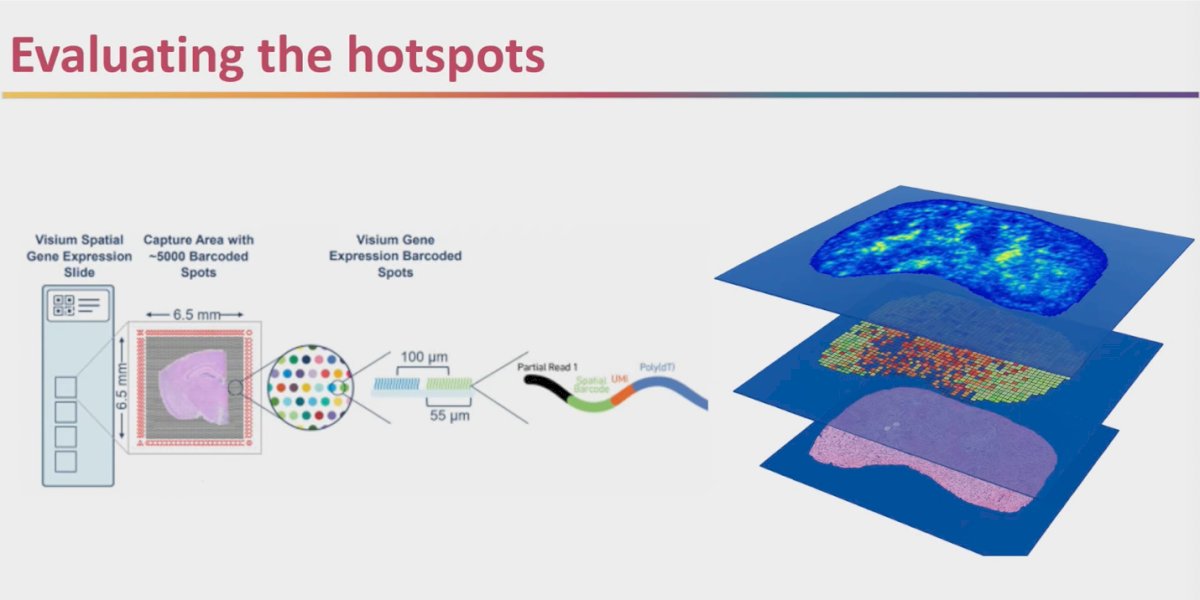
Lastly, building on the earlier DNA findings, Dr. Sutera showed that AI attention maps also revealed overexpression of MYC targets, nicely complementing the copy number gain data previously presented. This consistency between DNA alterations and transcriptional output supports the biological rationale for MMAI, reinforcing that the model is capturing relevant oncogenic pathways rather than noise.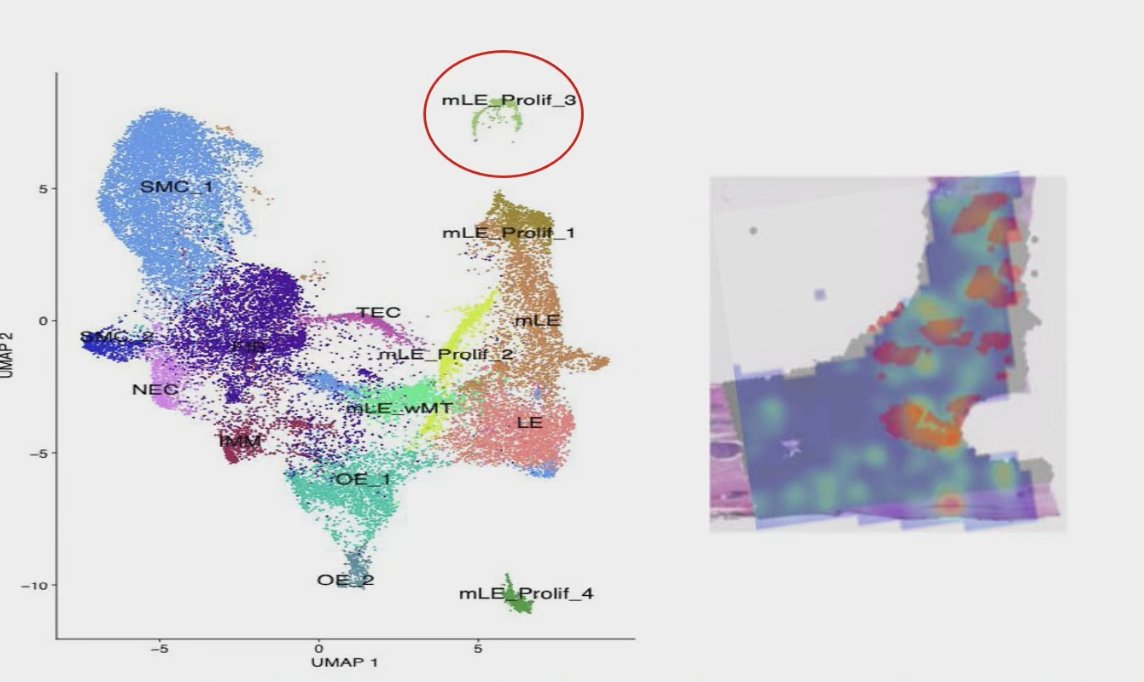
Dr. Sutera concluded his presentation by outlining future directions for MMAI research. He emphasized the need to validate MMAI as a prognostic marker in larger prospective cohorts, explore whether MMAI can predict which patients benefit from MDT with or without ADT, and continue efforts to open the “black box” of AI to better understand the biological underpinnings of its predictions.
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Cancer Treatment and Research Center (CTIC), Luis Carlos Sarmiento Angulo Foundation via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco between the 28th of September and the 30th of September.
References:
- Spratt DE, Liu VYT, Jia AY, Royce TJ, Sandler HM, Pugh SL, Tran PT, Feng FY. Meta-analysis of Individual Patient-level Data for a Multimodal Artificial Intelligence Biomarker in High-risk Prostate Cancer: Results from Six NRG/RTOG Phase 3 Randomized Trials. Eur Urol. 2024 Oct;86(4):369-371. doi: 10.1016/j.eururo.2024.06.019. Epub 2024 Jul 17. PMID: 39025748; PMCID: PMC11480946.
- Markowski MC, Ren Y, Tierney M, Royce TJ, Yamashita R, Croucher D, Huang HC, Todorovic T, Chen E, Showalter TN, Carducci MA, Chen YH, Liu G, Parker CTA, Esteva A, Feng FY, Attard G, Sweeney CJ. Digital Pathology-based Artificial Intelligence Biomarker Validation in Metastatic Prostate Cancer. Eur Urol Oncol. 2025 Jun;8(3):755-762. doi: 10.1016/j.euo.2024.11.009. Epub 2024 Dec 10. PMID: 39665917; PMCID: PMC12369405.
- Wang JH, Deek MP, Mendes AA, Song Y, Shetty A, Bazyar S, Van der Eecken K, Chen E, Showalter TN, Royce TJ, Todorovic T, Huang HC, Houck SA, Yamashita R, Kiess AP, Song DY, Lotan T, DeWeese T, Marchionni L, Ren L, Sawant A, Simone N, Berlin A, Onal C, Esteva A, Feng FY, Tran PT, Sutera P, Ost P. Validation of an artificial intelligence-based prognostic biomarker in patients with oligometastatic Castration-Sensitive prostate cancer. Radiother Oncol. 2025 Jan;202:110618. doi: 10.1016/j.radonc.2024.110618. Epub 2024 Nov 6. PMID: 39510141; PMCID: PMC11663099.