(UroToday.com) The 67th American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco, between September 28 and September 30 was host to the Session 28 - GU 6: Revelations in Renal Radiotherapy. Dr. Ryan Assadi presented abstract 263 - Stereotactic Radiation for Systemic Therapy-naïve Oligometastatic Kidney Cancer: Final Results of a Phase IIb Trial.
Dr. Assadi opened his presentation by outlining the global landscape of renal cell carcinoma, noting an annual incidence of approximately 431,000 cases and 180,000 deaths worldwide. The median age at diagnosis is 75 years, compared to 64 years in the United States. Key risk factors include obesity, hypertension, chronic kidney disease, and smoking, while hereditary syndromes such as VHL, HLRCC, HPRC, and BHD, along with germline mutations in VHL, FH, MET, and FLCN, also contribute.1 Between 15–20% of patients present with metastatic disease, and 30% experience recurrence or distant metastasis, with a 5-year overall survival of only 18.2% per SEER data. Current management includes systemic therapy with PD-1 inhibitors, ICIs, or TKIs, metastasectomy, and Stereotactic Ablative Radiotherapy (SABR); however, systemic treatment carries grade ≥3 toxicities in 30–85% of patients.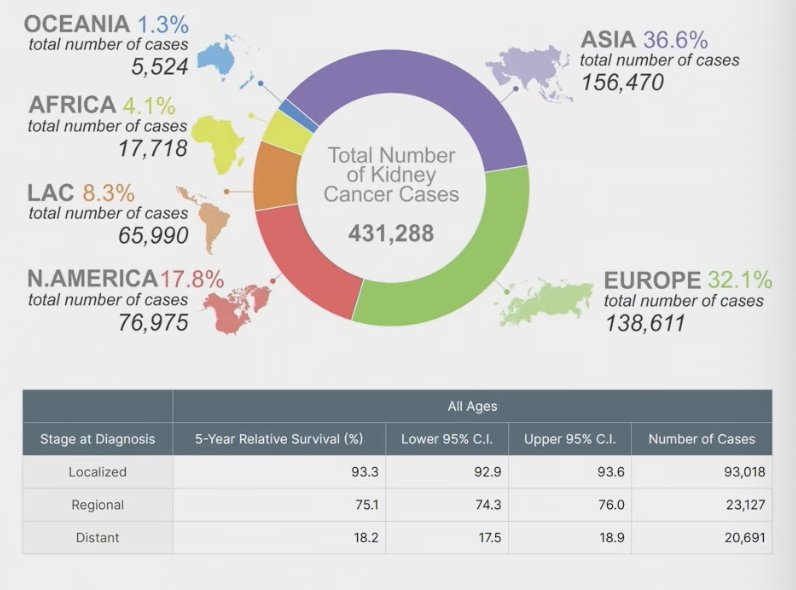
Investigation into local therapies for mRCC has been ongoing, with metastasectomy shown to improve OS in select patients. (2) While RCC has historically been considered radioresistant to conventional fractionation, SABR has emerged as a strategy to overcome this by delivering higher doses per fraction, achieving local control rates >95% with minimal toxicity as shown below. Importantly, SABR also allows for repeat application across additional sites and sequential treatments, making it an appealing option in patients with indolent disease biology.
Clinical data, such as the UTSW retrospective experience of 47 patients treated with SABR to 88 metastases, demonstrated a 91.5% local control rate at 2 years and a median delay in systemic therapy initiation of 15.2 months without significant ≥G3 toxicity. These findings raise the question of which disease characteristics may favor an upfront systemic therapy approach versus a local therapy-first strategy, with current objectives focusing on whether delay in time to systemic therapy (TTST) can serve as a surrogate for PFS.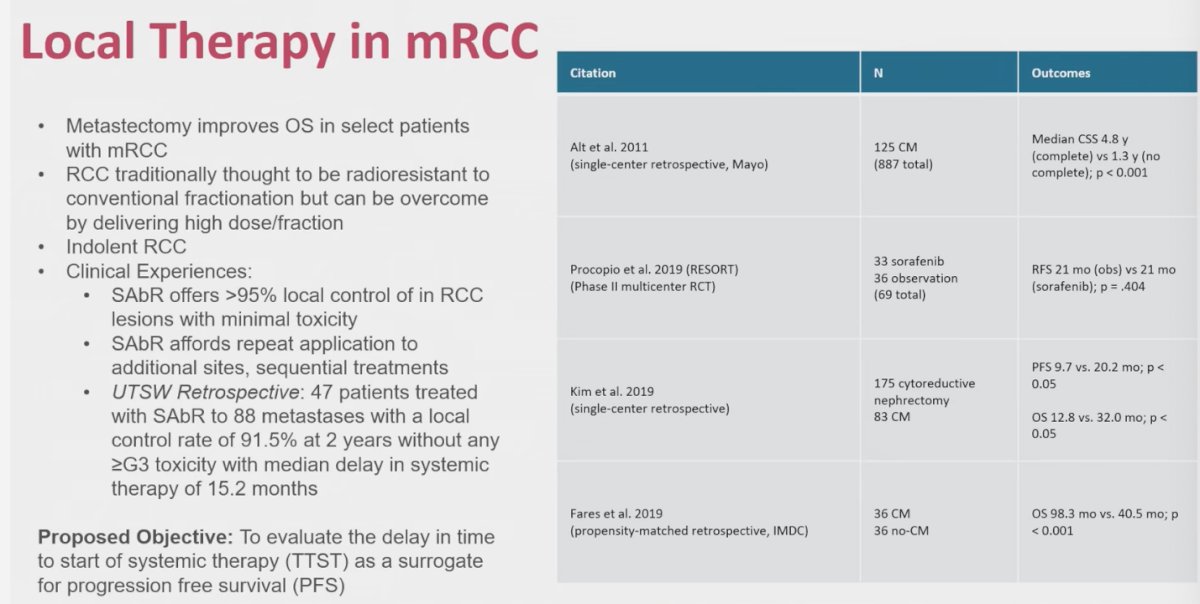
Dr. Assadi presented the trial design, highlighting the primary objective of evaluating whether SABR could delay the initiation of systemic therapy by more than one year in at least 60% of patients. Secondary objectives included modified progression-free survival, progression-free survival on subsequent therapy, overall survival, cancer-specific survival, local control, toxicity, and health-related quality of life. From a statistical perspective, enrollment of 23 patients provided 80% power at a significance level of 0.10 to detect a 20% improvement in one-year delay to systemic therapy compared to historical estimates. Kaplan-Meier methods were used for survival endpoints, and mixed model analyses were applied for quality-of-life outcomes.
Eligibility criteria required patients to have three or fewer sites of metastatic renal cell carcinoma, be suitable for stereotactic ablative radiotherapy (SABR) to all metastatic lesions, and have fewer than three poor prognostic factors as defined by MSKCC, with no brain metastases. A complete metastatic work-up and baseline assessments were performed prior to enrollment. SABR was delivered to all measurable oligometastatic sites, with sequential SABR permitted for new lesions if disease control was maintained, as illustrated below.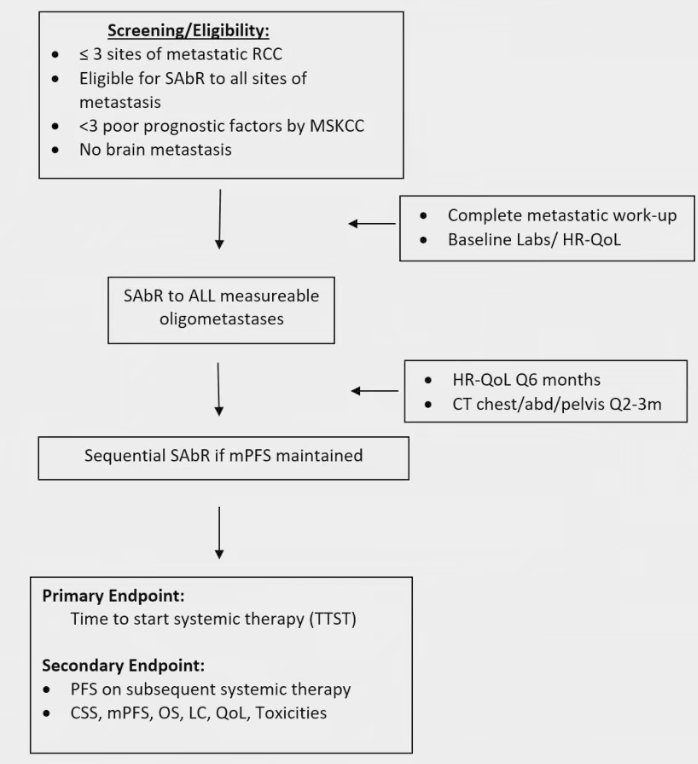
They defined objective progression for sequential local therapy using mPFS criteria: more than 3 new sites of metastasis at one imaging interval, new sites not amenable to SAbR, more than 6 total sites requiring SAbR, local failure at a previously treated site, or development of brain metastases. RECIST 1.1 was used to define new lesions and local failure. This framework provides an objective balance to guide the timing of systemic therapy while accounting for the multifactorial nature of progression in patients managed with sequential focal approaches.
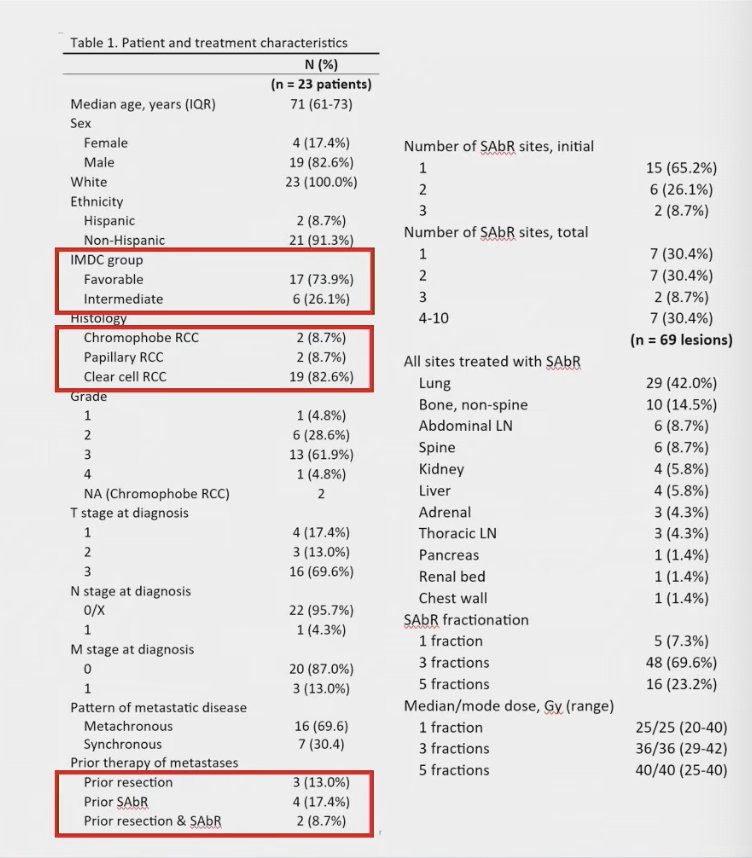
Patient enrollment went from November 2017 to February 2021, with most patients classified as IMDC favorable risk (n=17) and predominantly clear-cell RCC (n=19). All but one were systemic therapy naïve. At baseline, 33 lesions were treated, and 11 patients later received sequential SABR to 36 additional lesions. Lesion sites included the lungs (42%), abdominal lymph nodes (9%), and bone (9% spine, 15% non-spine). Treatment regimens included 25 Gy in a single fraction, 12 Gy across three fractions, or 8 Gy across five fractions as shown in the table below.
With a median follow-up of 45 months (IQR 26–57), progression defined by mPFS included >3 new metastases in 5 patients, new sites not amenable to SAbR in 3 patients, and >6 sites requiring SAbR in 2 patients. No local failures were observed at treated sites, while 1 patient developed brain metastasis. Additionally, 5 patients died prior to initiating systemic therapy, 3 were unsuitable for systemic treatment and 2 died from unrelated causes while remaining with no evidence of disease (NED) as shown in the Swimmers plot below.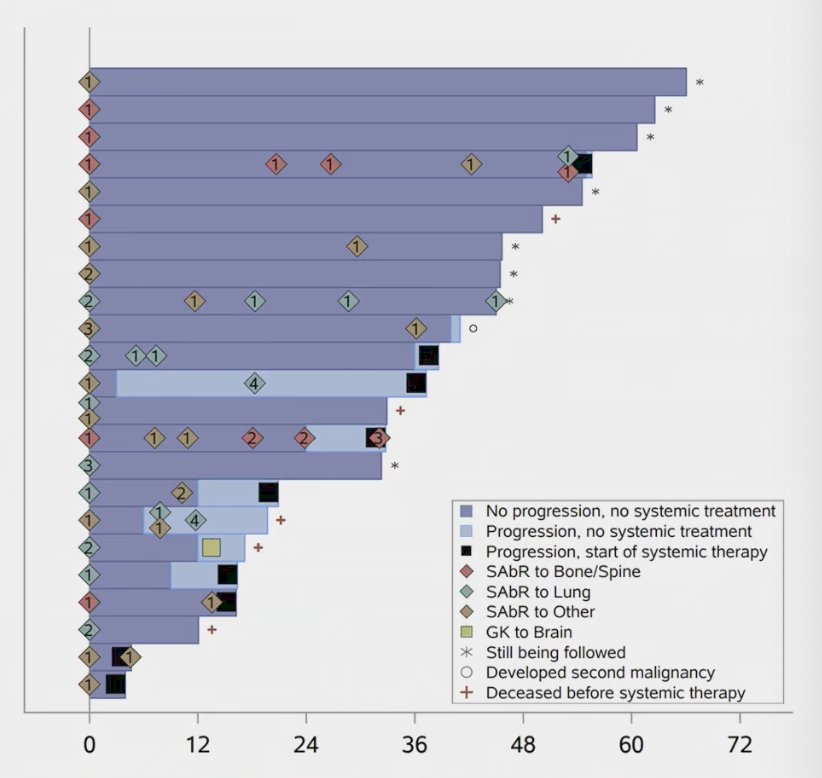
Freedom from systemic therapy at 1 year was 91% (95% CI: 69.5–97.8). The median time to start systemic therapy was 55.6 months, with 9 patients eventually requiring systemic treatment. Median mPFS was 40 months, with 9 patients meeting mPFS criteria within the 3-year enrollment period and 2 additional patients meeting criteria during registry follow-up. Importantly, SAbR-treated sites demonstrated a local control rate of 100%.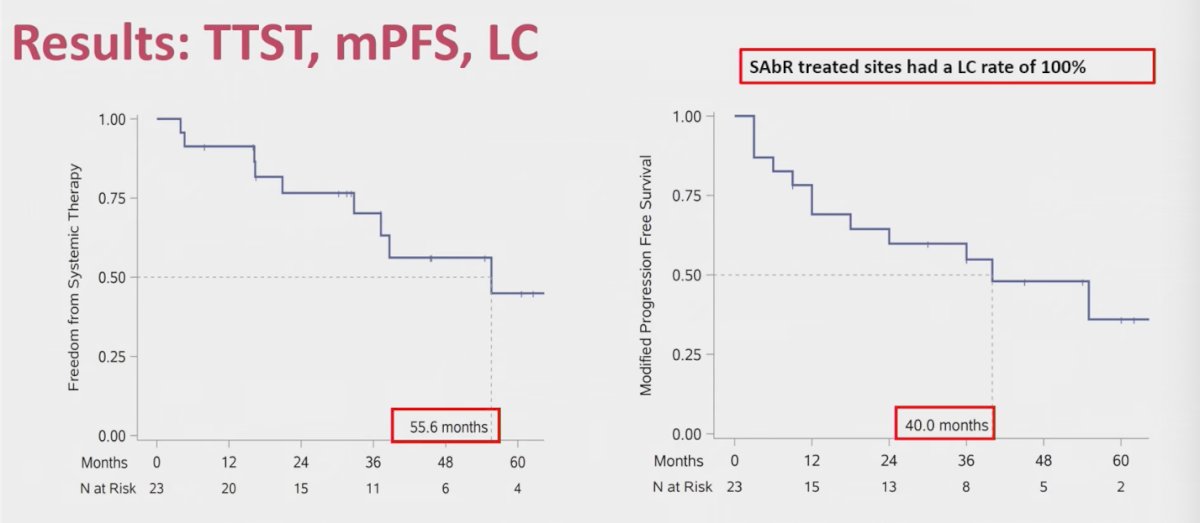
Furthermore, the PFS on subsequent therapy was 5.7 months, which at first glance may appear modest. However, this should be interpreted in the context that patients had already received one or two prior lines of systemic therapy. Overall survival was consistent with published literature, with 91% at 18 months and 68.7% at 36 months. Cancer-specific survival was favorable, reaching 91% at 18 months and 87% at 36 months.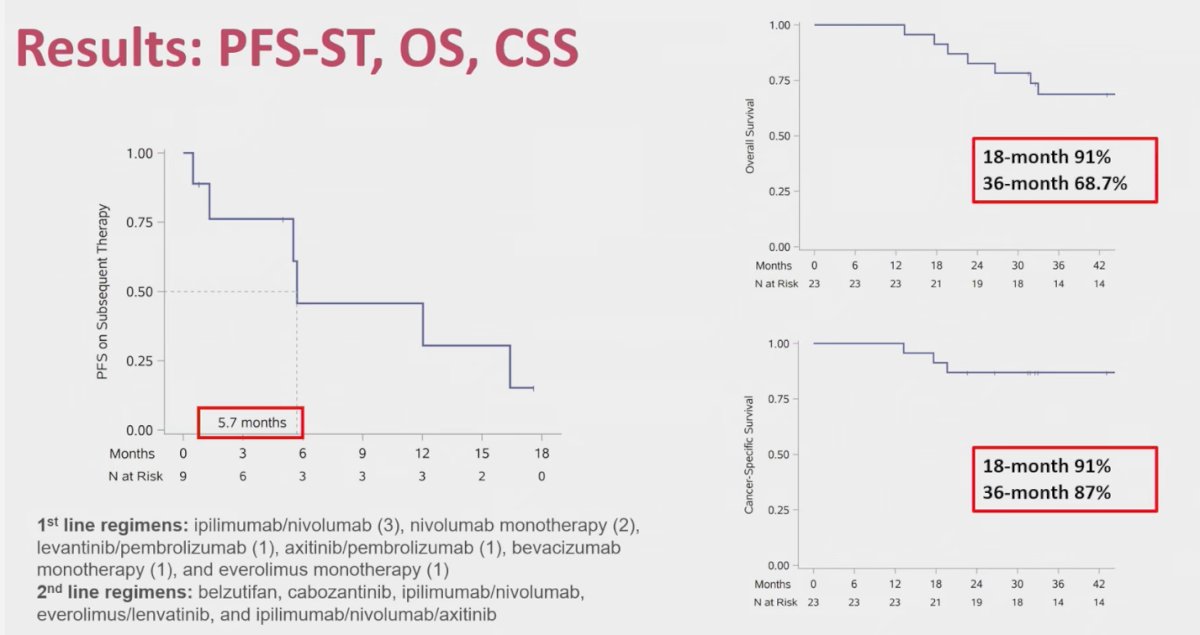
Importantly, there were no statistically significant positive or negative effects on quality of life, which the investigators noted as a key win for local therapy. Only one case of grade ≥3 toxicity was reported, possibly related to treatment (ICI colitis), translating to a 4% rate substantially lower than the 30–85% rates typically observed with first-line systemic therapies. Patient-reported health-related quality of life remained stable across all domains measured by EQ-5D-5L, FACT-G, and FKSI, contrasting with the declines often seen with systemic therapy.
This is the first phase 2b trial evaluating systemic therapy–naïve oligometastatic RCC. The study exceeded its prescribed benchmark, affirming and extending prior retrospective analyses, while standing out as unique compared to other prospective oligometastatic RCC trials. Importantly, it applied a novel, objective definition of disease progression for sequential local therapy and demonstrated preservation of HR-QoL. Limitations noted included the lack of validated patient selection criteria, small sample size, single-institution design, single-arm structure, and focused inclusion criteria.
Dr. Assadi concluded his presentation with the following key takeaways:
- SABR may represent a safe and effective first-line option for patients with oligometastatic RCC, offering the ability to delay initiation of systemic therapy.
- The phase 2b data exceeded benchmarks, preserved HR-QoL, and supported prior retrospective findings.
- To confirm these benefits, including potential impact on long-term survival outcomes, phase III randomized data are required.
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Cancer Treatment and Research Center (CTIC), Luis Carlos Sarmiento Angulo Foundation via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco between the 28th of September and the 30th of September.
Reference:
- Fares AF, Araujo DV, Calsavara V, Saito AO, Formiga MN, Dettino AA, Zequi S, da Costa WH, Cunha IW. Complete metastasectomy in renal cell carcinoma: a propensity-score matched by the International Metastatic RCC Database Consortium prognostic model. Ecancermedicalscience. 2019 Oct 14;13:967. doi: 10.3332/ecancer.2019.967. PMID: 31921338; PMCID: PMC6834380.
- Bukavina L, Bensalah K, Bray F, Carlo M, Challacombe B, Karam JA, Kassouf W, Mitchell T, Montironi R, O'Brien T, Panebianco V, Scelo G, Shuch B, van Poppel H, Blosser CD, Psutka SP. Epidemiology of Renal Cell Carcinoma: 2022 Update. Eur Urol. 2022 Nov;82(5):529-542. doi: 10.1016/j.eururo.2022.08.019. Epub 2022 Sep 10. PMID: 36100483.