(UroToday.com) The 2025 ASTRO annual meeting featured a plenary session and a presentation by Dr. Rodney Ellis discussing the co-primary results from NRG-GU005, an international phase III trial of SBRT versus hypofractionated IMRT for localized intermediate risk prostate cancer. Intermediate risk prostate cancer has multiple accepted radiotherapy fractionation strategies, including stereotactic body radiation, which is guideline endorsed and phase III comparative data has been emerging. This randomized non-blinded phase III trial compared stereotactic body radiation therapy to moderately hypofractionated IMRT in localized intermediate risk prostate cancer patients and was designed for superiority of disease free survival and patient reported health related quality of life.
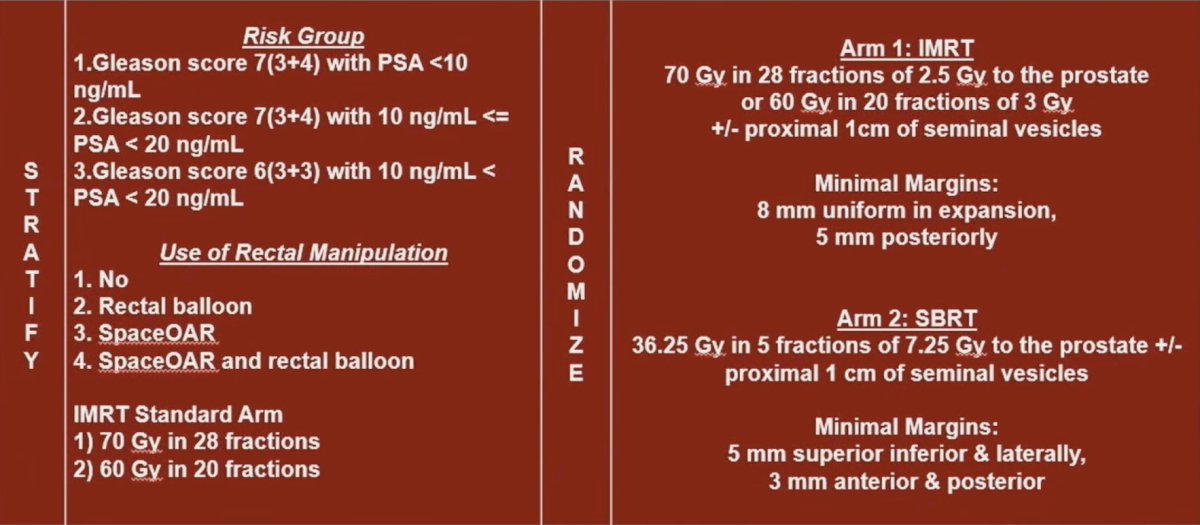
The NRG-GU005 trial enrolled patients with intermediate-risk prostate cancer and randomized 1:1 to receive stereotactic body radiation therapy (36.25 Gy in 5 fractions) or IMRT (70 Gy in 28 fractions or 60 Gy in 20 fractions):
NRG-GU005 had co-primary endpoints:
- To determine if stereotactic body radiation is superior to hypofractionated IMRT: in terms of patient reported gastrointestinal and genitourinary toxicity, as measured by EPIC-26 bowel and urinary irritation domains, respectively, at 24 months post completion of therapy, by minimal clinically important difference in EPIC-26
- To determine if stereotactic body radiation is superior to hypofractionated IMRT for disease free survival: this was defined as time to biochemical failure (Phoenix definition), local failure, regional failure, distant metastasis, or death from any cause
The health related quality of life co-primary endpoint was designed to show 10% and 8% absolute reductions in the frequency of a minimal clinically important decline in bowel and urinary irritation/obstruction domains, respectively, at 24 months. The disease free survival endpoint, was designed to detect a 38% relative improvement with stereotactic body radiation therapy. Both endpoints had interim futility analyses.
In terms of radiotherapy details, CTV included the prostate +/- 1 cm of the proximal seminal vesicles (at the discretion of the treating physician). Moderate hypofractionated IMRT included 70 Gy in 28 fractions or 60 Gy in 20 fractions, with a CTV to PTV expansion of 8 mm in all directions except posteriorly, where 5 mm was allowed. Stereotactic body radiation was 36.25 Gy in 5 fractions of 7.25 Gy, delivered at 2-3 fractions per week. CTV to PTV expansion was 5 mm radially and 3 mm both posteriorly and anteriorly. The maximum dose to PTV was 38.8 Gy, and the maximum dose to 0.03 cc and 50% of the bladder was 39 Gy and 15 Gy, respectively. The use of fiducial markers and MRI fusion for planning, as well as daily advanced IGRT, were mandated.
The sample size calculation details included a 2 sided type I error = 0.05 for health related quality of life at 24 months, with one interim futility analysis. For the EPIC bowel domain, this included a 10% absolute reduction in the percentage of minimal clinically important difference (>= 4) for 80% power. For the EPIC urinary irritation/obstruction domain, this included an 8% absolute reduction in the percentage of minimal clinically important difference (>= 5) for 83% power. This resulted in 466 evaluable patients. For disease free survival, assuming a hazard ratio of 0.62, 15 patients per month, a 2-sided type I error of 0.05, and one interim futility analysis, this resulted in 89% power and 178 events from 590 evaluable patients. The target accrual was 691 patients, assuming 25% inflation for non compliance, and 10% inflation for death/consent withdrawal.
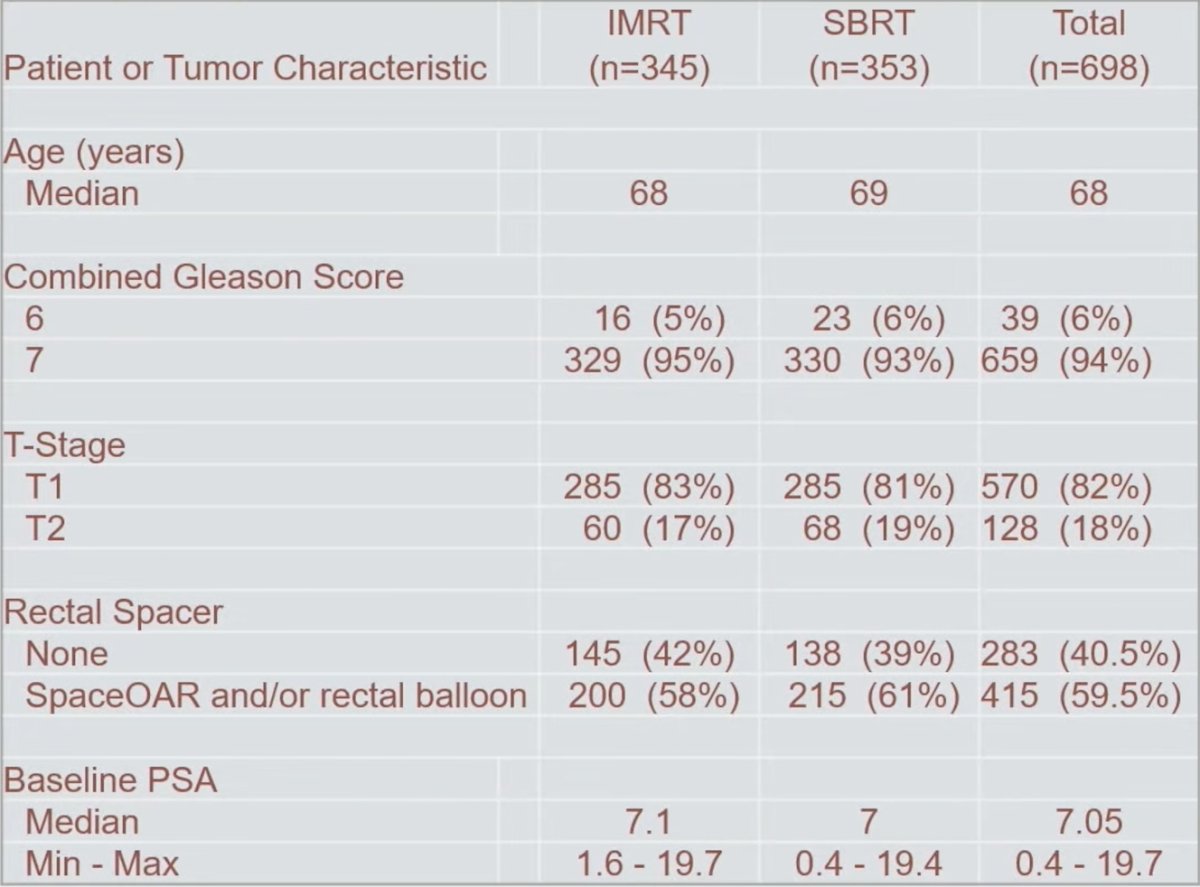
Overall, there were 698 patients randomized, with 353 in the stereotactic body radiation therapy arm and 345 in the IMRT arm. The baseline characteristics were well balanced across arms, with no significant differences in baseline health related quality of life:
At 2 years post-treatment, 82.5% of moderately hypofractionated IMRT and 85.1% stereotactic body radiation therapy patients completed the EPIC-26. Of those, 97.5% and 96.2% had scoreable bowel and urinary irritation/obstruction domains.
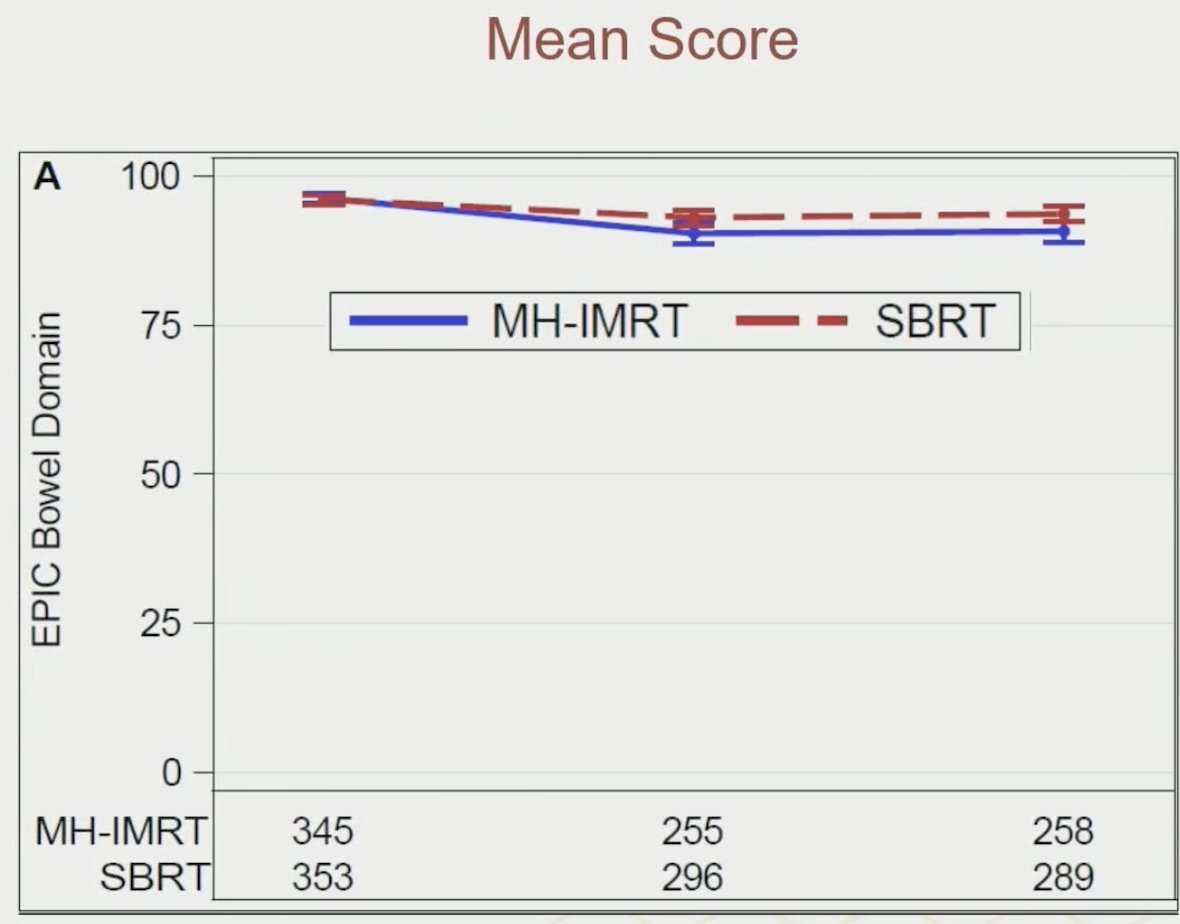
There were significantly fewer patients in the stereotactic body radiation therapy arm who experienced a 2-year minimal clinically important decline in bowel health related quality of life (35% versus 44%, p = 0.034). The analysis of the longitudinal bowel domain scores showed a significant treatment effect in favor of stereotactic body radiation therapy (least square mean = 2.68, 95% CI: 1.02, 4.34; p = 0.0016):
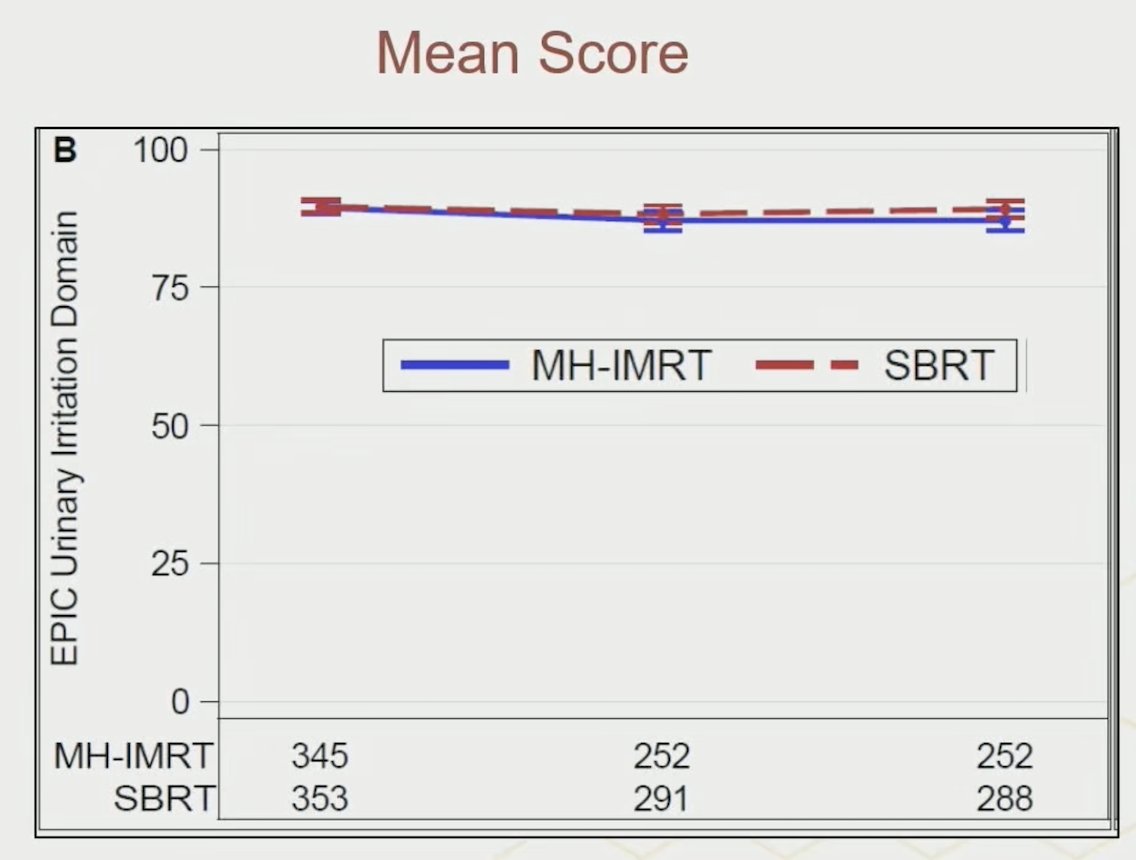
Minimal clinically important decline frequency for the urinary irritation/obstruction domain was not significantly different between stereotactic body radiation therapy and IMRT (35% versus 34%, p = 0.68):
Secondary EPIC favorable stereotactic body radiation therapy outcomes included sexual domain at 1 year (p = 0.03) and urinary incontinence at 2 years (p = 0.02). Longitudinal analysis also favored stereotactic body radiation therapy over moderately hypofractionated IMRT in terms of patient reported urinary incontinence related quality of life. The futility bound for disease free survival was crossed in the interim analysis (HR 1.38, 95% CI 0.91-2.09, p = 0.13), indicating lack of superiority for stereotactic body radiation therapy over hypofractionated IMRT (5-year rates of 89%, 95% CI 85%-92% for stereotactic body radiation therapy versus 92%, 95% CI 89%-95% for IMRT):
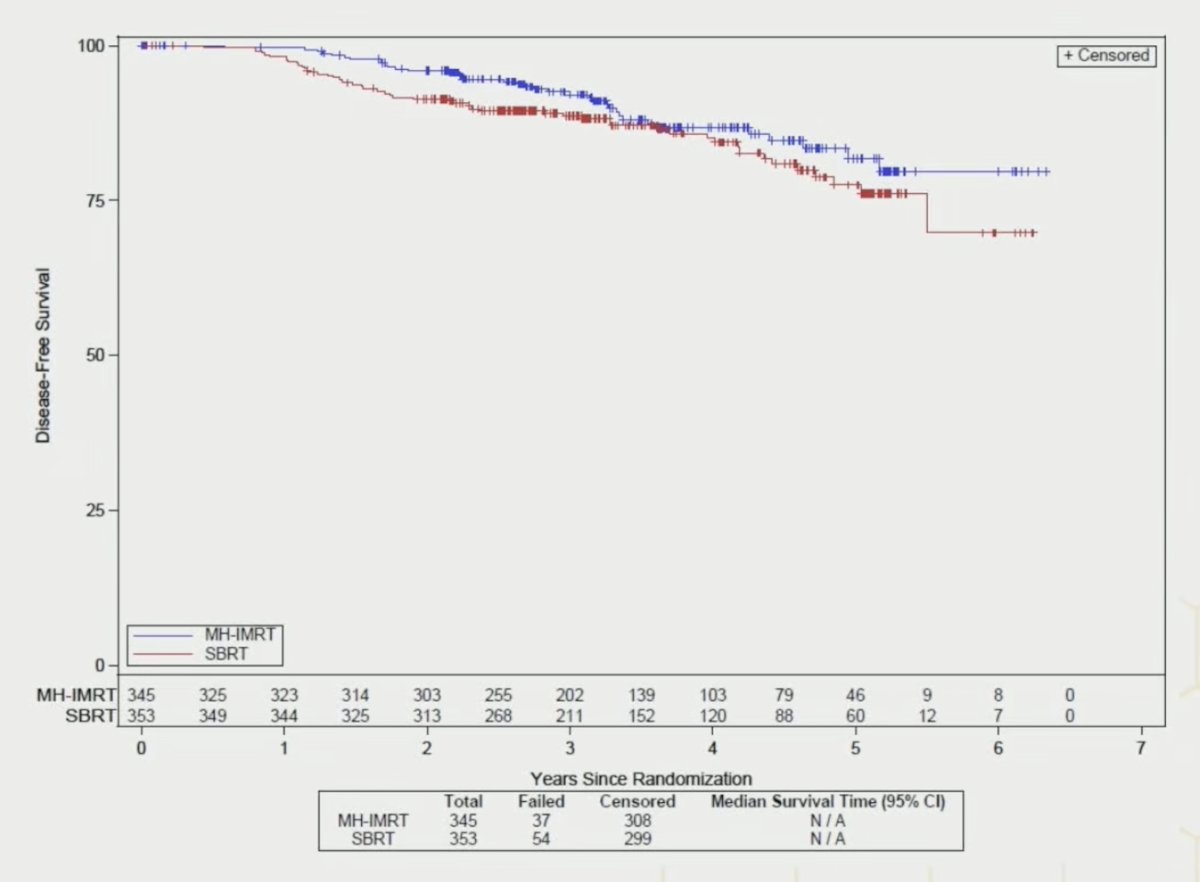
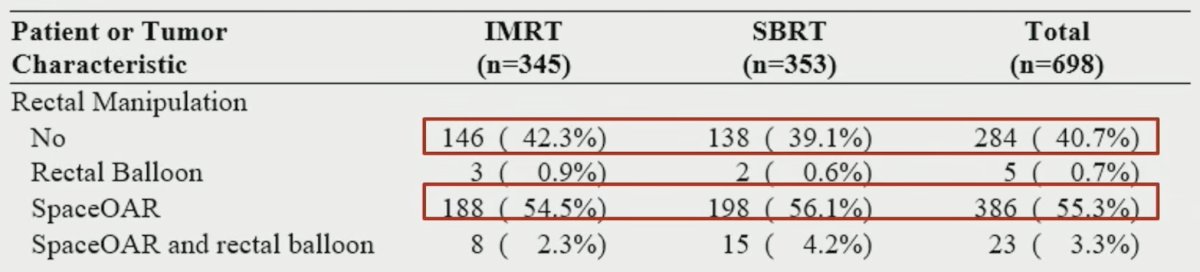
Minimal local or distant failures were reported; however, cumulative instance of biochemical failure were lower at 3 years in IMRT as compared to stereotactic body radiation therapy (4%, 95% CI 2.3-7.0 versus 8%, 95% CI 5.2-11.0, p = 0.037). Overall survival at 5 years showed no difference (p = 0.66) between stereotactic body radiation therapy (91%, 95% CI 85%-95%) and IMRT (94%, 95% CI 90%-97%). Using a rectal spacer occurred in 56% stereotactic body radiation therapy versus 55% IMRT subjects and resulted further in superior EPIC bowel domain scores (least square mean = -2.81, 95% CI: -4.49, -1.13; p = 0.0011):
Dr. Ellis concluded his presentation discussing the primary results from NRG-GU005 with the following take home points:
- Bowel health related quality of life was significantly better with stereotactic body radiation therapy
- There was no difference between arm in primary urinary irritative/obstructive health related quality of life
- EPIC urinary incontinence domain favor stereotactic body radiation therapy at 2 years (p = 0.02)
- EPIC sexual domain favors stereotactic body radiation therapy at 1 year (p = 0.03
- There was no disease free survival superiority of stereotactic body radiation therapy
Presented by: Rodney Ellis, MD, University South Florida and Tampa General Hospital Cancer Institute, Tampa, FL
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, Sat, Sept 27 – Wed, Oct 1, 2025.