(UroToday.com) The 2025 ESMO annual meeting featured a kidney cancer mini oral session and a presentation by Dr. Kathryn Beckermann discussing results from a phase 1b/2 trial of ipilimumab, nivolumab, and ciforadenant (an adenosine A2a receptor antagonist) in first-line advanced renal cell carcinoma (RCC).
Ciforadenant is an oral small molecule that selectively and reversibly binds adenosine-2A receptors on immune cells, reversing adenosine-mediated immunosuppression. Higher expression of A2AR in 60 patients with met RCC was associated with worse overall survival when treated with PD1/CTLA4 inhibitors. Dr. Beckermann and colleagues hypothesized that the addition of an adenosine-2A receptor antagonist, ciforadenant, to the combination of ipilimumab and nivolumab would favorably modulate metabolic adenosine signaling and the myeloid compartment to enhance clinical outcomes.
Eligibility criteria for this trial include untreated advanced clear cell RCC, ECOG performance status 0 or 1, and measurable disease by RECIST 1.1. The study included a safety phase 1b lead-in with ciforadenant 100 mg BID orally, nivolumab 3 mg/kg, and ipilimumab 1 mg/kg q3 weeks and a phase 2 dose-expansion. The primary objective was to assess safety and depth of response >50% based on a Bayesian design (H0 32%, H1 47%). Bulk RNA sequencing was performed on baseline tissue available in 29 patients:
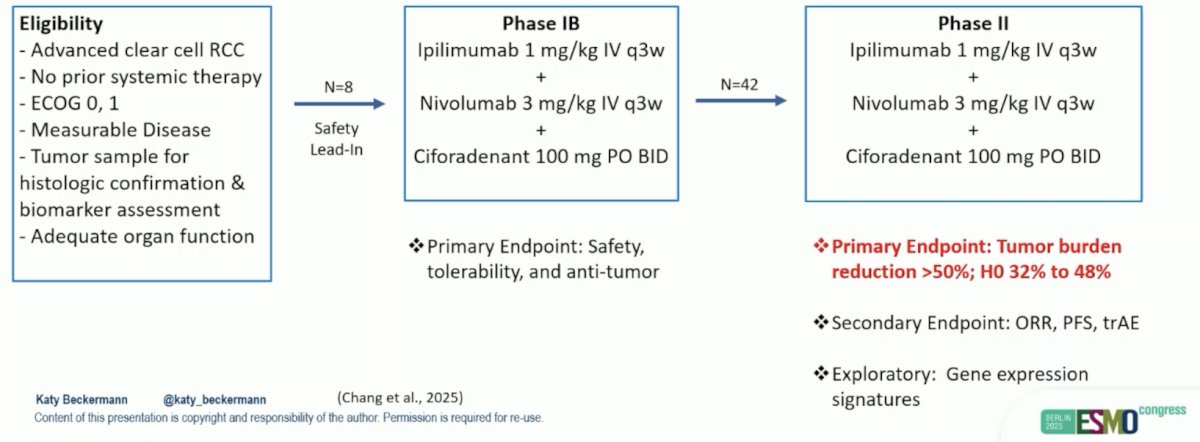
At the data cutoff (April 16, 2025), 51 patients were enrolled from 4 centers. One patient withdrew early without dose-limiting toxicity in phase 1b for 50 evaluable patients. The patients had a median age of 61.5 (IQR 53-70) years, and IMDC categories included 18% favorable, 71% intermediate, and 10% poor risk: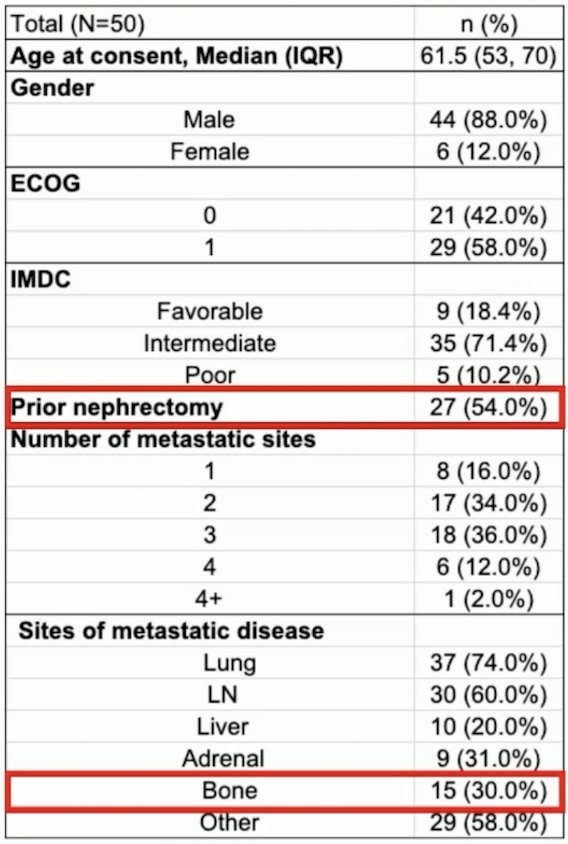
The median follow-up is 9.4 months, during which 17 patients (34%) achieved >50% tumor shrinkage, and the objective response rate was 46% (95% CI 33%, 60%):
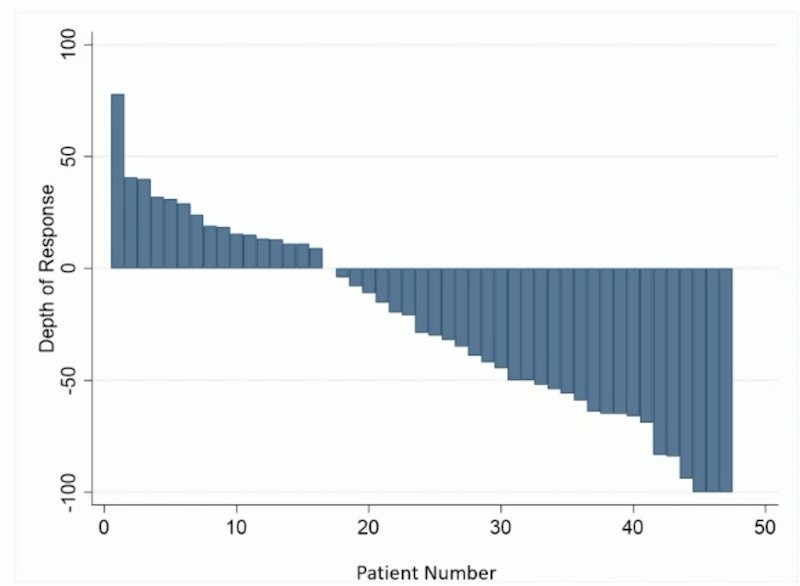
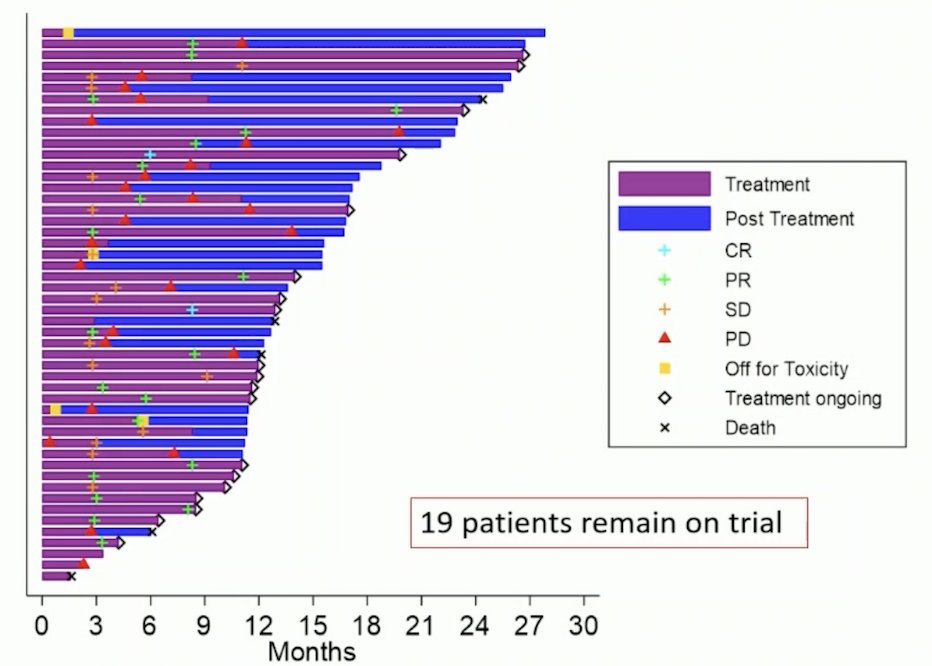
There were 16% of patients who had progressive disease as best response, and the median progression-free survival was 11.0 months (95% CI 7.1, 13.8). The median duration of response was 8.51 months (95% CI 2.66 – not evaluable), with 19% of patients remaining on trial:
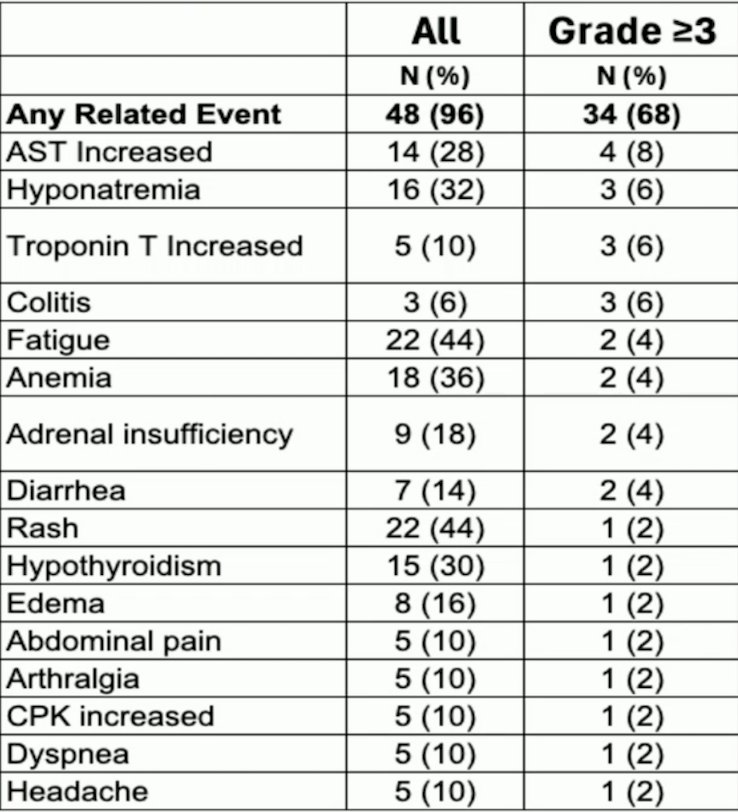
The grade 3 or higher adverse event rate was 68% with the most common all-grade treatment-related adverse events being fatigue, rash, AST and ALT increase, and hyponatremia. One patient died of immune checkpoint inhibitor overlap syndrome. Treatment discontinuation secondary to toxicity occurred in 5 patients (10%):
RNA signatures, including a previously identified exploratory adenosine signature,1 did not enrich for response to treatment, while the IMmotion 151/OPTIC immunotherapy [2] cluster demonstrated significantly higher objective response rates (100% in immunotherapy with n = 4 vs 30% in Angio cluster with n = 21, p = 0.032) and correlated with progression free survival:
![RNA signatures, including a previously identified exploratory adenosine signature,1 did not enrich for response to treatment, while the IMmotion 151/OPTIC immunotherapy [2] cluster demonstrated significantly higher objective response rates (100% in immunotherapy with n = 4 vs 30% in Angio cluster with n = 21, p = 0.032) and correlated with progression free survival:](/images/com-doc-importer/231-astro-2025/astro-2025-phase-1b-2-trial-of-ipilimumab-nivolumab-and-ciforadenant-in-first-line-advanced-rcc-a-kidney-cancer-research-consortium-study/image-5.jpg)
Dr. Beckermann concluded her presentation discussing results from a phase 1b/2 trial of ipilimumab, nivolumab, and ciforadenant in first-line advanced RCC with the following take-home points:
- Triplet therapy (ipilimumab, nivolumab, and ciforadenant) is feasible and well-tolerated in the KCRC study
- In this interim analysis of a single-arm study, the deep response rate/objective response rate was not significantly affected by the addition of ciforadenant to ipilimumab/nivolumab
- Comprehensive correlative analyses highlight the complexity of adenosine biology and provide support for biomarker trials
- Key questions remain, and a longer follow-up is needed to determine whether adenosine signaling blockade influences the durability of response
Presented by: Kathryn Beckermann, MD, PHD, Medical Director of GU Clinical Research/ Medical Oncology, Tennessee Oncology, Nashville, TN
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.
Related content: Phase Ib/II Trial Combines Ciforadenant with Ipilimumab and Nivolumab in Frontline Kidney Cancer - Kathryn Beckermann
References:
- Fong L, Hotson A, Powderly JD, et al. Adenosine 2A receptor blockade as an immunotherapy for treatment-refractory renal cell cancer. Cancer Discov. 202 Jan;10(1):40-53.
- Motzer RJ, Banchereau R, Hamidi H, et al. Molecular subsets in renal cancer determine outcome to checkpoint and angiogenesis blockade. Cancer Cell. 2020 Dec 14;38(6):803-817.