(UroToday.com) The 2023 ASTRO annual meeting included a session on oligometastatic prostate cancer, featuring a presentation by Dr. Shalini Moningi discussing prostate directed radiation in the oligometastatic setting. Dr. Moningi started her presentation by highlighting the following learning objectives for her presentation:
- Understand the role of prostate directed radiation therapy in oligometastatic prostate cancer
- Discuss SBRT for prostate cancer
- Understand the benefits of MR-Linac based prostate SBRT
- Discuss MR-Linac directed prostate SBRT in the low-volume oligometastatic setting
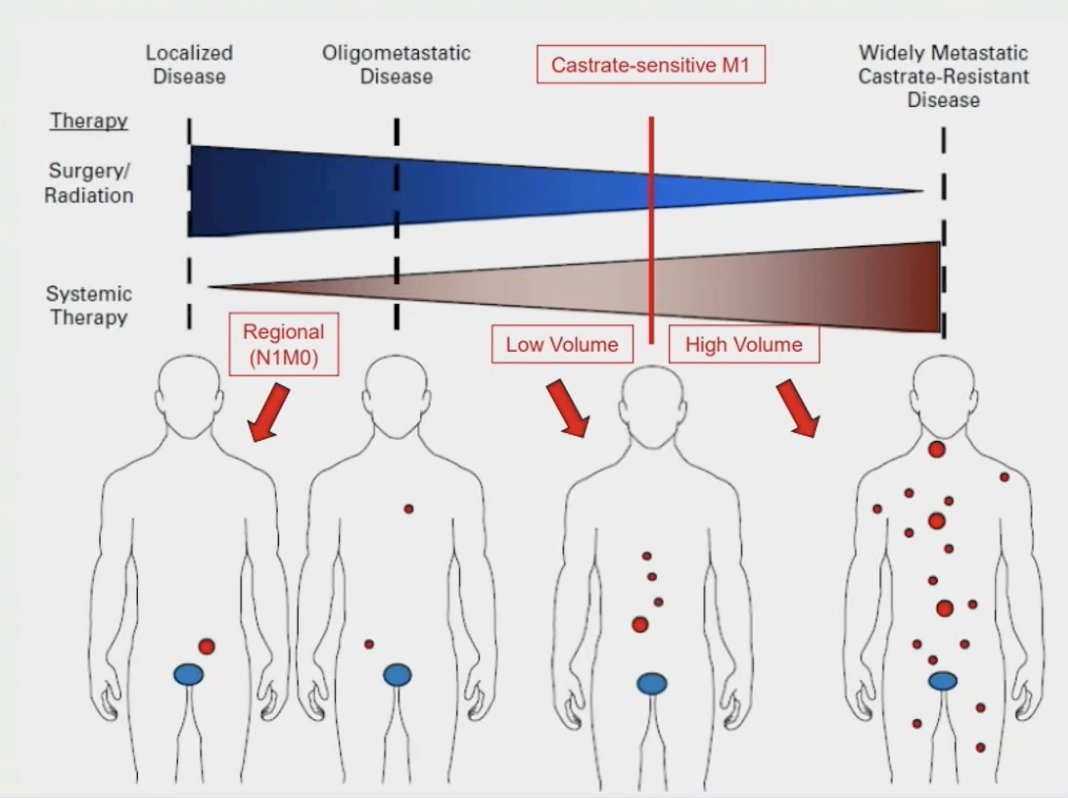
Prostate cancer has become a disease continuum highlighting the multidisciplinary treatment teams over the course of the disease:
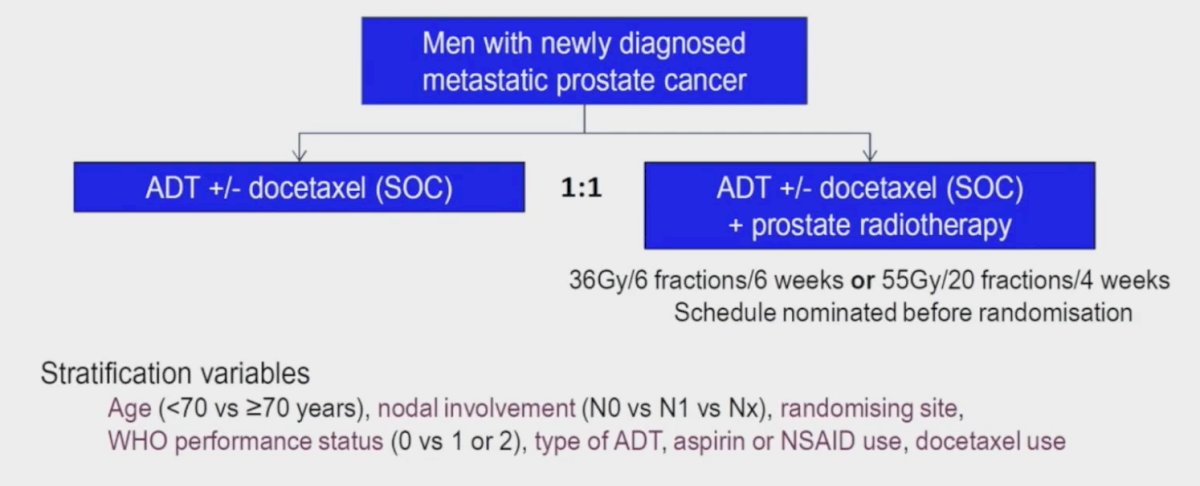
Reviewing the data for prostate directed radiotherapy for metastatic disease, Dr. Moningi started by discussing the STAMPEDE Arm H trial.1 This was an open label, randomized controlled phase III trial of 2,061 men at 117 hospitals across Switzerland and the UK. This arm randomized patients with de novo mHSPC in a 1:1 fashion to standard of care with or without radiotherapy between January 2013 and September 2016. Standard of care was lifelong androgen suppression with upfront docetaxel permitted from December 2015 onwards (18% of total cohort). Men allocated radiotherapy received either a daily (55 Gy in 20 fractions over 4 weeks) or weekly (36 Gy in six fractions over 6 weeks) schedule that was decided before randomization:
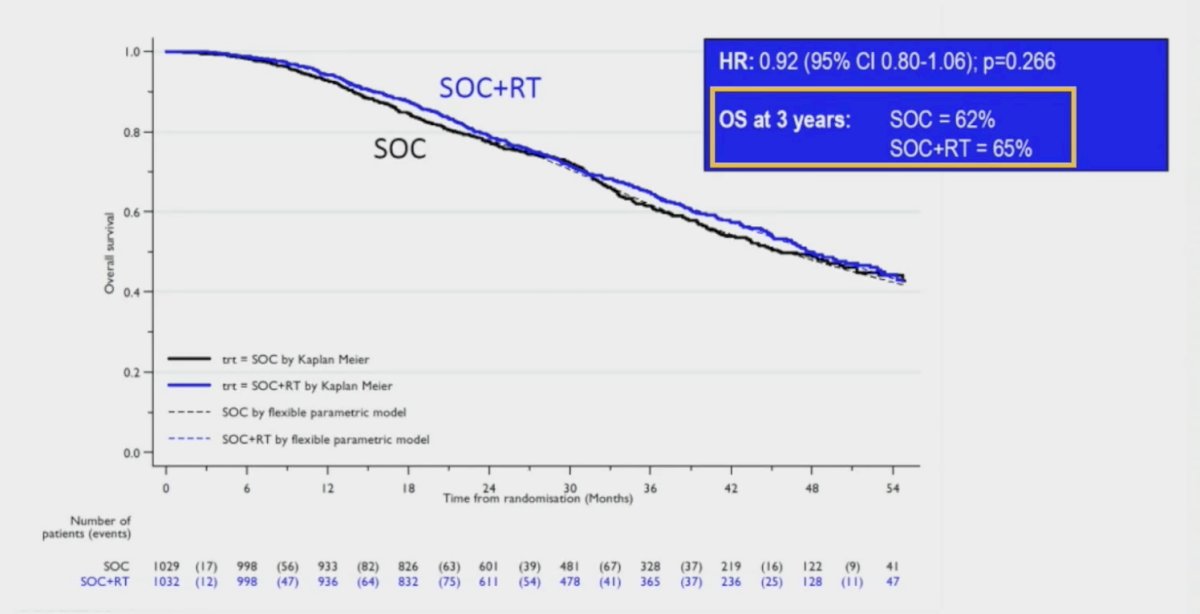
In this trial, the median PSA was 97 ng/ml and 54% had high metastatic burden compared to 40% with low metastatic burden (6% unknown). At a median follow up of 37 months, prostate radiotherapy improved failure-free survival (HR 0.76, 95% CI 0.68 – 0.84; p < 0.0001) but not overall survival (HR 0.92, 95% CI 0.80 – 1.06; p = 0.266) in the overall cohort:
However, when stratified by metastatic burden, overall survival benefits were seen in the low volume group (HR 0.68, 95% CI 0.52 - 0.90), but not in the high-volume population:

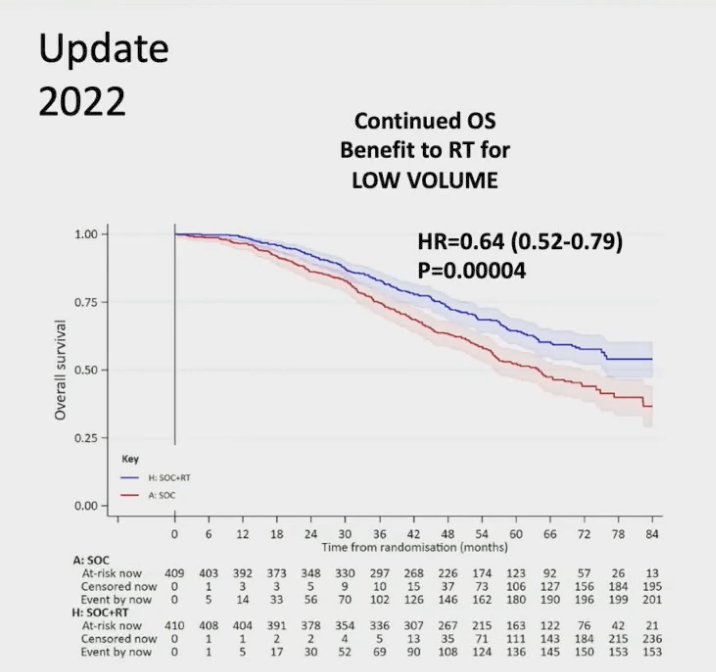
Updated results of this trial were published June 2022,2 and with a median follow up of 61.3 months, prostate radiotherapy continued to demonstrate overall survival benefits in patients with low metastatic burden (HR 0.64, 95% CI 0.52 - 0.79, p < 0.001), whereas there was still no benefit seen in patients with a high metastatic burden (HR 1.11, 95% CI 0.96 - 1.28, p = 0.164; interaction p = 0.001):
Transitioning to the HORRAD trial,3 this was a multicenter prospective trial of 432 patients with previously untreated, de novo mHSPC. All eligible patients had a PSA >20 ng/ml and documented bone metastases on bone scan. Patients were randomized 1:1 to either androgen suppression alone or with external beam radiotherapy. After a median follow up of 47 months, the primary outcome of overall survival was non-significantly different: median 45 months in the radiotherapy/ADT arm versus median 43 months in the ADT alone arm (HR 0.90, 95% CI 0.70 - 1.14, p = 0.40). However, subgroup analysis by number of metastatic lesions suggested a potential overall survival benefit for radiotherapy in patients with <5 metastatic sites (HR 0.68, 95% CI 0.42 - 1.10):

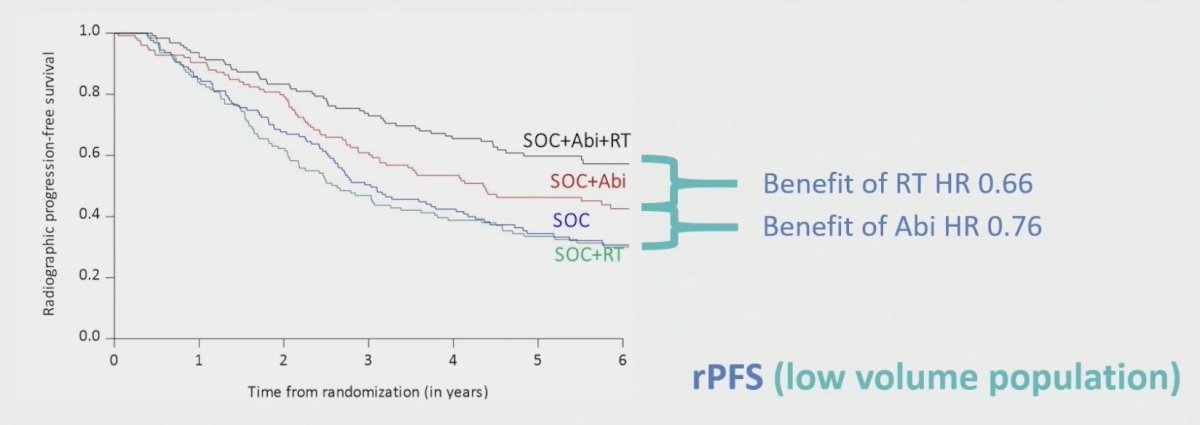
Dr. Moningi then discussed the PEACE-1 trial, which randomized patients 1:1:1:1 to ADT vs ADT + abiraterone vs ADT + local radiotherapy vs ADT + local radiotherapy + abiraterone. Of note, most patients received docetaxel as well after 2015. Presented at ASCO 2023, the results of the analysis of the efficacy and safety of prostate radiotherapy for patients with low volume, de novo mHSPC were discussed. Over a median follow-up of 73 months, for rPFS the addition of prostate radiotherapy to standard of care + abiraterone was associated with a significant rPFS benefit (median 7.5 versus 4.4 years, p = 0.02). Conversely, addition of radiotherapy to standard of care alone was not associated with rPFS benefits (median 2.6 versus 3.0 years; HR 1.11, 95% CI 0.67 – 1.84, p=0.61). Dr. Moningi notes that the magnitude of benefit of adding prostate radiation to standard of care + abiraterone was similar to the benefit of adding abiraterone to standard of care systemic therapy:
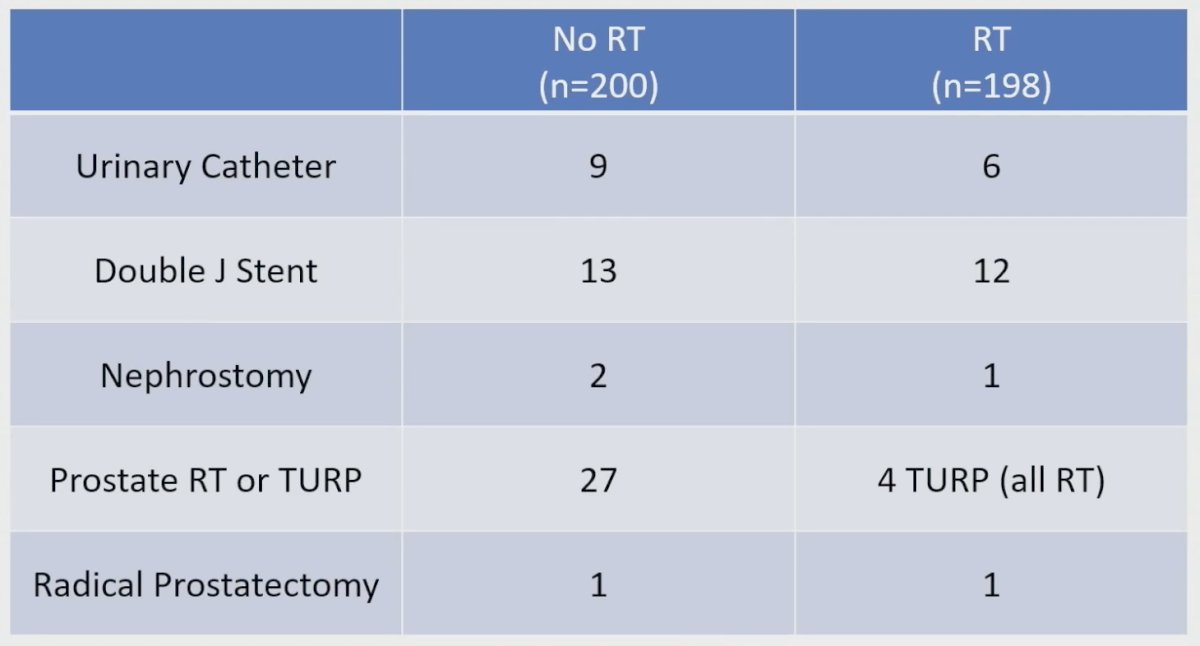
Furthermore, in PEACE-1 they also looked at serious genitourinary events, stratified by radiotherapy versus no radiotherapy, noting that patients receiving radiotherapy had fewer adverse events:
Dr. Moningi’s conclusions from PEACE-1 are as follows:
- Combining prostate radiotherapy with intensified treatment (abiraterone with or without docetaxel) improves radiographic progression free survival and CRPC-free survival in men with de-novo, low burden metastatic CSPC
- There was no detectable impact of prostate radiotherapy on overall survival, with minimal added toxicity
- For the first time, PEACE-1 also established a role of radiotherapy in the prevention of serious genitourinary events, irrespective of metastatic burden
- A triplet of ADT + abiraterone + prostate radiotherapy should be considered a standard in men with de novo low burden mCSPC (additive effect). Radiotherapy may also be considered in select men with de novo high burden mCSPC (“quadruplet”)
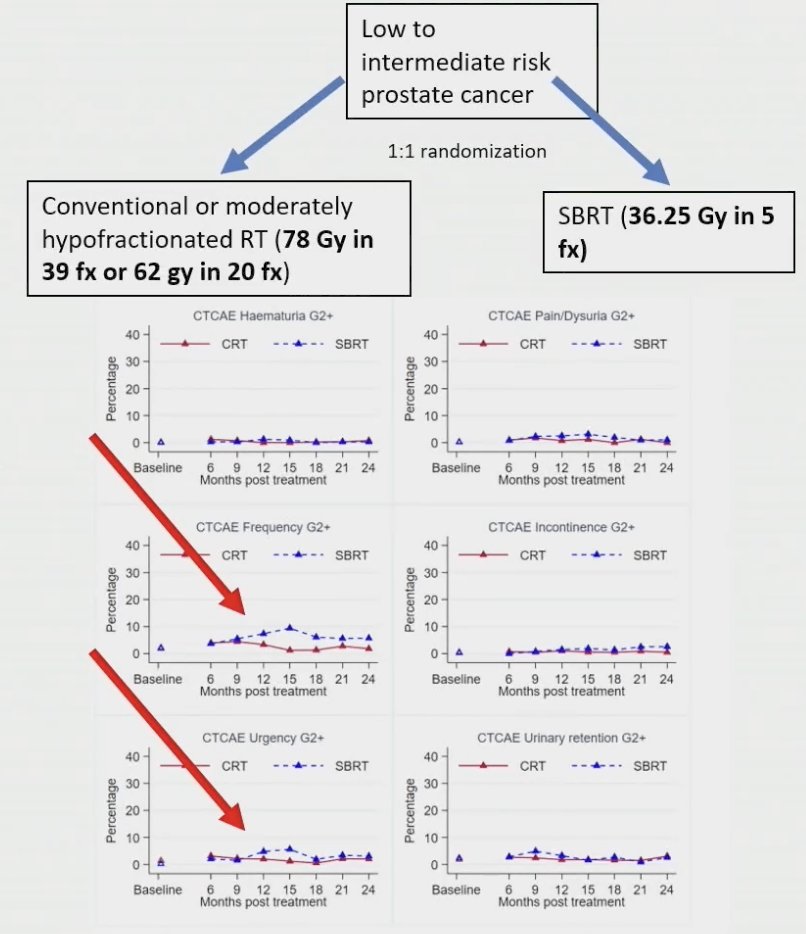
Dr. Moningi then discussed prostate SBRT focusing first on the PACE-B trial, which published 2-year toxicity outcomes in 2022.4 PACE-B was an international multicenter, phase III, open-label, randomized, non-inferiority trial that randomized men with low- or intermediate-risk prostate cancer (Grade Group 3 excluded) in a 1:1 fashion to either conventionally (78 Gy in 39 fractions over 7.8 weeks) or moderately hypofractionated radiotherapy (62 Gy in 20 fractions over 4 weeks) versus stereotactic body radiotherapy (36.25 Gy in five fractions over one to two weeks). There were 874 men randomized to conventional/moderate hypofractionation (n = 441) or stereotactic body radiotherapy (n = 433). Worst acute RTOG gastrointestinal toxic effects were as follows: grade 2 or more severe toxic effects in 12% of patients in the conventional/moderate hypofractionation arm versus 10% in the stereotactic body radiotherapy group (difference −1.9 percentage points, 95% CI: −6.2 to 2.4; p = 0.38). There were similarly no significant differences in worst acute RTOG genitourinary toxicity effects with grade 2 or worse toxicity noted in 27% and 23% of patients, respectively (difference −4.2 percentage points, 95% CI: −10.0 to 1.7; p = 0.16):
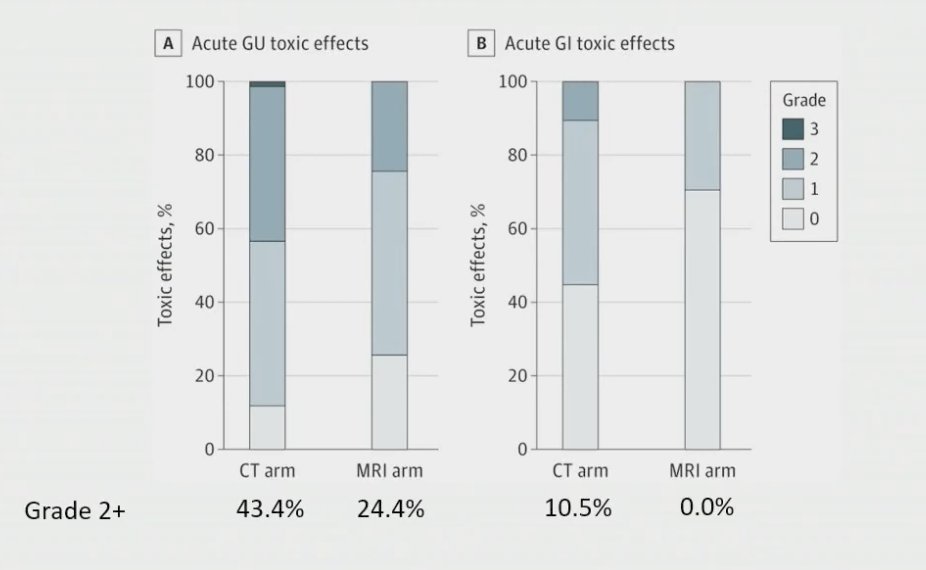
The MIRAGE trial sought to assess whether MRI-guided radiation can improve upon the toxicity profile of prostate SBRT.5 This trial randomized men 1:1 to CT-guided SBRT (4mm PTV margin) versus MRI-guided SBRT (2mm PTV margin) with a primary outcome of incidence of acute grade >=2 genitourinary toxicity. Importantly, this trial found that there were reduced acute G2+ genitourinary and gastrointestinal toxicity with MRI-guided SBRT as highlighted in the following figure:
Dr. Moningi then pivoted to discuss the importance of adaptive planning. The first reason this is important is because there can be seminal vesicle variation from the original plan to the day of treatment plan:

Secondly, is the consideration of prostate swelling, which typically develops after one fraction of prostate SBRT. This can be substantial given that there may be a median 5% increase in prostate volume by the third fraction with a range as broad as 0-56%. This would be unaccounted for without adaptive planning, which is a newly appreciated concern for non-adaptive prostate SBRT:
Third, adaptive planning is important for sparing the urethra, which is an important organ at risk for prostate SBRT. In fact, there is a 1% increase in G2+ late urinary toxicity for every 1 Gy increase dose to the urethra.
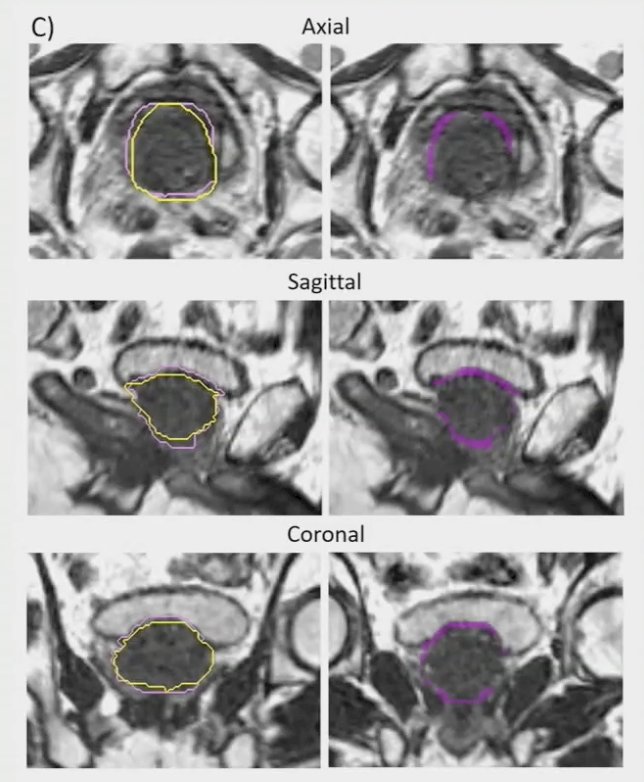
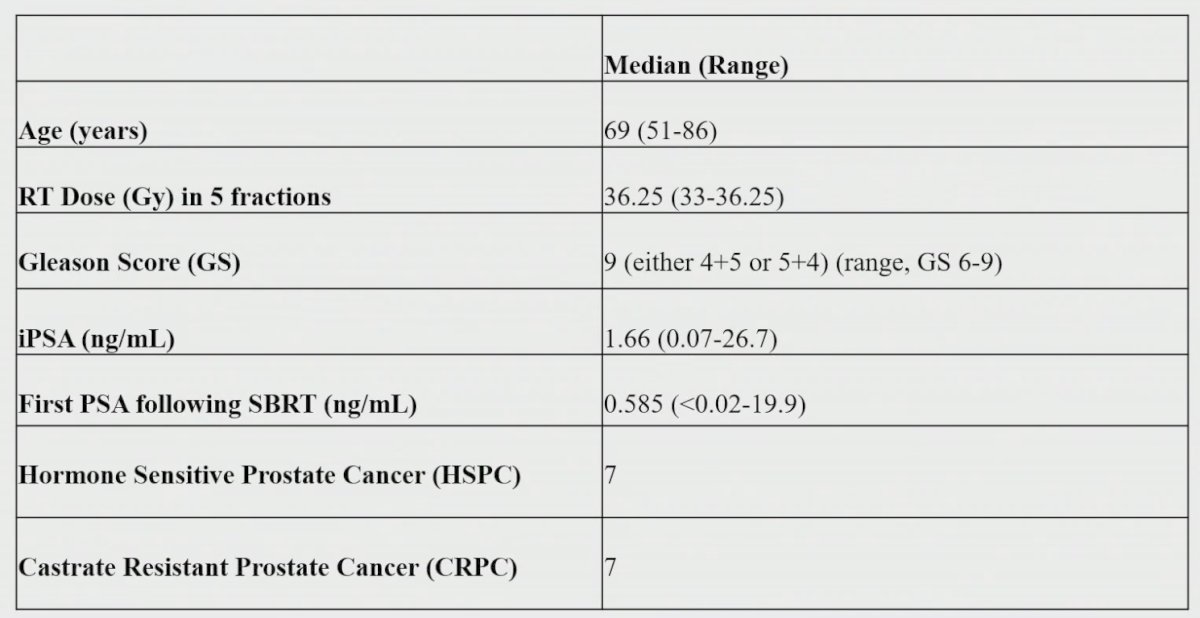
To conclude her presentation, Dr. Moningi discussed prostate SBRT in the oligometastatic setting. At her institution, she notes that they have experience using stereotactic MR guided adaptive prostate SBRT for patients with low volume metastatic disease. As such, they reviewed 14 consecutive patients with metastatic prostate cancer with low volume metastatic disease who received prostate SBRT from 2019 to 2021 on a 0.35T MR-Linac platform. Genitourinary and gastrointestinal toxicities were assessed using CTCAE v 5.0 and collected prospectively in this cohort of patients; post-treatment PSA response was also evaluated. As follows are the baseline characteristics:
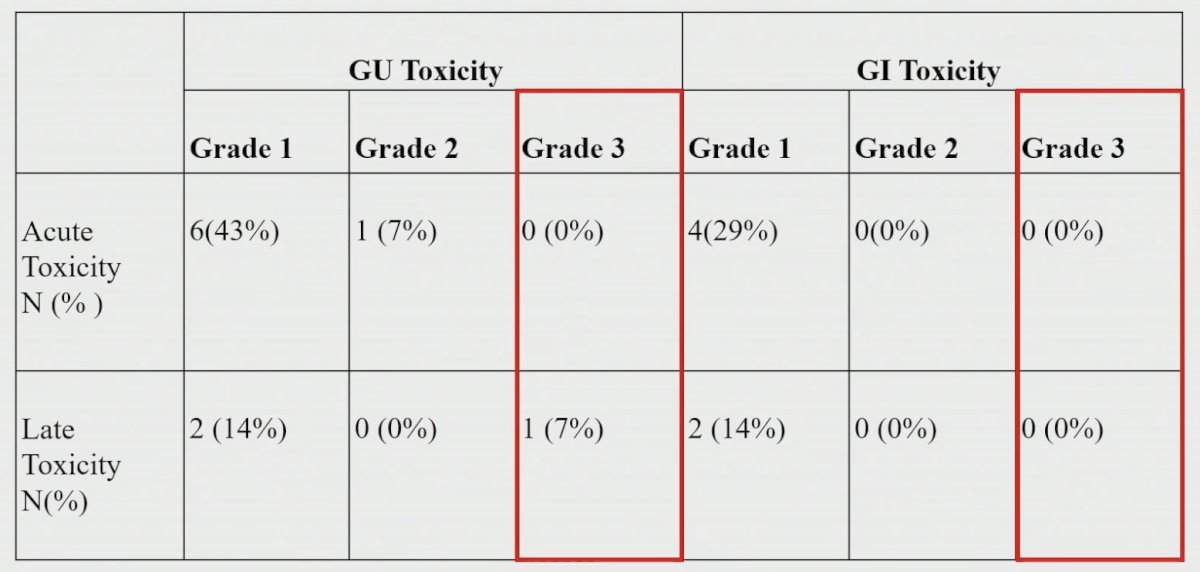
There was no G2 or G3 acute gastrointestinal toxicity with only one event of grade 2 acute genitourinary toxicity:
As follows are the PSA SBRT trends over time, stratified by castration sensitive versus resistant:
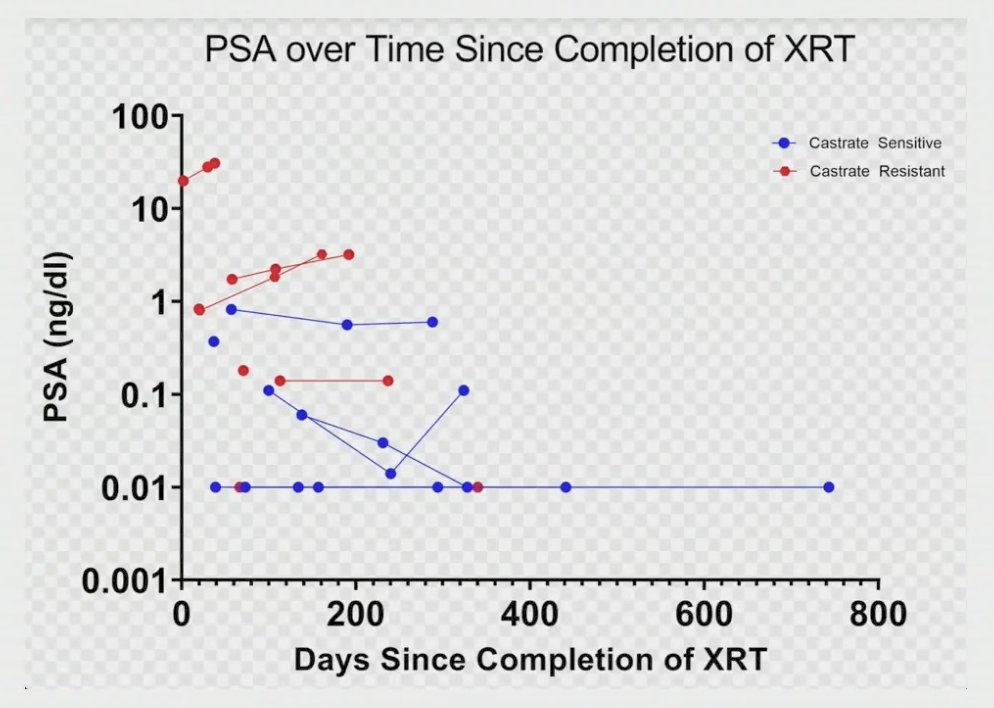
As such, Dr. Moningi notes that prostate SBRT was feasible in the metastatic prostate cancer population and was associated with low rates of acute genitourinary toxicity and no acute grade >= 2 gastrointestinal toxicity. Additionally, there were high rates of disease control among this cohort and no progression of local disease at last time of follow-up. Overall, prostate SBRT was well-tolerated, and these findings support its role as a low-risk approach for patients with limited metastatic disease.
Dr. Moningi concluded her presentation by discussing prostate directed radiation in the oligometastatic setting with the following take-home points:
- There is a significant role of radiotherapy in the low-volume oligometastatic setting
- Prostate SBRT is well tolerated and even better tolerated when using MR-Linac technology
- There is an emerging role of prostate SBRT for oligometastatic prostate cancer patients
Presented by: Shalini Moningi, MD, Brigham and Women's Hospital/Dana-Farber, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2023 American Society for Therapeutic Radiation Oncology (ASTRO) 65th Annual Meeting held in San Diego, CA between October 1st and 4th, 2023
References:
- Parker CC, James ND, Brawley CD, et al. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): A randomized controlled phase 3 trial. Lancet 2018 Dec 1;392(10162):2353-2366.
- Parker CC, James ND, Brawley CD, et al. Radiotherapy to the prostate for men with metastatic prostate cancer in the UK and Switzerland: Long-term results from the STAMPEDE randomised controlled trial. PLoS Medicine. 2022;19(6):e1003998.
- Boeve LMS, Hulshof MCCM, Vis AN, et al. Effect on Survival of Androgen Deprivation Therapy Alone Compared to Androgen Deprivation Therapy Combined with Concurrent Radiation Therapy to the Prostate in Patients with Primary Bone Metastatic Prostate Cancer in a Prospective Randomised Clinical Trial: Data from the HORRAD Trial. Eur Urol. 2019 Mar;75(3):410-418.
- Tree AC, Ostler P, van der Voet H, et al. Intensity-modulated radiotherapy versus stereotactic body radiotherapy for prostate cancer (PACE-B): 2-year toxicity results from an open-label, randomized, phase 3, non-inferiority trial. Lancet Oncol. 2022 Oct;23(10):1308-1320.
- Kishan AU, Ma TM, Lamb JM, et al. Magnetic resonance imaging-guided vs computed tomography-guided stereotactic body radiotherapy for prostate cancer: The MIRAGE randomized clinical trial. JAMA Oncol. 2023 Mar 1;9(3):365-373.