(UroToday.com) The 67th American Society for Radiation Oncology (ASTRO) annual meeting held in San Francisco, was host to the Revelations in Renal Radiotherapy session. Dr. Muhammad Ali presented Abstract # 68067 - Neoadjuvant Pembrolizumab and Stereotactic Radiotherapy Prior to Nephrectomy for Renal Cell Carcinoma (NAPSTER): A Phase II Randomized Clinical Trial.
Dr. Ali highlighted that there remains a significant risk of recurrence following surgery for RCC, with 5–15% of patients experiencing local recurrence and up to 50% developing distant metastases. She noted that despite this high-risk landscape, five randomized trials evaluating adjuvant immune checkpoint inhibitors (ICIs) have been reported to date—IM-010 (atezolizumab), PROSPER (nivolumab), KN-564 (pembrolizumab), CM-914 (nivolumab/ipilimumab), and RAMPART (durvalumab/tremelimumab) with only KN-564 showing a positive result both in disease-free survival (DFS) and overall survival (OS).1

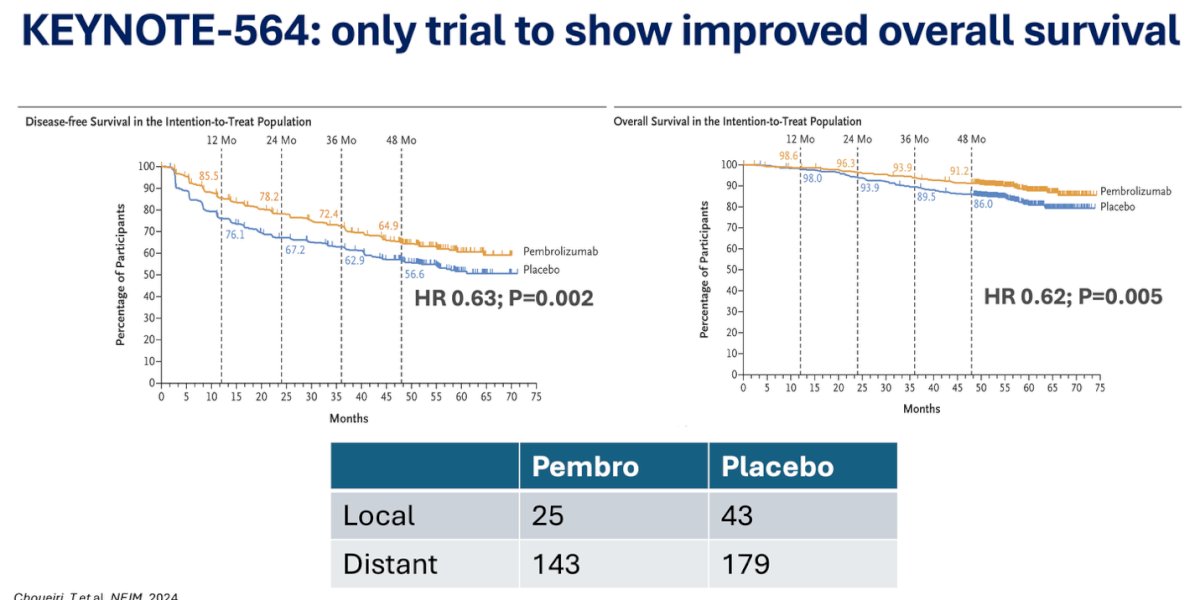
The phase III KEYNOTE-564 trial remains the only study in the perioperative RCC setting to demonstrate an OS benefit with adjuvant immunotherapy. In this trial, 1,000 patients were randomized to one year of pembrolizumab or placebo following nephrectomy. Pembrolizumab significantly improved both disease-free survival (HR 0.63; p=0.002) and overall survival (HR 0.62; p=0.005), with separation of the survival curves maintained over time. Despite these benefits, rates of local and distant recurrence remained notable, underscoring the ongoing need for improved strategies to further reduce relapse risk.1
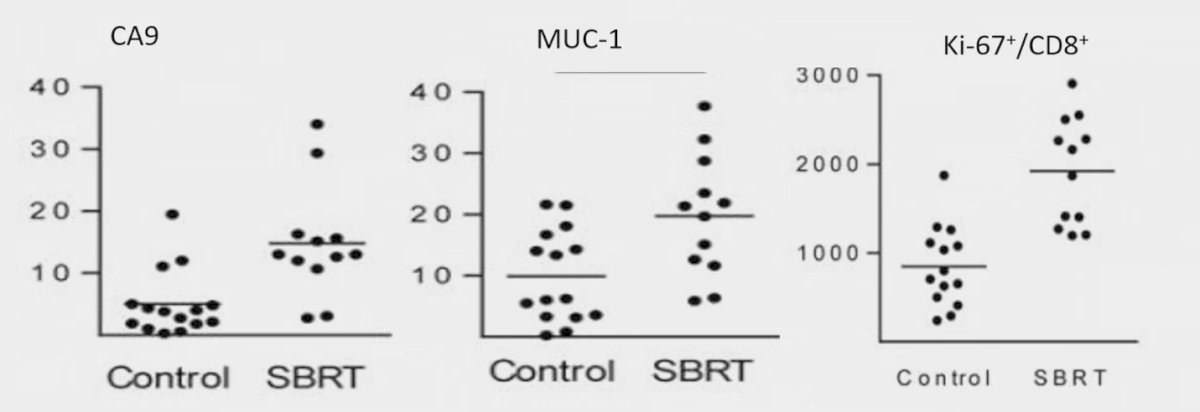
A pilot study of stereotactic body radiation therapy (SBRT) combined with cytoreductive nephrectomy in metastatic RCC enrolled 16 patients with stage IV disease planned for nephrectomy. Patients received a single 15 Gy fraction four weeks prior to surgery. The approach was associated with increased tumor-associated antigens, including CA9 and MUC-1 (shown below), as well as higher Ki-67 expression and enhanced T-cell infiltration, suggesting potential immune-priming effects of SBRT in this setting.2
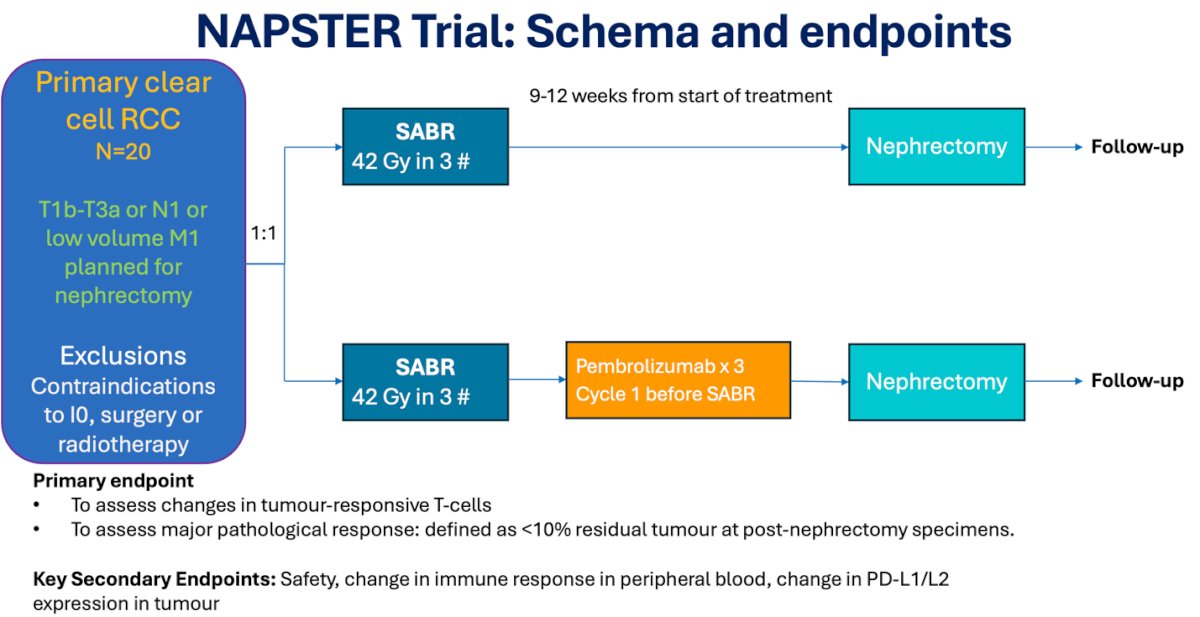
The NAPSTER trial is a two-site study conducted at Princess Margaret Cancer Centre and Princess Alexandra Hospital, evaluating neoadjuvant SABR with or without pembrolizumab in patients with clear cell RCC (T1b–T3a, N1, or low-volume M1) planned for nephrectomy. Twenty patients are randomized 1:1 to SABR (42 Gy in 3 fractions) alone or three cycles of pembrolizumab followed by SABR, with nephrectomy performed 9–12 weeks later. The primary endpoints are changes in tumor-responsive T cells and major pathological response, while key secondary endpoints include safety, immune response in peripheral blood, and PD-L1/L2 expression. The study schema is shown below.
In the NAPSTER trial, 23 patients with renal masses were enrolled, of whom 3 had non–clear cell histology and were excluded. Twenty patients were treated: 9 received neoadjuvant SABR alone, and 11 received SABR plus immunotherapy, with 2 of the latter group not proceeding to surgery due to anesthetic risk or patient decision. The median age was 64 years in the SABR group and 68 years in the SABR/IO group. Tumor characteristics were comparable between arms, with median maximal dimension of 6.2 cm vs 6.0 cm, and median tumor volumes of 204.6 cc vs 145.8 cc, respectively.

In terms of safety, grade 1–2 adverse events were common across both arms, while grade 3 events occurred in 22% of patients receiving SABR (duodenitis, hematuria) and 9% in the SABR/IO group (fatigue). Radical nephrectomy was successfully completed in 18 patients, with no additional technical challenges reported by surgeons. Surgical morbidity was low, with one grade 2 wound complication in the SABR group, and in the SABR/IO arm one grade 2 wound infection, one grade 2 hematoma, and one grade 3 hematoma were reported. Overall, the neoadjuvant approaches were feasible and manageable from a safety perspective

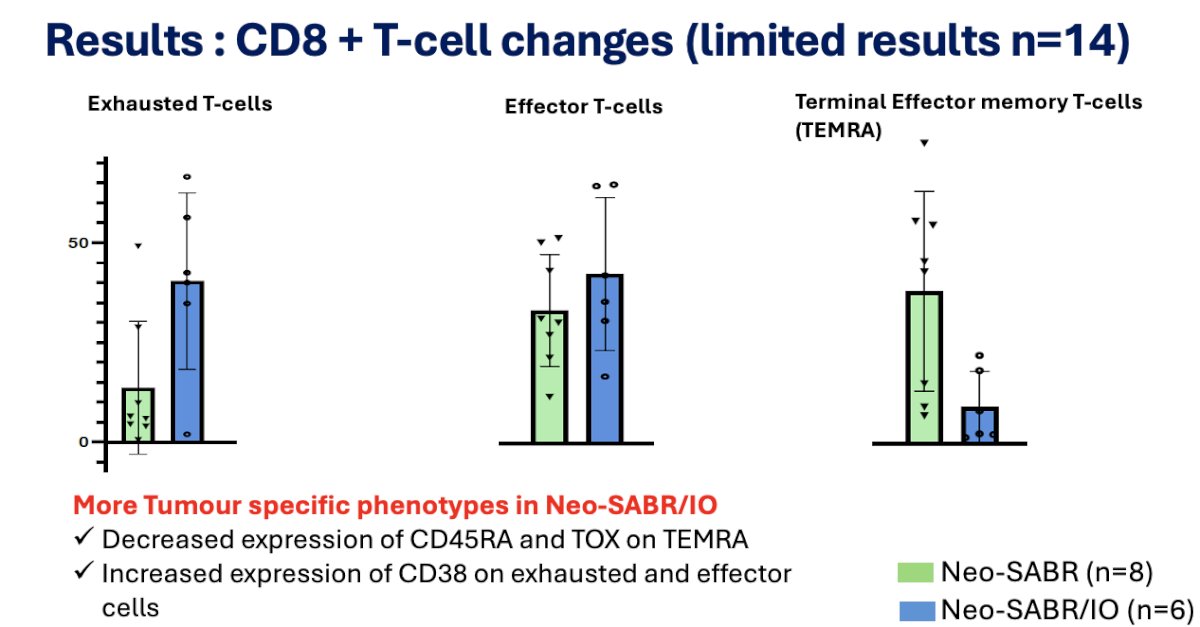
Molecular analysis is still ongoing; however, immune profiling from a subset of 14 patients demonstrated notable CD8+ T-cell changes. In the SABR/IO group, higher levels of exhausted T cells were observed, likely reflecting pembrolizumab-mediated reinvigoration and proliferation. Both treatment groups showed an increase in effector T cells, while SABR/IO was associated with fewer terminal effector memory T cells (TEMRA). These findings suggest that neoadjuvant SABR, particularly when combined with immunotherapy, may promote more tumor-specific T-cell phenotypes.
Dr. Ali highlighted that two patients who declined surgery after receiving neoadjuvant SABR/IO have remained free from both local and distant progression at 3 years and 2.5 years of follow-up, respectively, underscoring the potential durability of response with this approach.
Lastly, a substantial number of trials have evaluated neoadjuvant strategies in RCC, including VEGFR-TKI and IO monotherapy, which demonstrate variable objective response rates and reductions in primary tumor size but most report a good safety profile. These experiences highlight the potential to integrate SABR into multimodal neoadjuvant approaches, aiming to enhance immune responses and optimize outcomes in localized and locally advanced disease.

Dr. Ali concluded with the following take-home messages:
- NAPSTER is the first randomized neoadjuvant trial to report the safety of SABR with or without pembrolizumab prior to nephrectomy.
- Neoadjuvant SABR and a short course of pembrolizumab are safe.
- This approach results in increased tumor-specific T-cell phenotypes.
- It may be less toxic and potentially more cost-effective than neoadjuvant ICIs, TKIs, or their combinations.
- More comprehensive analyses of T-cell changes using single-cell RNAseq, TCRseq, and CyTOF/CyTEK are awaited and will help guide future prospective studies in this space.
Written by: Julian Chavarriaga, MD, Urologic Oncologist at Cancer Treatment and Research Center (CTIC) Luis Carlos Sarmiento Angulo Foundation via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during tthe 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, Sat, Sept 27 – Wed, Oct 1, 2025.
Reference:
- Choueiri TK, Tomczak P, Park SH, Venugopal B, Ferguson T, Symeonides SN, Hajek J, Chang YH, Lee JL, Sarwar N, Haas NB, Gurney H, Sawrycki P, Mahave M, Gross-Goupil M, Zhang T, Burke JM, Doshi G, Melichar B, Kopyltsov E, Alva A, Oudard S, Topart D, Hammers H, Kitamura H, McDermott DF, Silva A, Winquist E, Cornell J, Elfiky A, Burgents JE, Perini RF, Powles T; KEYNOTE-564 Investigators. Overall Survival with Adjuvant Pembrolizumab in Renal-Cell Carcinoma. N Engl J Med. 2024 Apr 18;390(15):1359-1371. doi: 10.1056/NEJMoa2312695. PMID: 38631003.
- Singh AK, Winslow TB, Kermany MH, Goritz V, Heit L, Miller A, Hoffend NC, Stein LC, Kumaraswamy LK, Warren GW, Bshara W, Odunsi K, Matsuzaki J, Abrams SI, Schwaab T, Muhitch JB. A Pilot Study of Stereotactic Body Radiation Therapy Combined with Cytoreductive Nephrectomy for Metastatic Renal Cell Carcinoma. Clin Cancer Res. 2017 Sep 1;23(17):5055-5065. doi: 10.1158/1078-0432.CCR-16-2946. Epub 2017 Jun 19. PMID: 28630212; PMCID: PMC5581708.