(UroToday.com) The 2025 ASTRO annual meeting featured a clinical trials session and a presentation by Dr. Daniel Spratt discussing the BALANCE NRG GU006 trial assessing apalutamide and radiotherapy for recurrent prostate cancer. Radical prostatectomy is a treatment option for appropriately selected men with localized prostate cancer; however, recurrence rates after radical prostatectomy for men with intermediate and high-risk prostate cancer range from 40-80% in clinical trials. Use of early secondary (previously termed salvage) radiotherapy is generally preferred over adjuvant radiotherapy for most men.
Currently, there are no prospectively validated predictive biomarkers to guide the use of hormonal therapy in prostate cancer. Moreover, hormone therapy in unselected men receiving early salvage radiotherapy does not improve overall survival. This was recently emphasized in the DADSPORT meta-analysis, showing that for a PSA <= 0.3 ng/mL the overall survival HR was 0.97, and for a PSA >0.3 – 0.5 ng/mL the overall survival HR was 1.07.1 In 2015, Dr. Spratt and colleagues developed a novel, luminal-basal classification adapted from breast cancer: the PAM50 signature. Zhao et al.2 applied the classifier to 3,782 samples (1,567 retrospective, 2,215 prospective), noting that the PAM50 classifier consistently segregated prostate cancer into three subtypes in both retrospective and prospective cohorts:
- Luminal A (retrospective 34.3%; prospective 33.3%)
- Luminal B (retrospective 28.5%; prospective 32.6%)
- Basal (retrospective 37.1%; prospective 34.1%)
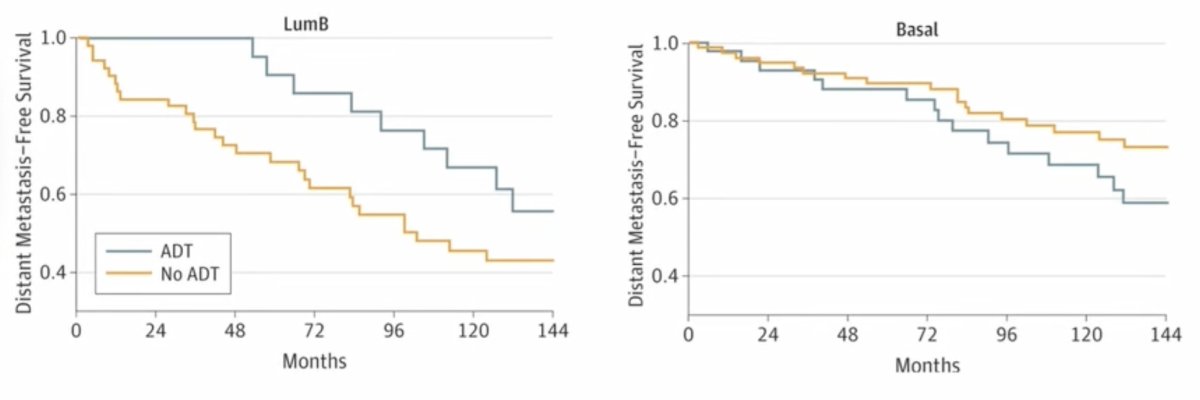
When assessing luminal B and basal tumors with regard to response to ADT, this study suggests there may be a benefit to the treatment of luminal B patients with ADT, but no benefit is seen in those with basal tumors:
NRG GU006, a phase II biomarker-stratified randomized trial of patients receiving salvage radiotherapy with or without apalutamide, was designed with the hypothesis that transcriptionally defined molecular subtypes would differentially benefit from apalutamide. Patients were enrolled between April 2018 – February 2020 and were required to be post-radical prostatectomy with a PSA 0.1-1.0 ng/mL without evidence of nodal or distant metastasis and randomized to salvage radiotherapy with placebo or apalutamide 240 mg daily for 6 months. Patients were stratified by PAM50 molecular subtype (luminal B versus non-luminal B):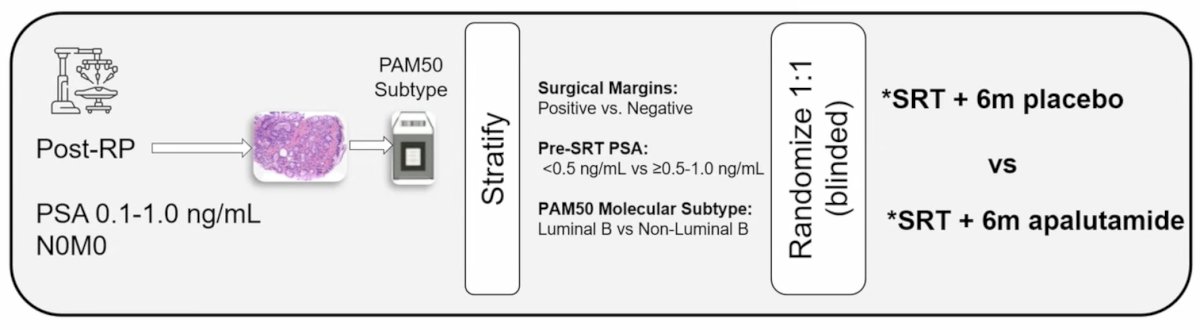
The primary endpoint was biochemical progression-free survival, defined as the first occurrence of biochemical, local, regional, distant recurrence, or death from any cause. Key secondary endpoints reported are metastasis-free survival, distant metastasis, salvage hormone therapy use, and toxicity. The design and analysis involved first testing efficacy within the luminal B subtype (hypothesized to show greater benefit), followed by evaluation of the non-luminal-B group. If the lower limit of the 80% confidence interval for the hazard ratio (HR [apalutamide/placebo]) in the latter group was > 0.77, lack of efficacy in this subgroup would be declared.
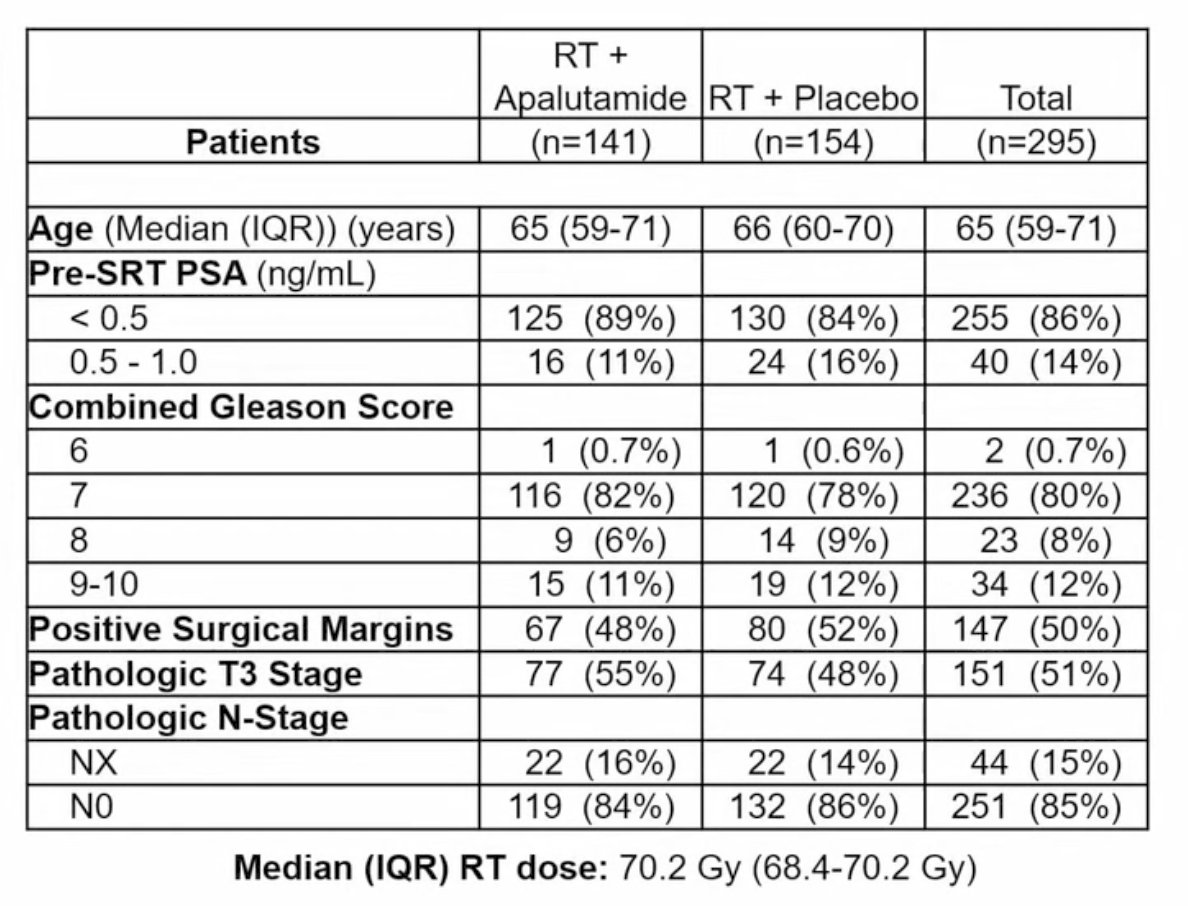
A total of 295 eligible patients were enrolled with a median follow-up of 5.0 years. The arms were well balanced, with a median age of 65 years (IQR 59-71), 50% with positive surgical margins, 51% with pathologic T3 disease, and 86% with entry PSA of <0.5 ng/mL. There were 20% of patients with grade group 4-5 prostate cancer:
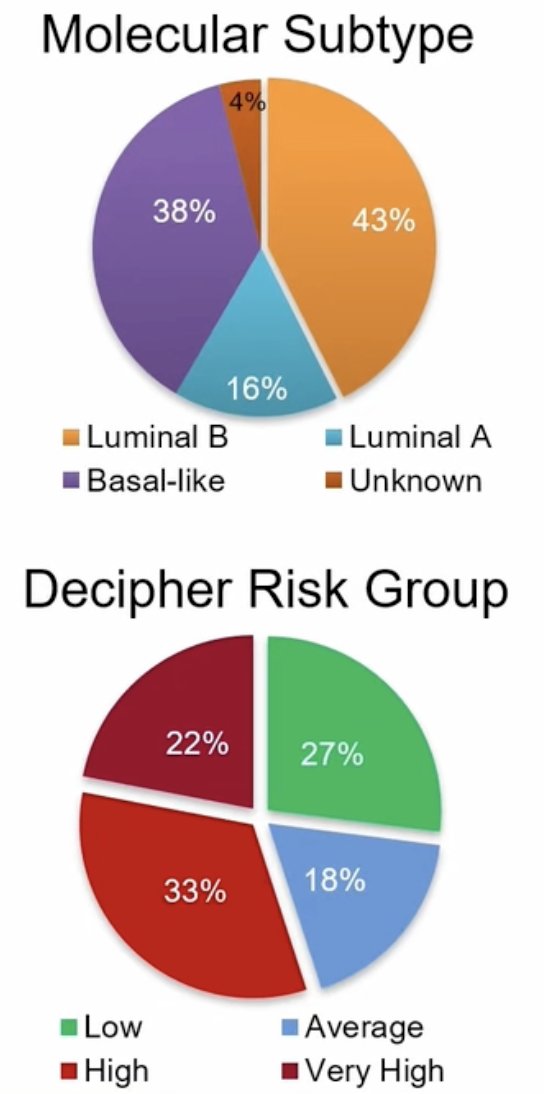
Overall, 43% of patients were luminal B and 33% of patients had Decipher high risk score:
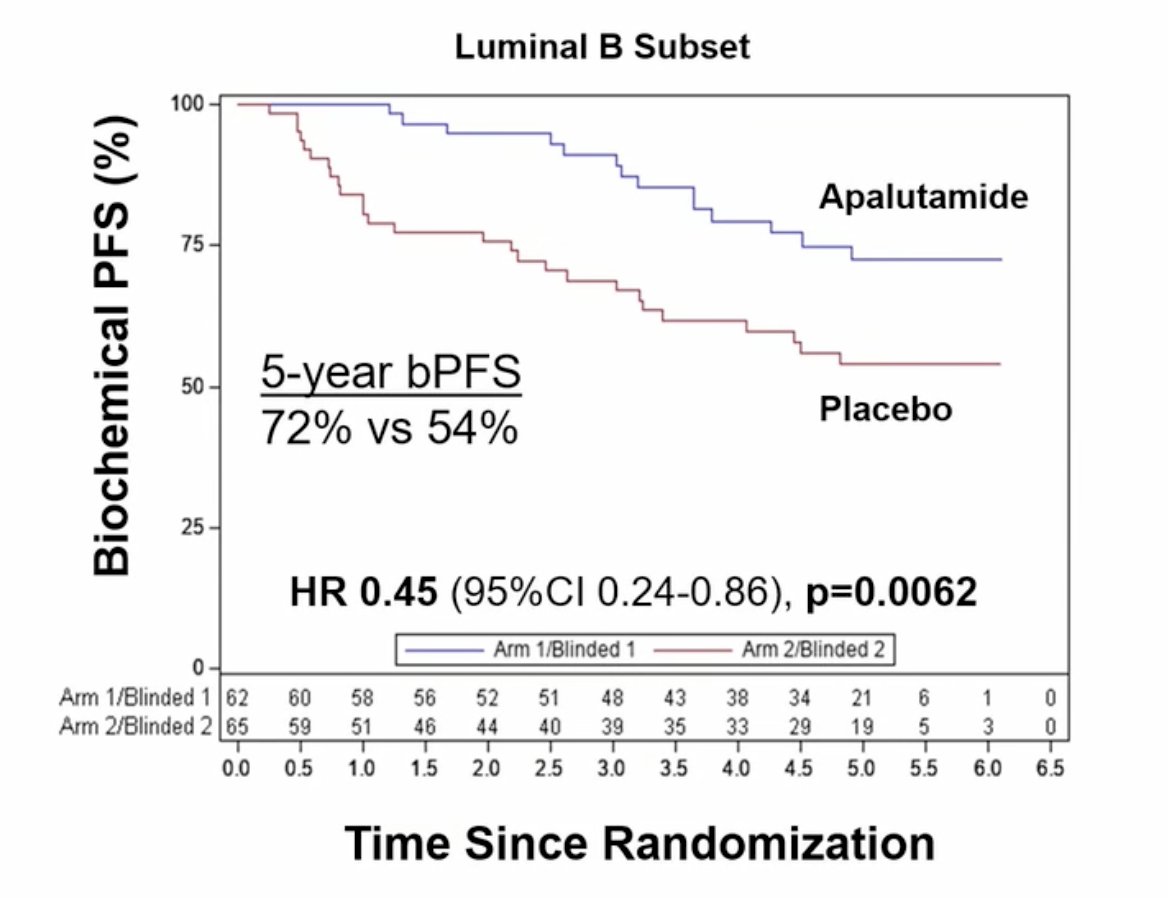
In luminal B patients, apalutamide significantly improved biochemical progression-free survival (HR 0.45, 80% CI 0.29-0.68, one-sided p = 0.0062), with 5-year estimated biochemical progression-free survival of 72% versus 54% in the apalutamide and placebo arms, respectively:
In contrast, non-luminal B patients did not demonstrate improvement in biochemical progression-free survival (HR 0.95, 80% CI 0.65-1.41, p = 0.44), with 5-year estimated biochemical progression-free survival of 70% versus 71%, although the lower CI limit was <0.77: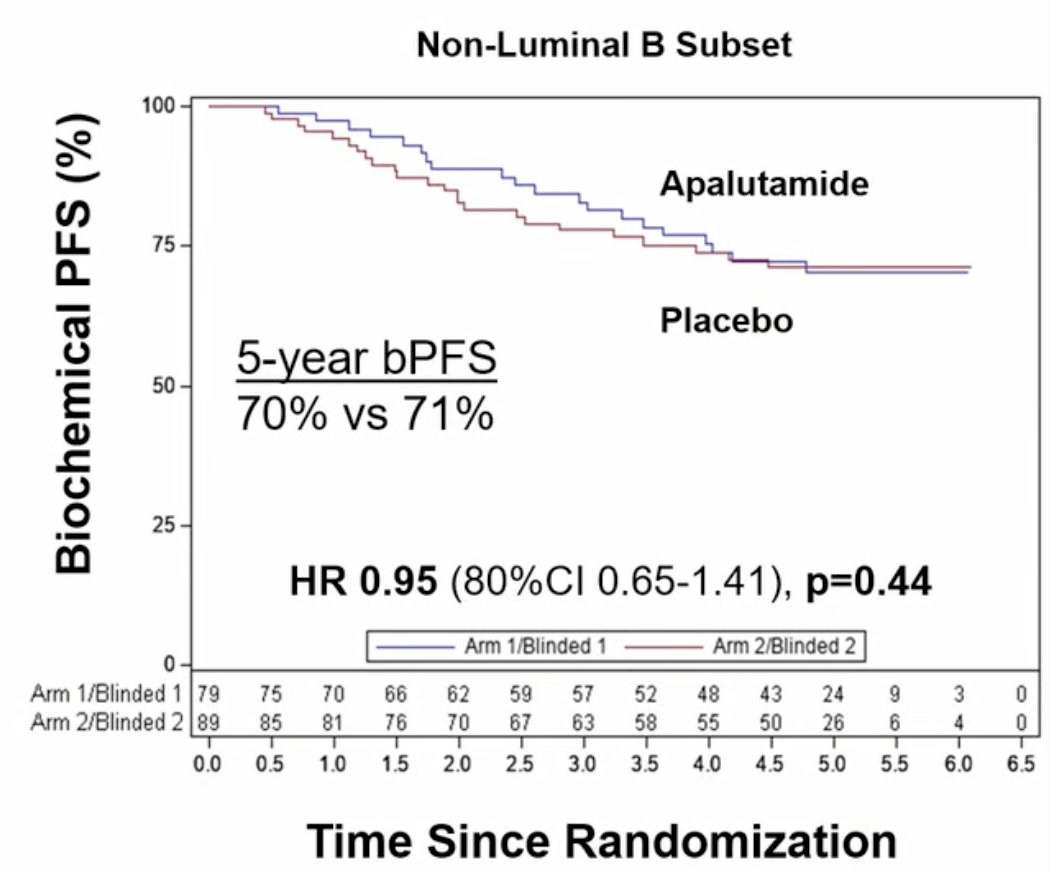
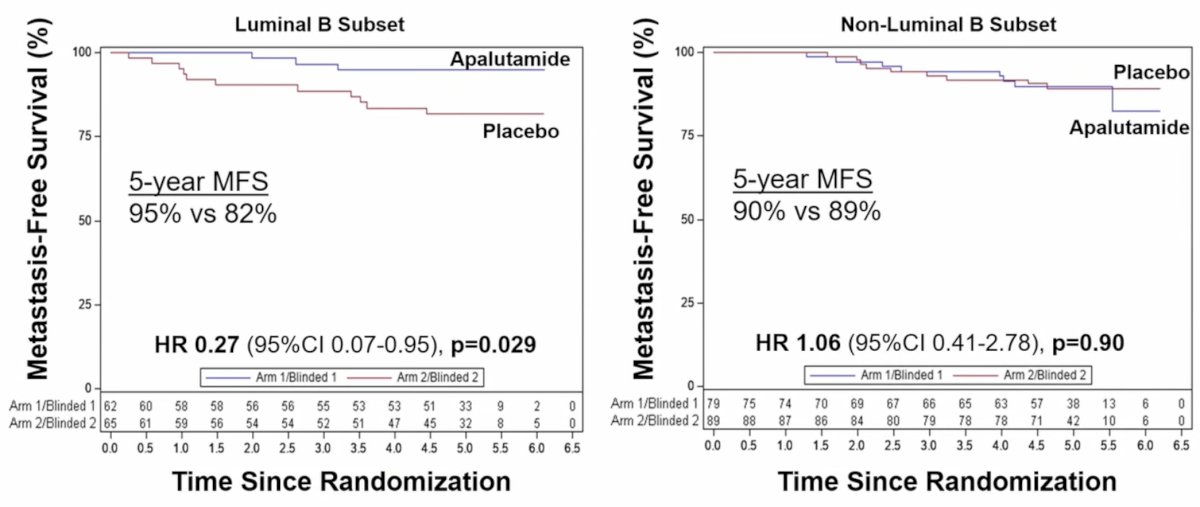
Metastasis-free survival was also improved with apalutamide in luminal B patients (HR 0.27, 95% CI 0.07-0.95, p = 0.029; 5-year estimates of 95% versus 82%), but not in non-luminal B patients (HR 1.06, 95% CI 0.41-2.78, p=0.90; 5-year estimates of 90% versus 89%):
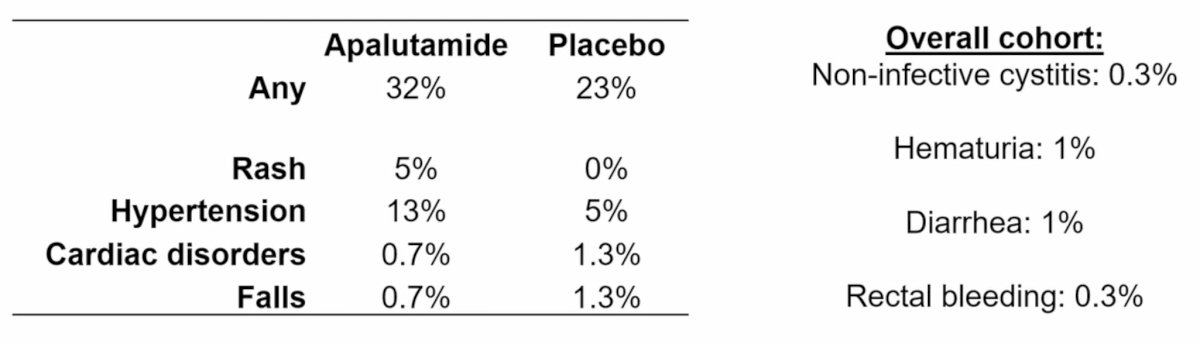
The all-cause mortality rate in the apalutamide arm was 4% versus 5% in the placebo group. In the apalutamide versus placebo arm (regardless of attribution), grade 3+ gastrointestinal toxicity occurred in 5.7% versus 2.6%, and genitourinary toxicity in 3.5% versus 4.5%, respectively. In the apalutamide arm, grade 3+ rash occurred in 5% of patients and breast pain in 0.7%:
Dr. Spratt concluded his presentation discussing the BALANCE NRG GU006 trial with the following take-home points:
- PAM50 represents the first and only prospectively validated predictive biomarker to guide the use of hormone therapy (Simon level 1A evidence)
- This trial demonstrates that patients with luminal B tumors derive clinically meaningful benefits, including in metastasis-free survival, from the addition of apalutamide to salvage radiotherapy
- These benefits were not observed in patients with non-luminal B tumors, with hazard ratios ~1.0, but a small potential benefit in this subgroup cannot be ruled out
- 6 months of apalutamide with salvage radiotherapy was well tolerated and is an effective treatment for patients with recurrent prostate cancer post radical prostatectomy
Presented by: Daniel Spratt, MD, Chair and Professor of Radiation Oncology, UH Cleveland Medical Center, Seidman Cancer Center, Case Western Reserve University School of Medicine, Cleveland, OH
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, Sat, Sept 27 – Wed, Oct 1, 2025.
Related content: NRG-GU006 Trial for Post-Prostatectomy Radiation Therapy - Daniel Spratt
References:
- Burdett S, Fisher DJ, Tierney JF, et al. Duration of Androgen Suppression with Postoperative Radiotherapy (DADSPORT) for Nonmetastatic Prostate Cancer: A Collaborative Systematic Review and Meta-analysis of Aggregate Data. Eur Urol. 2025 Sep;88(3):277-290.
- Zhao SG, Chang SL, Erho N, et al. Associations of Luminal and Basal Subtyping of Prostate Cancer with Prognosis and Response to Androgen Deprivation Therapy. JAMA Oncol. 2017 Dec 1;3(12):1663-1672.