(UroToday.com) The 67th American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco, between September 28 and September 30 was host to the Session 28 - GU 6: Revelations in Renal Radiotherapy. Dr. Hiroshi Onishi presented abstract 265 - Long-Term Follow-up Results after Stereotactic Body Radiotherapy (SBRT) for Primary Renal Cell Carcinoma: A Prospective Multicenter Phase 2 Trial.
Dr. Onishi opened his presentation by reviewing the historical perception of RCC as radioresistant when treated with conventional fractionation. He cited work by Ning et al., which reported α/β values of 2.6 and 6.92 Gy for RCC cell lines, suggesting potential radiosensitivity at larger fraction sizes. Given that an α/β ratio below 3 Gy favors hypofractionation, SBRT may reduce chronic toxicity to surrounding tissues while preserving tumor control. Supporting this, large fraction SBRT regimens (26 Gy in a single fraction or 42–48 Gy across three fractions) have demonstrated favorable outcomes and are now recommended as an optimal approach in International Stereotactic Radiosurgery Society (ISRS) guidelines.
Currently, there are no clinical data to define the true α/β ratio of RCC, leaving the biological rationale for very large fraction doses uncertain and unsupported by evidence. Against this background, the present study was designed to evaluate the long-term efficacy and safety of SBRT delivered in a 10-fraction regimen for RCC.
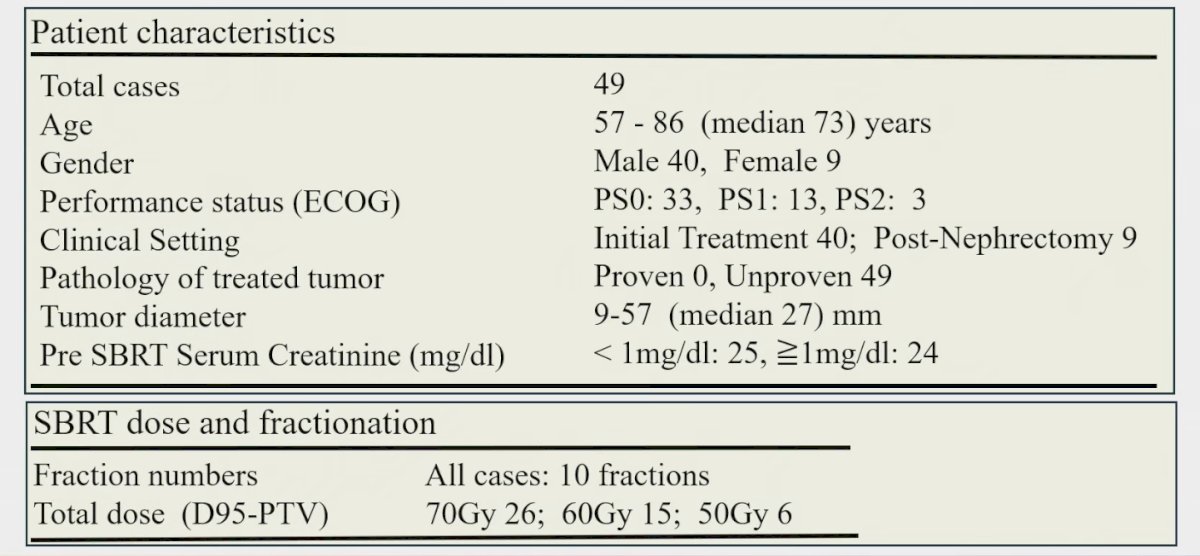
Dr. Onishi presented findings from a multicenter, prospective phase 2 trial conducted across six centers in Japan. Eligible patients had an ECOG performance status of 0–2 and a clinical diagnosis of RCC, with or without biopsy confirmation, and were enrolled if they were medically inoperable, at high surgical risk, or declined surgery. SBRT was delivered in 10 fractions with doses of 50, 60, or 70 Gy prescribed as D95 to the PTV, while maintaining normal tissue dose constraints. The primary endpoint was local control, defined as the absence of progression within the irradiated field, with secondary endpoints including treatment-related adverse events, PFS, OS, and CSS.
A total of 49 patients were enrolled, with a median age of 73 years and a predominance of male participants. Nine patients had undergone prior nephrectomy, and the median tumor size was 27 mm. Patient characteristics are shown below. All patients were free of nodal or distant metastases at baseline. SBRT doses were prescribed as 70 Gy in 26 patients, 60 Gy in 15, and 50 Gy in 8. Enrollment occurred between August 2007 and May 2017, with follow-up ranging from 16 to 169 months (median, 76 months).
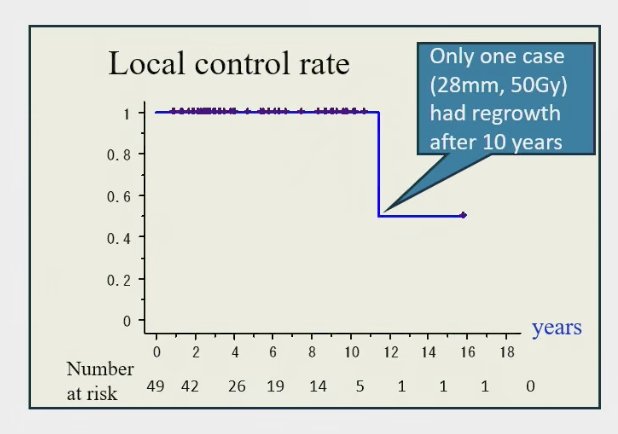
At 11.4 years, the local control rate was 100%, with durable responses maintained over long-term follow-up. Only a single patient, with a 28 mm tumor treated at 50 Gy, experienced in-field regrowth after 10 years.
The 5- and 10-year PFS rates were 84.9% and 70.8%, respectively, with corresponding OS rates of 73.2% and 49.8%. Cancer-specific survival remained favorable, at 95.2% and 87.2% at 5 and 10 years. Notably, CSS was significantly higher among patients who received SBRT as their initial therapy, with a 10-year CSS of 97.3%, compared to those with a history of contralateral nephrectomy.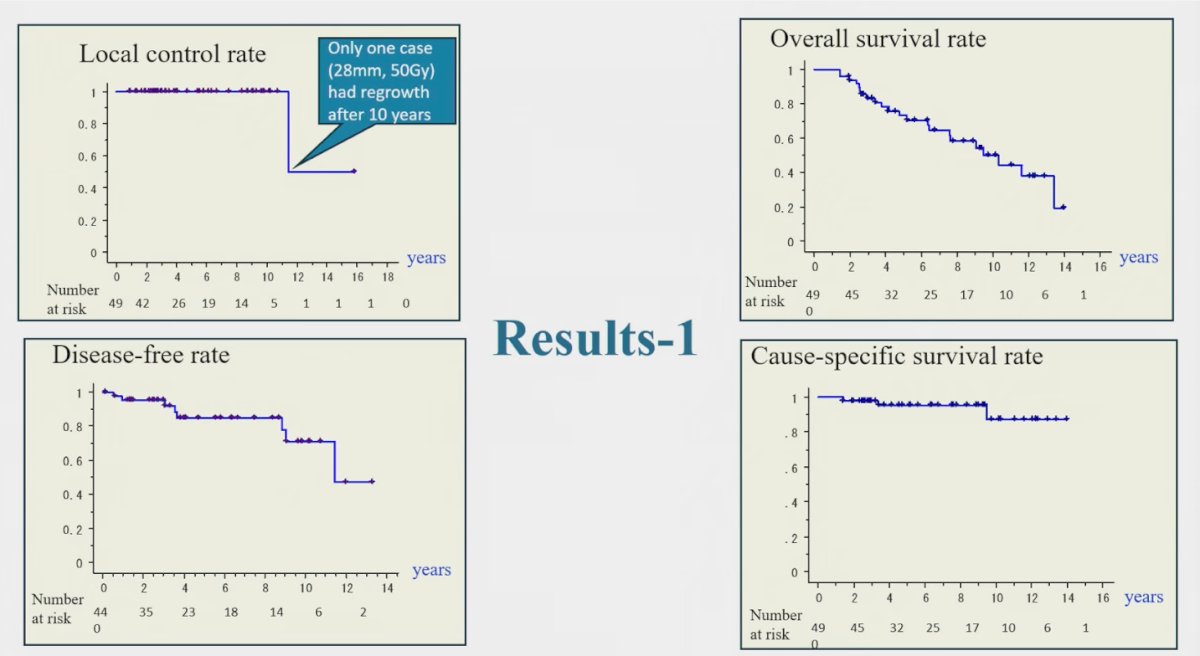
On multivariable analysis, tumor size showed a trend toward significance for overall survival (p=0.06), while clinical setting (initial SBRT versus post-nephrectomy) was significantly associated with both OS (p=0.03) and disease-free rate (p<0.01). Age, performance status, and SBRT dose were not significant predictors.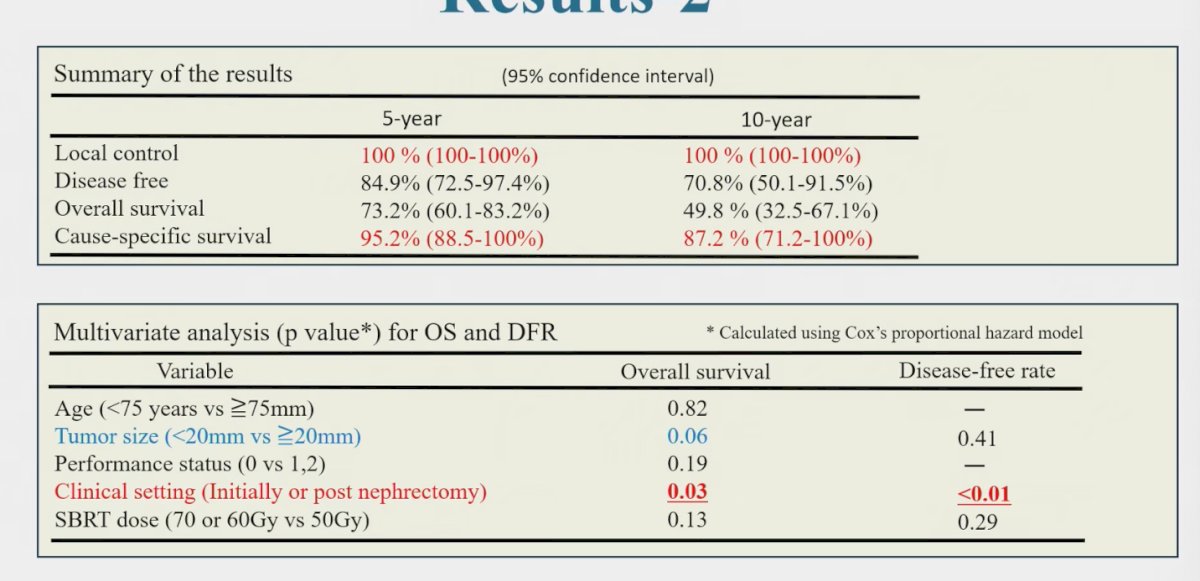
Treatment was generally well tolerated. Grade 3–4 gastrointestinal adverse events occurred in two patients (4.1%), both with tumors adjacent to the duodenum or colon and treated with 70 Gy in 10 fractions. Additionally, 12 patients (24.5%) developed an increase in serum creatinine ≥1.0 mg/dL during follow-up, with renal function decline more common among those with a solitary kidney following prior nephrectomy.
When compared with prior SBRT series in RCC, this study stands out for having the longest median follow-up at 76 months. Local control remained excellent, with a 100% rate at 12 months and durable responses thereafter. As summarized in the table, outcomes were comparable or superior to previous reports, with a low incidence of grade 3 gastrointestinal toxicity (2%). These findings highlight the long-term efficacy and safety of a 10-fraction SBRT regimen for RCC.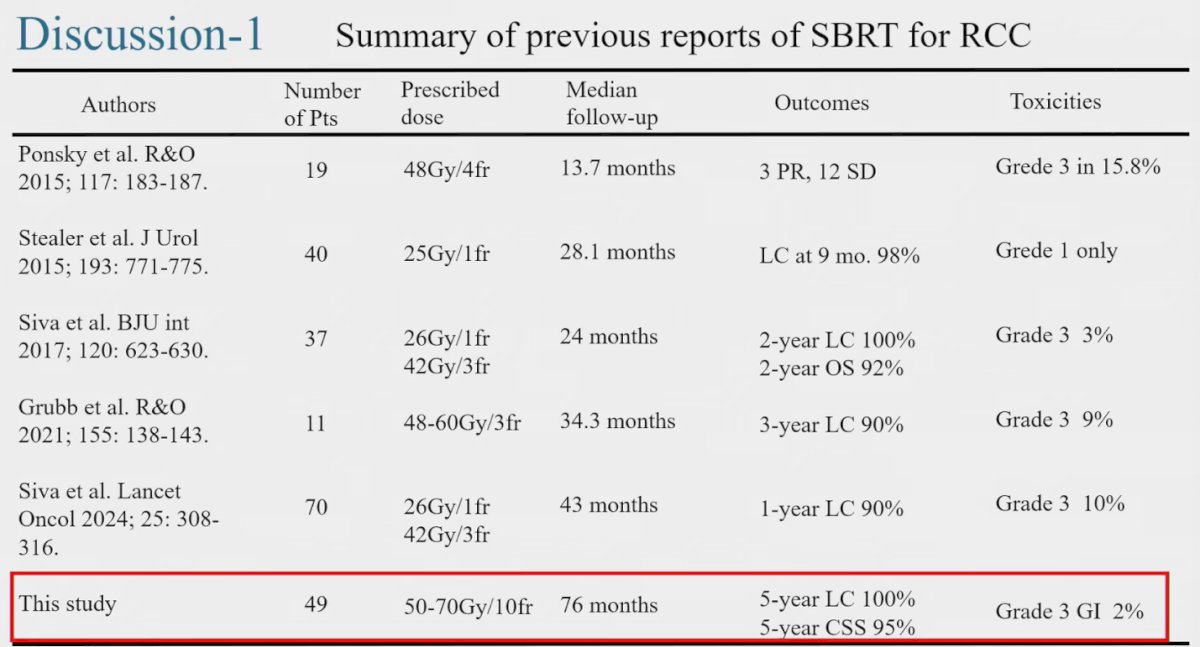
Dr. Onishi highlighted the ISRS practice guidelines, which recommend SBRT regimens of 26 Gy in one fraction for tumors ≤4–5 cm, 42–48 Gy in three fractions for tumors >4–5 cm, or 40 Gy in five fractions when organ-at-risk constraints preclude three-fraction treatment. In contrast, his study employed 50–70 Gy delivered in 10 fractions, which he noted may be particularly useful for tumors located adjacent to the intestine, where stricter dose constraints apply. He further emphasized that if the α/β ratio of RCC is closer to 7 Gy, such a fractionation schedule provides an effective balance between tumor control and treatment safety.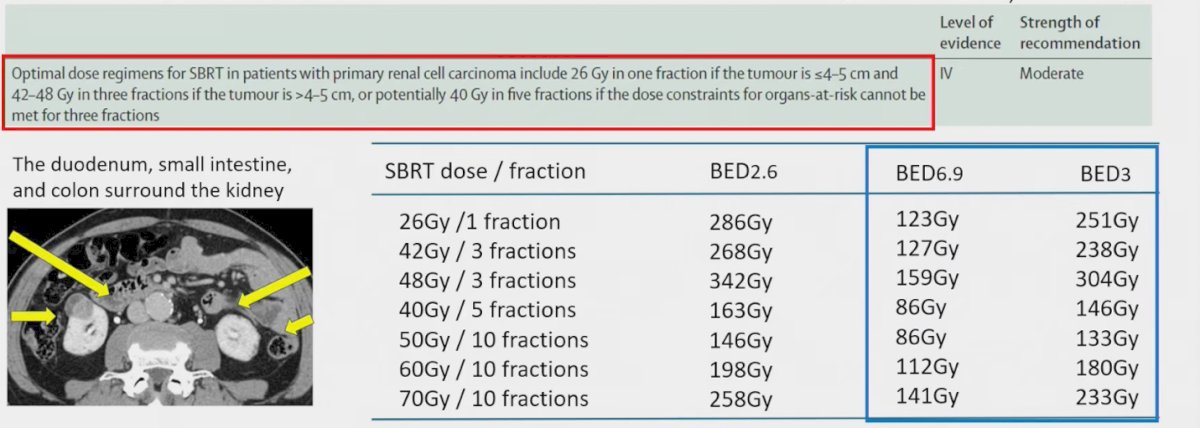
Key limitations of this study include the absence of pathological confirmation in all cases, reliance on older 3D-conformal radiotherapy techniques rather than modern IMRT, and the possibility that the α/β ratio of RCC may be heterogeneous across patients.
Dr Onishi concluded his presentation with the following key messages:
- SBRT with 50–70 Gy in 10 fractions demonstrated excellent long-term local control and cause-specific survival in patients with primary RCC.
- Grade 3–4 gastrointestinal adverse events occurred in two patients (4.1%); since this trial, dose constraints have become stricter in routine practice.
- This fractionation protocol may offer advantages over less-fractionated regimens by reducing toxicity when bowel or other critical organs are near the target, particularly if the α/β ratio of RCC is closer to 7 Gy.
- Clinical setting (initial treatment vs. post-nephrectomy) was a significant factor for overall survival, disease-free rates, and renal dysfunction.
- These long-term results support SBRT as a potentially curative option for patients unwilling or unfit for surgery and provide a strong rationale for future randomized trials comparing SBRT with surgery in primary RCC.
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Cancer Treatment and Research Center (CTIC), Luis Carlos Sarmiento Angulo Foundation via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco between the 28th of September and the 30th of September.