(UroToday.com) The 2025 ASTRO annual meeting featured a prostate cancer session and a presentation by Dr. Wee Loon Ong discussing the kinetics of testosterone recovery after androgen deprivation therapy (ADT). Dr. Ong started his presentation by noting that the story of androgen suppression and prostate cancer dates back to the 1940s with the Nobel prize winning work spearheaded by Charles Huggins and Clarence Hodges. However, there are many side effects of ADT, including:
- Loss of bone mineral density
- Fracture risk
- Diabetes
- Cardiovascular disease
- Depression
- Hot flashes
- Gynecomastia
- Myocardial infarction
- Stroke
- Alzheimer’s disease
Dr. Ong notes that the first aim for assessing testosterone recovery after ADT is to quantify the time to testosterone recovery and identify factors associated with testosterone recovery. There are several important questions/considerations:
- When we prescribe ADT for X months, we are shutting down testosterone production for at least X months
- However, it takes time for testosterone recovery after the X months of ADT
- How do we counsel patients on the likelihood of testosterone recovery and the time to testosterone recovery following ADT?
- Are there factors that affect testosterone recovery?
The TRANSPORT meta-analysis1 included individual patient data from 5 randomized controlled trials of radiotherapy with ADT and prospectively collected serial testosterone data from the MARCAP Consortium:

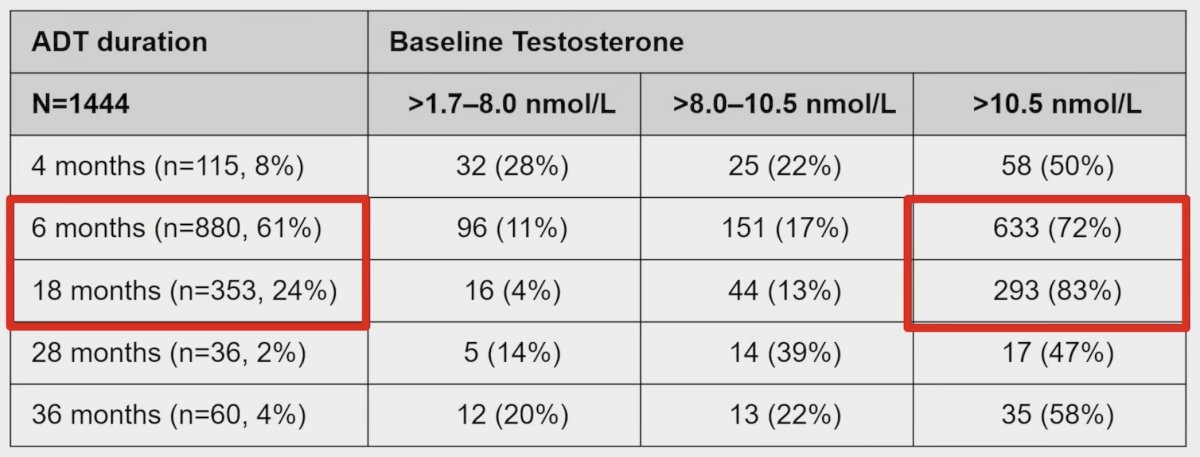
Dr. Ong and colleagues estimated the times to non-castrate testosterone recovery (>1.7 nmol/l) and non-hypogonadal testosterone recovery (>8.0 nmol/l) for each prescribed ADT duration. The time to testosterone recovery was the end date of prescribed ADT until the date of testosterone recovery. Patients were excluded if they had no baseline testosterone, baseline testosterone >30 days after initiation of ADT, and patients that did not receive the prescribed duration of ADT. This analysis included 1,444 men, of whom 115 received 4 months, 880 received 6 months, 353 received 18 months, 36 received 28 months, and 60 received 36 months of ADT:
Time to non-castrate testosterone recovery varied considerably by ADT duration:
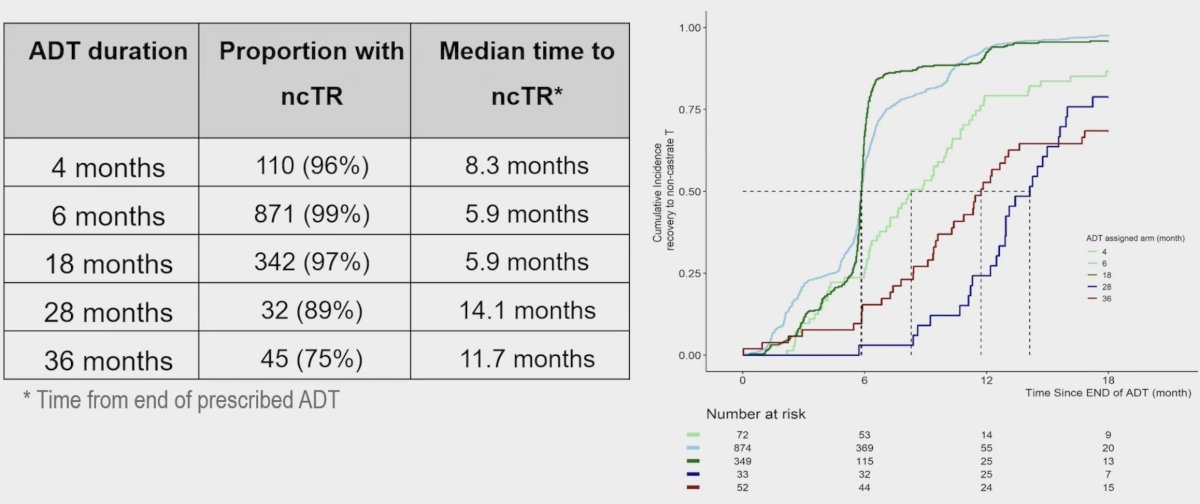
Similarly, time to non-hypogonadal testosterone recovery varied considerably by ADT duration:

Higher baseline testosterone and lower age were associated with a higher likelihood of testosterone recovery (p < 0.001 for both). These results culminated in a non-castrate testosterone and a non-hypogonadal testosterone recovery nomogram:
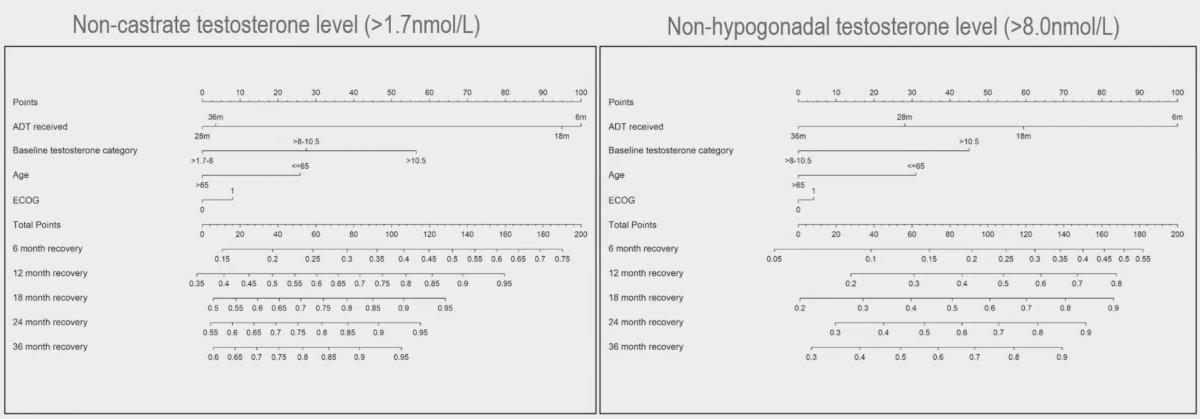
To illustrate the utilization of these nomograms, Dr. Ong noted two examples. The first was of a 70 year old man, ECOG 0, baseline testosterone 9.0 nmol/L, who received 6 months of ADT. Based on the nomogram, non-hypogonadal testosterone recovery is:
- ~23% at 6 months
- ~45% at 12 months
- ~60% at 18 months
The second was of a 60 year old man, ECOG 0, baseline testosterone 15.0 nmol/L, who received 6 months of ADT. Based on the nomogram, non-hypogonadal testosterone recovery is:
- 50% at 6 months
- >80% at 12 months
- >90% at 18 months
Dr. Ong notes that the second aim for assessing testosterone recover after ADT is to evaluate the association between effective castration period and metastases free survival. There are several important questions/considerations:
- Does the duration of ‘effective castration’ influence the outcomes?
- Prescribed ADT duration = the intended duration of castration
- But non-castrate testosterone recovery rates vary
- So, are there differential oncological outcomes depending on the effective castration duration?
- LHRH antagonist is associated with a more rapid testosterone recovery profile
- Is 6 months of LHRH agonist + radiotherapy equal to 6 months of LHRH antagonist + radiotherapy in terms of oncological outcomes?
Dr. Ma notes that effective castration period was not linearly associated with metastasis free survvial for any ADT duration on Cox regression. Cubic spline analysis revealed that the optimal effective castration period for an metastasis free survival benefit was 10.6 months for men who received 6 months of ADT and 18 months for men who received 18 months of ADT.
Dr. Ong concluded his presentation discussing the kinetics of testosterone recovery after ADT with the following take home points:
- The TRANSPORT individual patient data meta-analyses provide the highest level of prospective data on time to testosterone recovery by the prescribed ADT duration
- Older age, lower baseline testosterone, and longer ADT duration are associated with longer time to testosterone recovery
- A nomogram was developed to estimate the probability of testosterone recovery
- There may be a non-linear association between effective castration periods and metastasis free survival
- For short term ADT (ie. 6 months of ADT), a longer effective castration period (~11 months) may be associated with better oncological outcomes
- This may have implications in clinical decision making when using LHRH antagonists (with a more rapid testosterone recovery profile)
Presented by: Wee Loon Ong, Alfred Health Radiation Oncology, Melbourne, Australia
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, September 28th – 30th, 2025
References: