(UroToday.com) The 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting held in San Francisco, CA between September 28th and 30th, 2025, was host to a bladder and post-prostatectomy radiation session. Dr. Alyssa Anne Granda presented a systematic review and meta-analysis of bladder-only versus whole pelvis radiotherapy in trimodality treatment (TMT) for lymph node negative muscle-invasive urothelial carcinoma of the bladder (MIBC).
Dr. Granda noted that bladder cancer is the 9th most common cancer worldwide, with MIBC accounting for 25% of bladder cancer cases. TMT is a standard of care option for select patients with MIBC and involves a maximal TURBT with concurrent chemoradiation. The optimal radiation target volume remains unclear – should we electively irradiate the pelvic lymph nodes in node-negative MIBC (i.e., should bladder-only [BORT] or whole pelvis radiotherapy [WPRT] be performed)?
To date, only a few studies have compared outcomes between WP-RT and BO-RT in the setting of TMT for N0 MIBC. This is the first comprehensive meta-analysis comparing BO-RT versus WP-RT.

The primary study objective was to compare the efficacy and toxicity of BO-RT versus WP-RT in patients with node-negative MIBC undergoing TMT for bladder preservation. The efficacy and toxicity outcomes were as follows:
- Efficacy:
- Overall survival (OS)
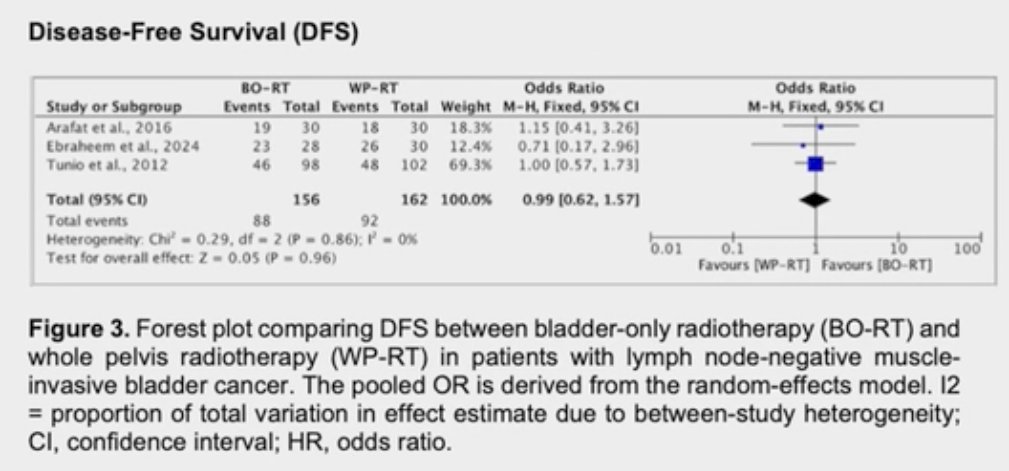
- Disease-free survival (DFS)
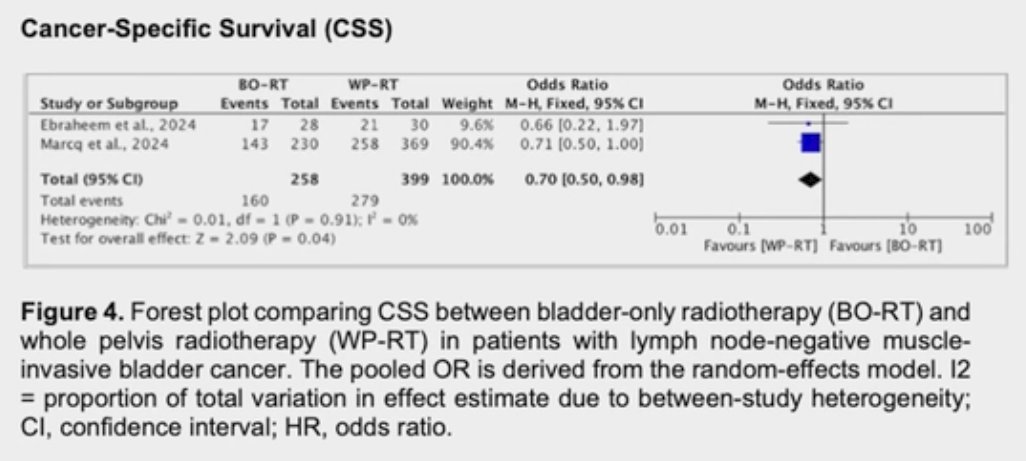
- Cause-specific survival (CSS)
- Toxicity:
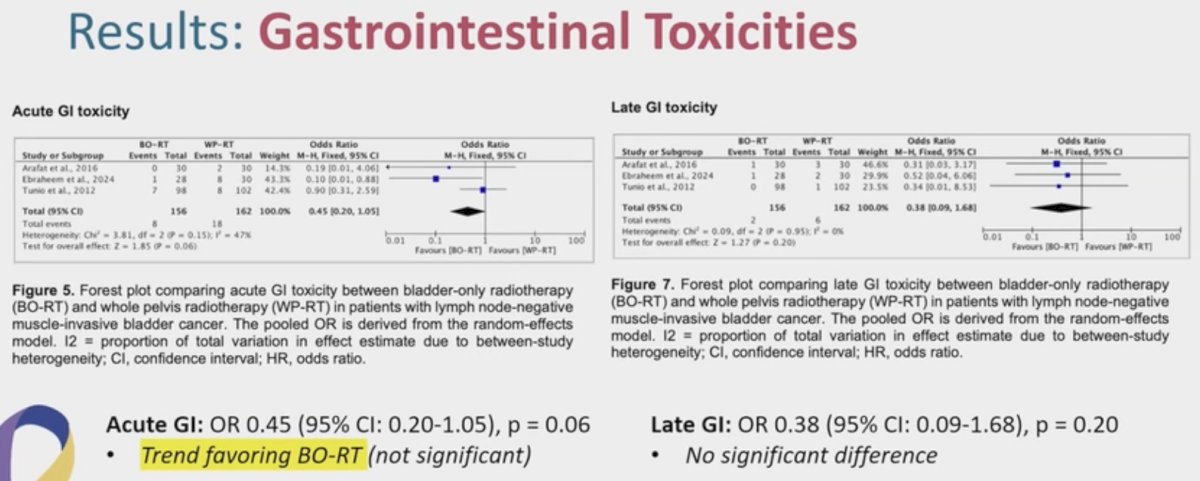
- Acute and late gastrointestinal (GI) toxicity
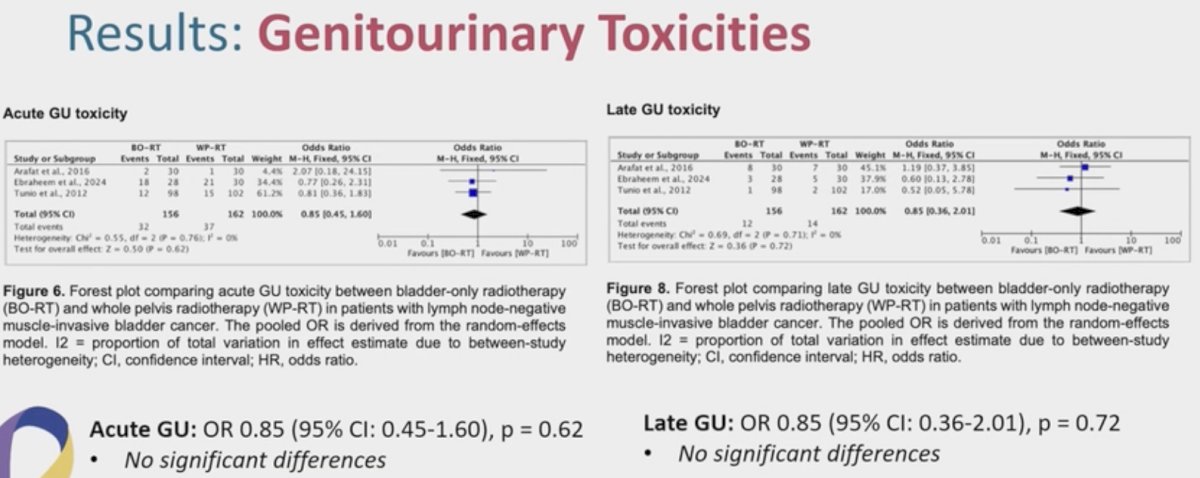
- Acute and late genitourinary (GU) toxicity
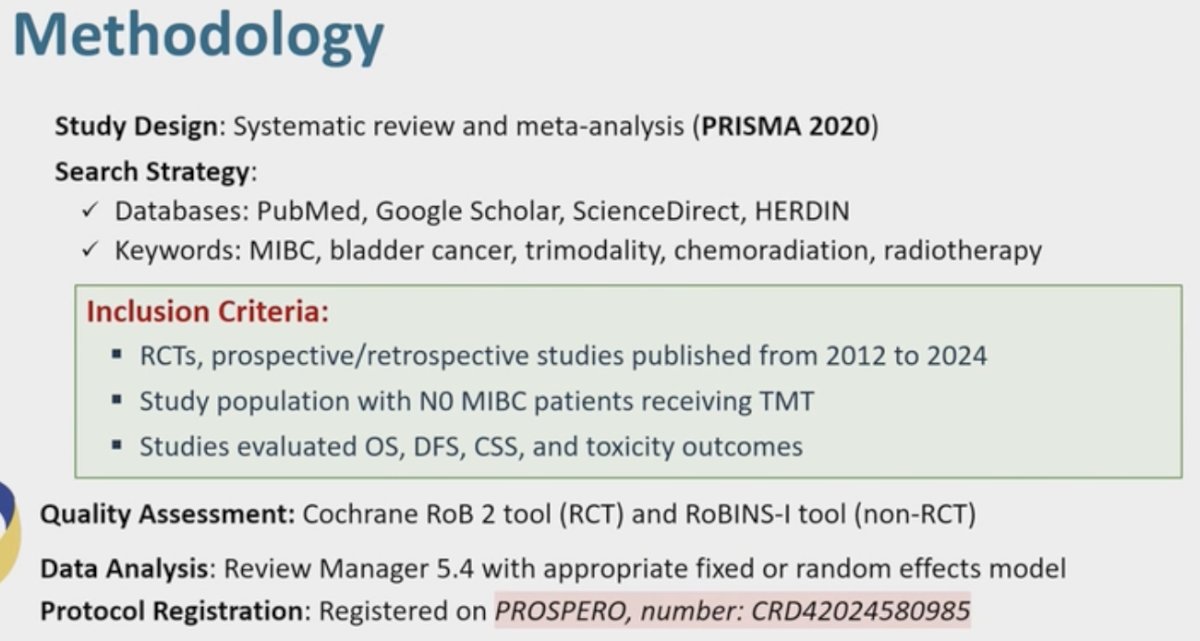
Dr. Granda and colleagues conducted a systematic review and meta-analysis of all randomized controlled trials and prospective/retrospective cohort studies evaluating TMT in N0 MIBC patients and reporting on OS, DFS, CSS, and toxicity outcomes.
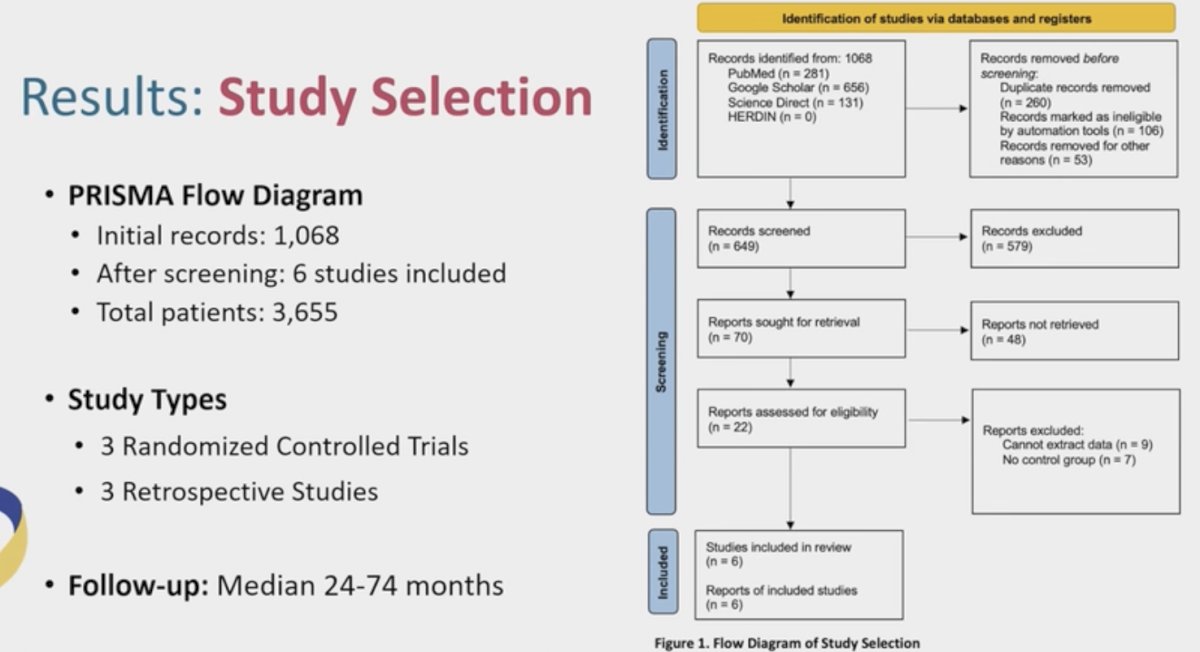
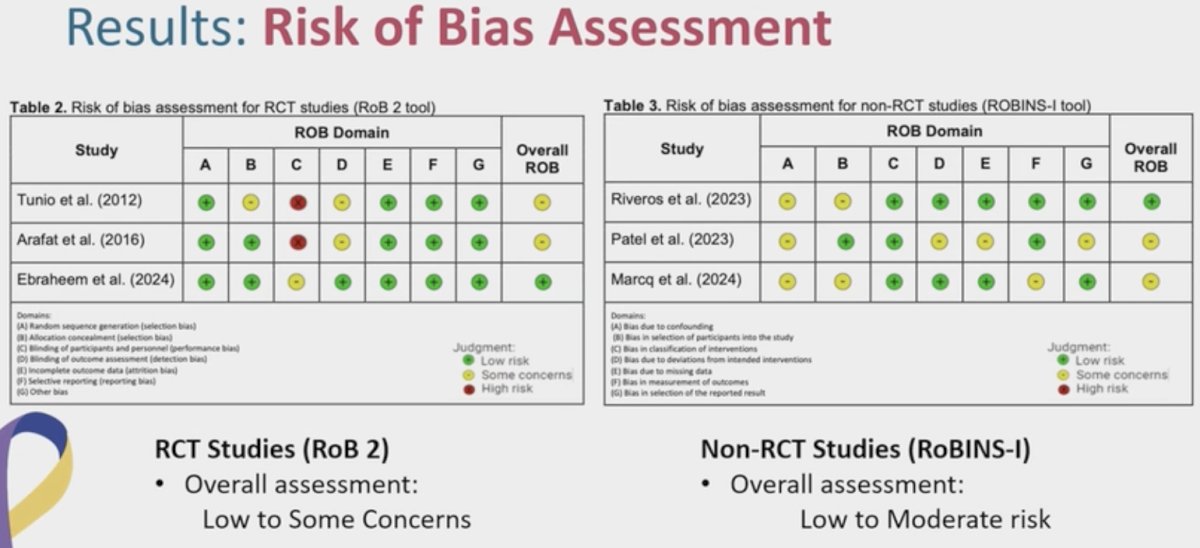
The final study cohort included 6 studies, of which 3 each were randomized controlled trials and retrospective studies. The median follow-up was 24-74 months.
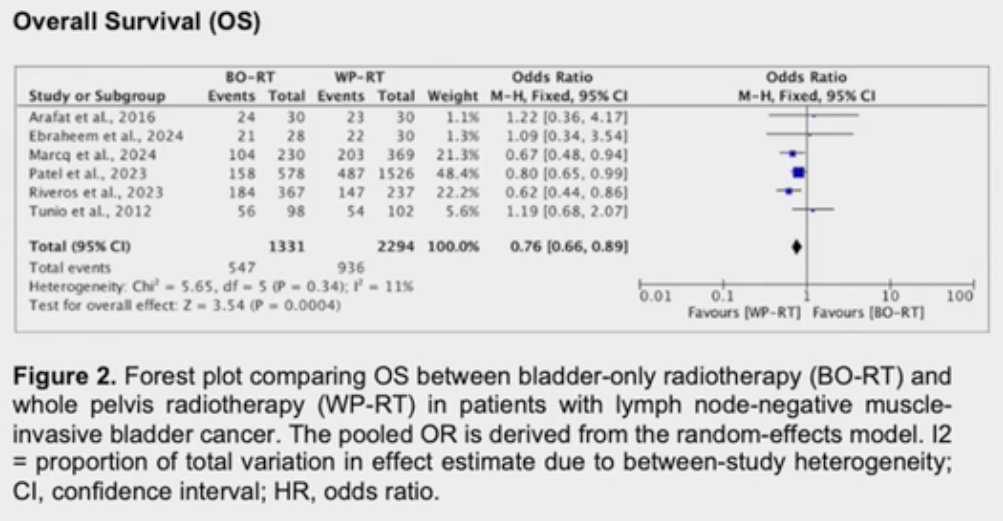
The pooled analysis of the OS outcome demonstrated that there was a 24% reduction in mortality with WP-RT (HR: 0.76, 95% CI: 0.66–0.89, p=0.0004).
Similarly, there was a 30% reduction in cancer-related deaths with WP-RT (HR: 0.70, 95% CI: 0.50-0.98, p=0.04).
There was no significant difference in DFS (OR: 0.99, p=0.96):
Acute GI toxicities favored BO-RT (OR: 0.45, p=0.06), but there were no significant differences in the odds of late GI toxicities (OR: 0.38, p=0.20).
There were no significant differences in the odds of acute or late GU toxicities.
Dr. Granda concluded as follows:
- WP-RT was associated with significant improvements in OSS and CSS
- Inclusion of the pelvic lymph nodes in the radiotherapy field may address potential micrometastases in the lymph nodes
- Up to 25% of N0 patients may harbor occult nodal disease
- The discrepancy between DFS and OS/CSS may be due to variations in recurrence patterns, success of salvage treatments, and individual patient characteristics
- Time to any recurrence was similar, but survival after recurrence favored WP-RT
- WP-RT did not prevent all recurrences, but improves salvage outcomes
- BO-RT may be associated with lower odds of acute GI toxicity (p=0.06), but with similar rates of late GI and both acute/late GU toxicities
- Smaller irradiated volume in BO-RT reduced bowel exposure
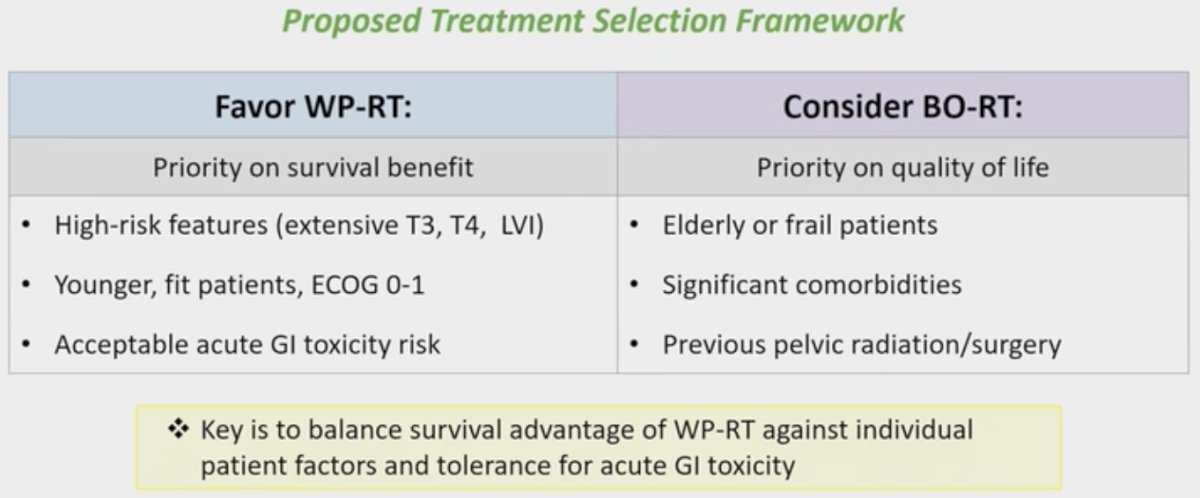
Dr. Granda and colleagues suggested the following proposed treatment selection framework:
Presented by: Alyssa Anne Granda, MD, Resident Physician, José R. Reyes Memorial Medical Center, University of Santo Tomas, Manila, The Philippines
Written by: Rashid K. Sayyid, MD, MSc, Urologic Oncologist, Department of Urology, The University of Arizona, @rksayyid on X during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, September 28th – 30th, 2025