(UroToday.com) The 2025 ASTRO annual meeting featured a plenary session and a presentation by Dr. Vedang Murthy discussing clinical outcomes from the phase III Bladder Adjuvant Radiotherapy (BART) multicenter randomized controlled trial. Advanced bladder cancer has several treatment modalities, including:
- Surgery: cystectomy (often with a urostomy bag)
- Adding chemotherapy: Neoadjuvant or adjuvant
- Overall survival improves 3-8% with cisplatin
- Adding nivolumab:1 adjuvant for 12 months (if available)
- Overall survival is 6-8%

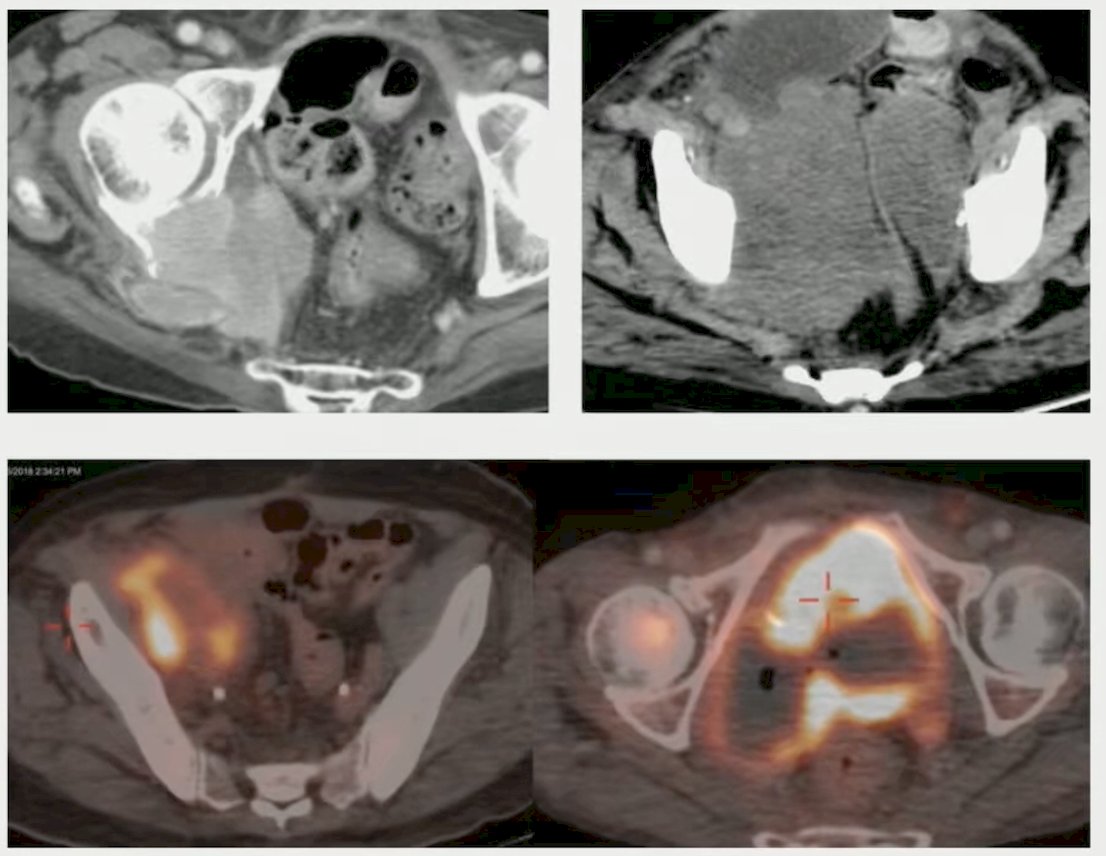
Dr. Murthy notes that it is firmly believed that a majority of failures are distant after cystectomy, but it is not well appreciated that locoregional recurrences are also a problem. Amongst several studies, the locoregional recurrence rate is ~30%, particularly for patients >= pT3, N+, those with <10 lymph nodes removed, LVI positive, and/or positive surgical margins. Locoregional recurrences can be a problem, with chemotherapy making little difference in these situations:
The objective of this trial was to report clinical outcomes from the multicenter phase III randomized trial of adjuvant radiotherapy after radical cystectomy and chemotherapy in locally advanced muscle invasive bladder cancer.
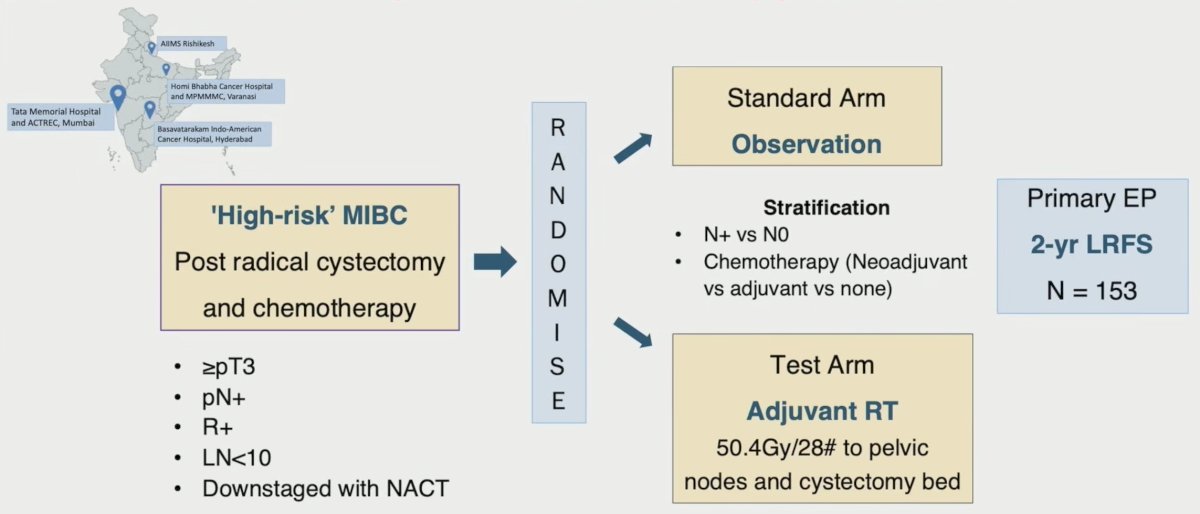
Patients with high-risk (T3-4, N1-3, R+) non-metastatic urothelial muscle invasive bladder cancer post-radical cystectomy were randomized 1:1 to adjuvant radiotherapy or observation, stratified by nodal stage (N0 versus N+) and chemotherapy (neoadjuvant/adjuvant/none). Cystectomy bed and pelvic nodes were treated with stoma-sparing adjuvant radiotherapy to 50.4Gy in 28 fractions. The primary endpoint of 2-year locoregional failure free survival and secondary endpoints of bladder cancer specific survival, disease free survival, and overall survival were compared per protocol by log rank test:
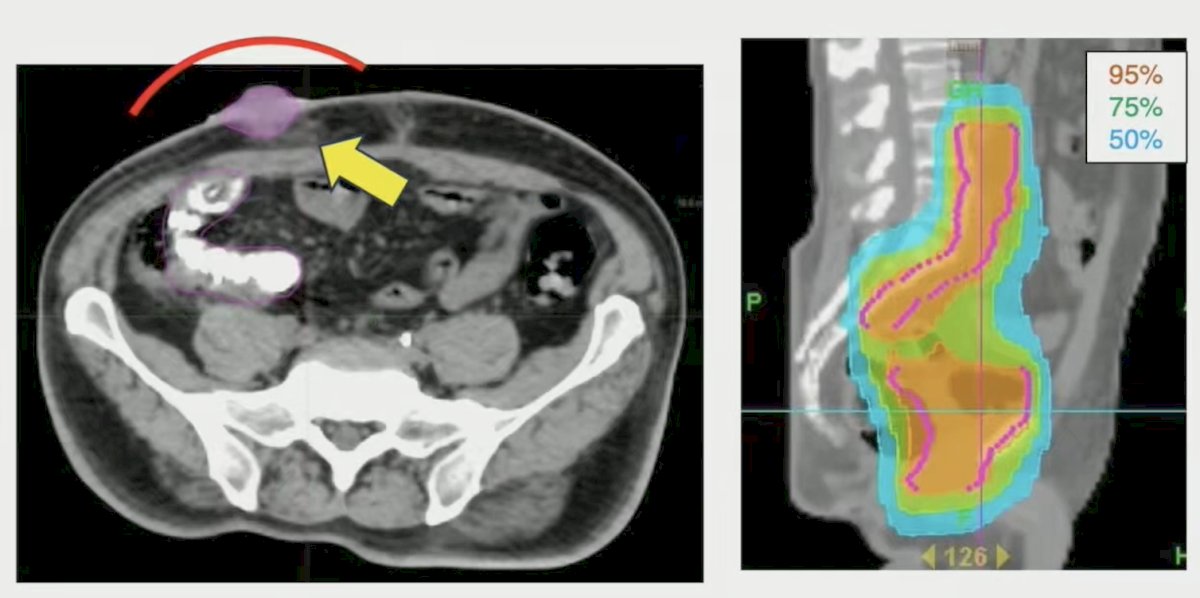
Competing risk analysis using Fine Gray model compared subdistribution hazard ratios for locoregional failure free survival (competing risks: distant metastases and non-cancer death) and disease free survival (competing risk: non-cancer death) between the two arms. Radiotherapy contouring included a CTV for the pelvis of common iliac, internal/external iliac, presacral, and obturator nodes, as well as a CTV including the cystectomy bed. Planning also included stoma and bowel sparing IMRT, as well as daily onboard image guidance:
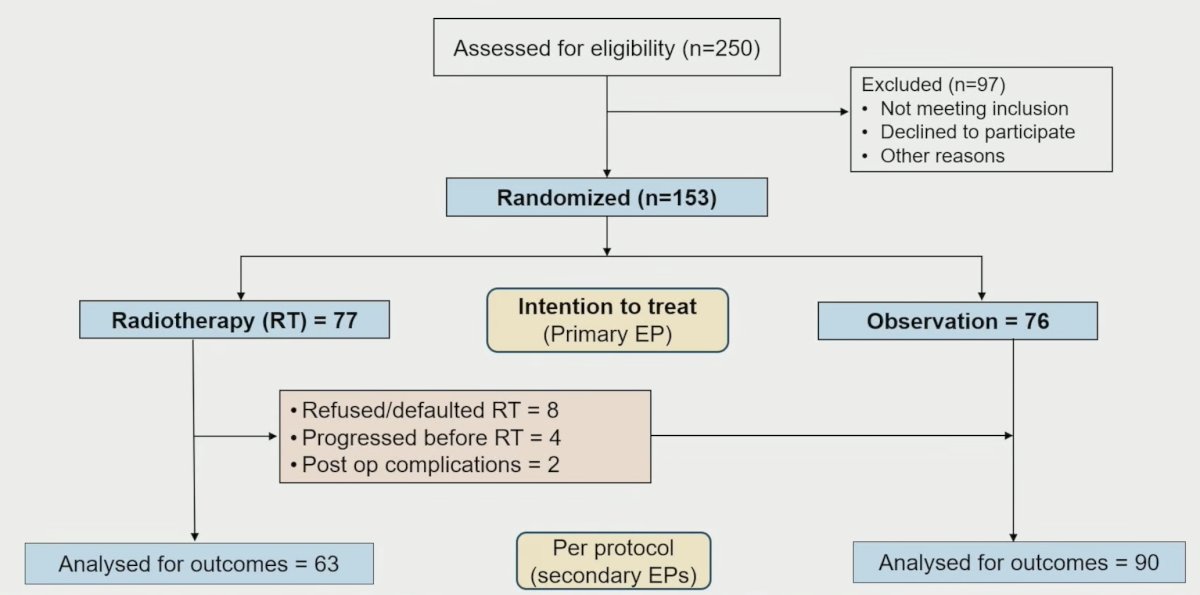
A total of 153 patients were randomized from 2016 to 2024 (adjuvant radiotherapy = 77, observation = 76). Overall, 62% patients had pT3-T4 and 41% had pN+ disease, and a variant histology component in 28% patients. Chemotherapy was neoadjuvant for 71% and adjuvant for 20% patients. No patients received immunotherapy:
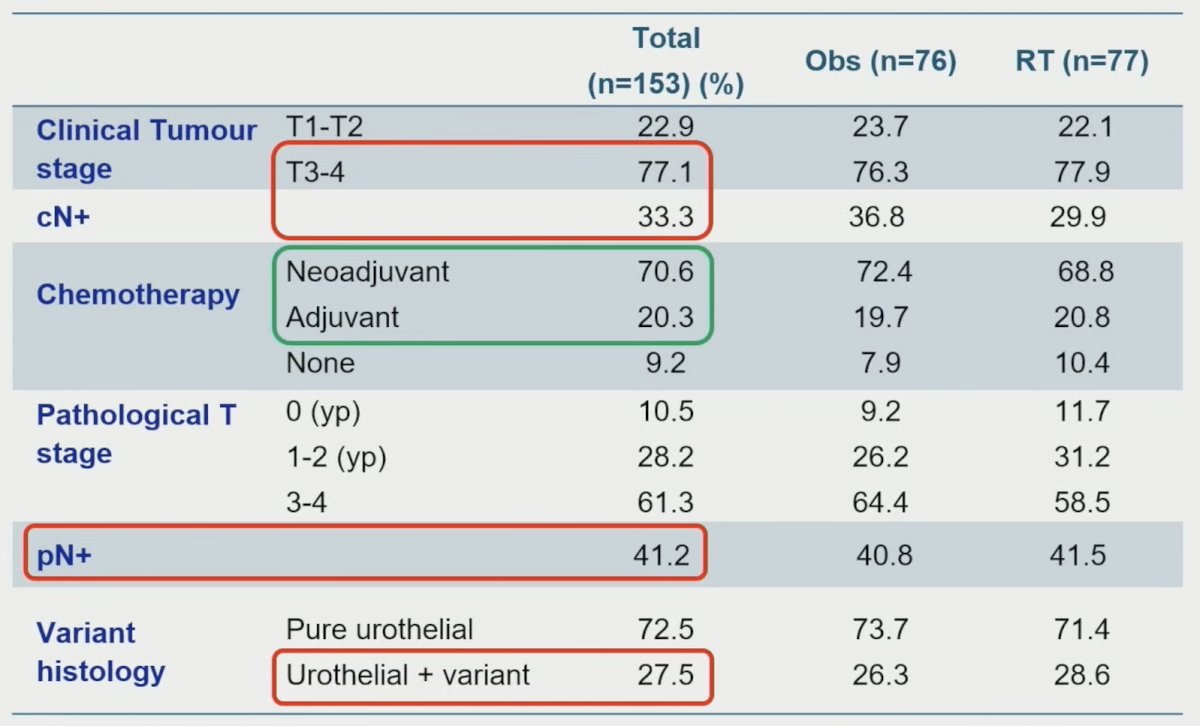
Additionally, the median age was 57 years of age, the median nodes dissected was 20, the positive margin rate was 4.6%, and 2.6% of patients had a neobladder. In the adjuvant radiotherapy arm, 63 received planned radiotherapy, and 14 (defaulted/refused radiotherapy = 8, pre-radiotherapy progression =4, radiotherapy deemed unfeasible = 2) were analyzed with the observation group (n = 90):
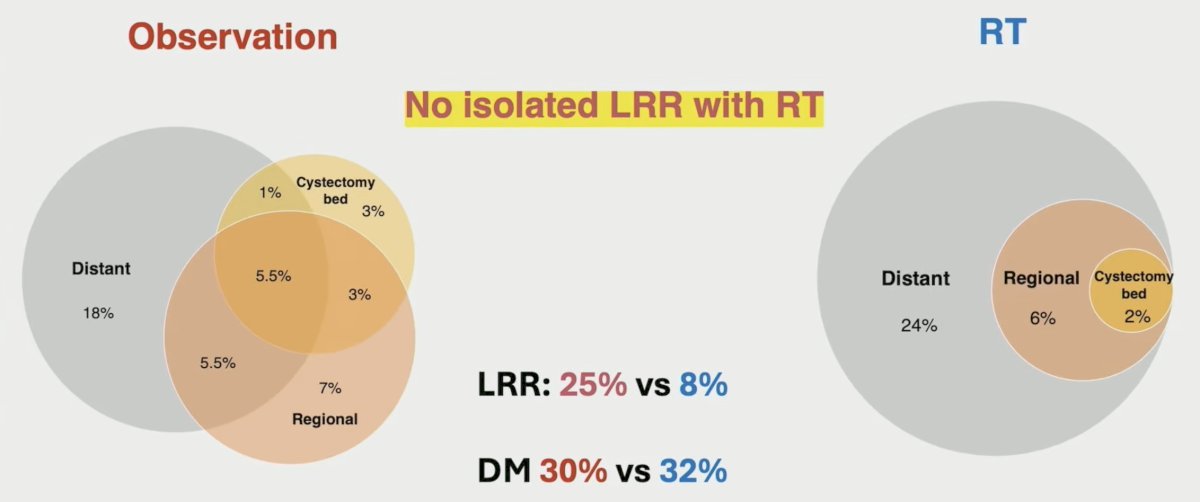
Over a median follow-up of 47 months, 37% of patients had recurred, with 18% locoregional recurrences (radiotherapy 8% versus observation 26%, p = 0.006). Two-year locoregional failure-free survival was 87.1% (adjuvant radiotherapy) versus 76.0% (observation) (HR 0.43, 95% CI 0.20-0.96, p = 0.04):

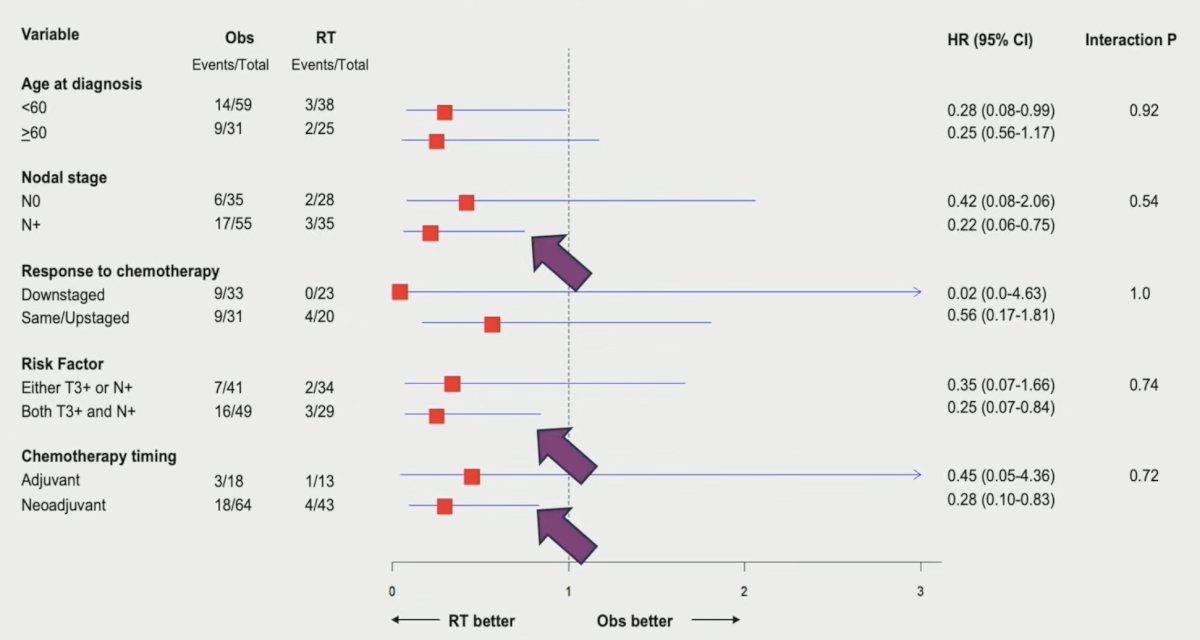
When assessing 2-year locoregional failure-free survival per protocol, the findings were even more impressive favoring adjuvant radiotherapy: 93.2% versus 75.0% (HR 0.27, 95% CI 0.10-0.71, p = 0.008). Subgroup analysis showed significant benefit in 2 year locoregional recurrence free survival with adjuvant radiotherapy in T3+ and N+ (HR 0.25, 95% CI 0.07-0.84) and N+ disease (HR 0.22, 95% CI 0.06-0.75):
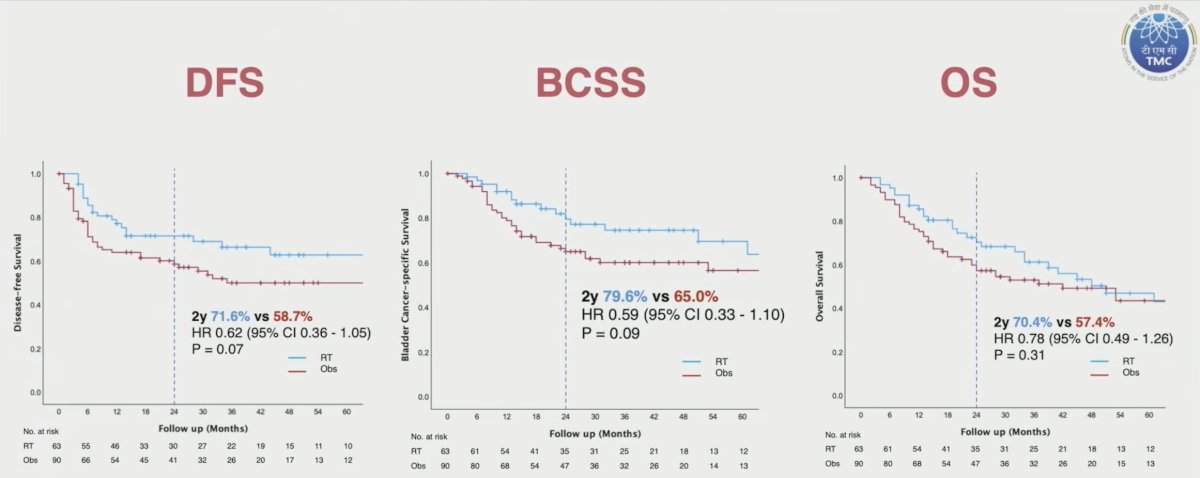
Two-year disease-free survival was 71.6% versus 58.7% (HR 0.62, 0.36-1.05, p = 0.07), bladder cancer-specific survival was 79.6% versus 65.0% (HR 0.59, 0.33-1.10, p = 0.09), and overall survival was 70.4% versus 57.4% (HR 0.78, 95% CI 0.49-1.26, p = 0.31), for adjuvant radiotherapy versus observation, respectively:
With regard to patterns of recurrence, there were no isolated locoregional recurrences with radiotherapy:
Dr. Murthy noted that at ASTRO 2024, he presented adverse effects of the BART trial (subsequently published in the Red Journal2), highlighting that grade 3 gastrointestinal adverse events were low: 4.1% in the observation arm versus 1.6% in the radiotherapy arm. However, Grade 2 gastrointestinal adverse events were higher in the radiotherapy arm (17.5% versus 1.4%), with no toxicity related discontinuation. Late grade 3+ toxicity was similar between the two arms: 8.4% for adjuvant radiotherapy versus 10.5% for observation, p = 0.60).
Dr. Murthy also highlighted a SWOT analysis of this trial:
- Strengths:
- The largest RCT in this disease space, multi-center
- Included standard of care surgery, chemotherapy, and radiotherapy
- Weaknesses:
- No immunotherapy
- Fell a bit short in the sample size goal
- Threats: “fear” of adjuvant radiotherapy among surgeons and radiation oncologists
- Opportunities:
- Radiotherapy + immunotherapy combinations (with non-overlapping toxicities)
- MERCY: an individual patient data meta analysis
Dr. Murthy concluded his presentation discussing clinical outcomes from the phase III BART multicenter randomized controlled trial with the following take home points:
- Adjuvant radiotherapy improved locoregional failure-free survival without increased severe late toxicity in patients with locally advanced muscle invasive bladder cancer post cystectomy and chemotherapy
- A potential benefit in overall survival is being explored in a planned individual patient data meta-analysis of randomized trial.
Presented by: Vedang Murthy, MD, Tata Memorial Centre, New Mumbai, Maharashtra, India
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 American Society for Radiation Oncology (ASTRO) Annual Meeting, San Francisco, CA, Sat, Sept 27 – Wed, Oct 1, 2025.
Related content: Adjuvant Radiotherapy Evaluated for High-Risk Bladder Cancer After Cystectomy - Vedang Murthy
References:
- Bajorin DF, Witjes JA, Gschwend JE, et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. 2021 Jun 3;384(22):2102-2114.
- Bladder Adjuvant Radiation Therapy (BART): Acute and Late Toxicity from a Phase III Multicenter Randomized Controlled Trial. Int J Radiat Oncol Biol Phys. 2025 Mar 1;121(3):728-736.