(UroToday.com) The 2023 ASTRO annual meeting included a session on novel prognostication techniques for prostate cancer, featuring a presentation by Dr. Alexander Sherry discussing multidimensional immunogenomic profiling of oligometastatic prostate cancer in the EXTEND trial.
Comprehensive metastasis-directed therapy for oligometastatic prostate cancer extended progression-free survival and time to new lesion formation in the intermittent hormone therapy basket of EXTEND.1 The EXTEND trial schema is as follows: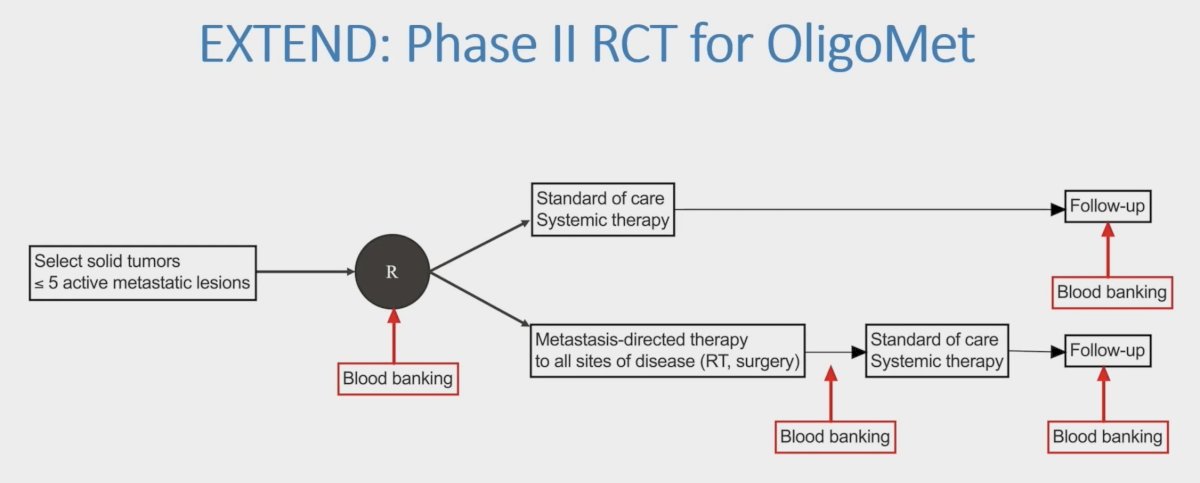
However, to better understand the mechanism of metastasis-directed therapy benefit, Dr. Sherry and colleagues pooled the intermittent and continuous hormone therapy baskets of EXTEND and tested the hypothesis that adding metastasis-directed therapy to hormone therapy would program systemic T-cells to control micrometastatic disease. This was based on the following observations:
- Comprehensive metastasis directed therapy facilitates diverse neoantigen exposure
- Comprehensive metastasis directed therapy eliminates macroscopic immunosuppressive stroma
- A preserved immune system of oligometastatic versus polymetastatic patients (chemotherapy exposure)
- Metastasis directed therapy + hormone therapy perhaps having synergy of immune effects
A total of 174 men were randomized to hormone therapy with or without metastasis-directed therapy to up to 5 sites of metastases. Hormone therapy was given for 6 months (intermittent basket, n=87) or indefinitely (continuous basket, n=87). Peripheral blood samples were drawn at enrollment, at the end of metastasis-directed therapy, at 3 months follow-up (3 month follow-up), and at progression and then analyzed by flow cytometry, T-cell receptor (TCR)-ß CDR3 variable region sequencing, multiplex cytokine profiling, and next-generation circulating tumor DNA (ctDNA) sequencing. TCR clonal expansion was determined using a published betabinomial model. Repertoire changes were assessed by Morisita’s index, and dominant TCR repertoire motifs were characterized with ImmunoMap. Associations between blood markers and progression-free survival were evaluated with Cox regression adjusted hazard ratios accounting for randomization arm and stratifying for intermittent vs continuous hormone therapy.
Randomization to metastasis-directed therapy + hormone therapy was associated with T-cell activation, proliferation, and clonal expansion: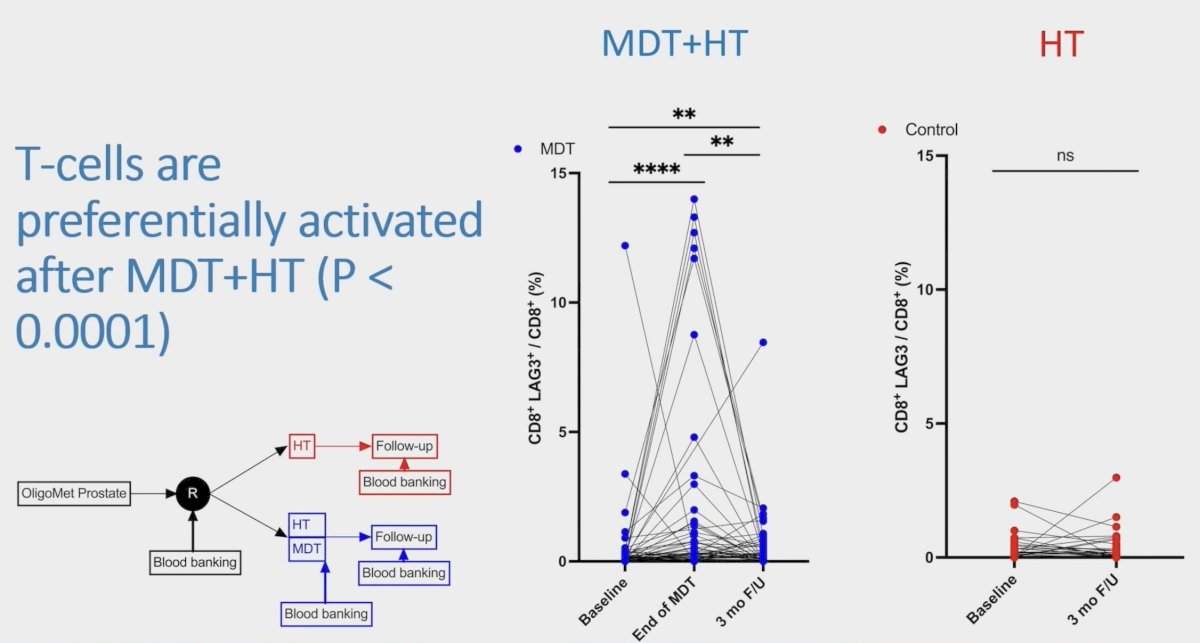
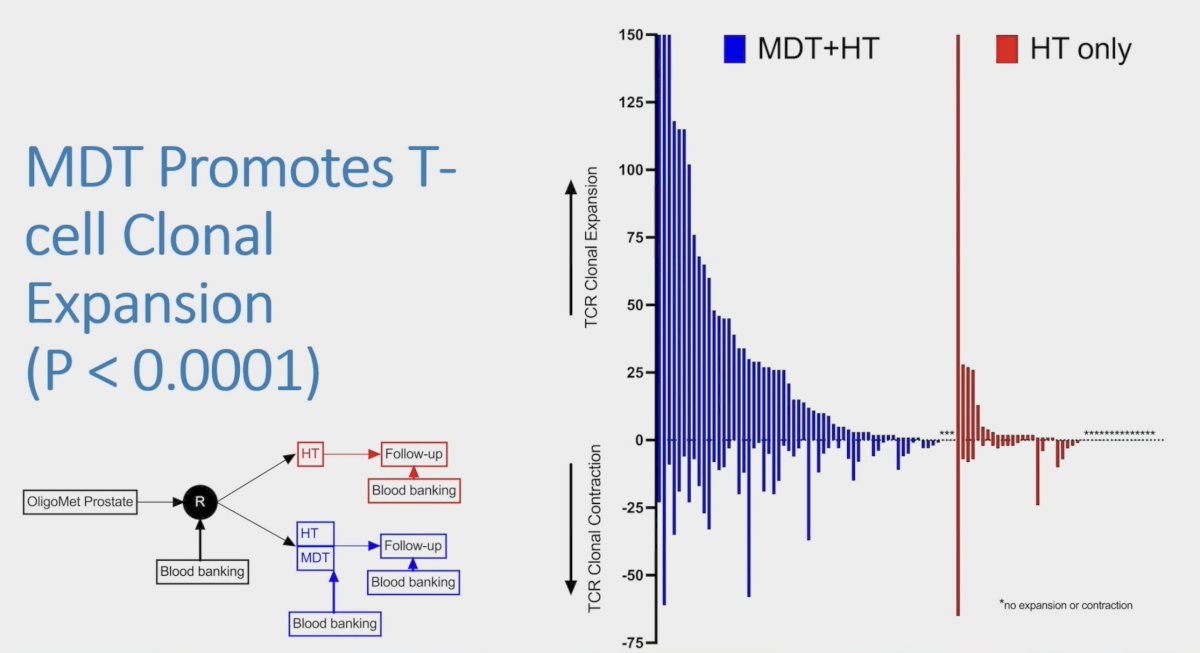
This response was first observed at end-metastasis-directed therapy as upregulated expression of T-cell activation and inhibition markers (i.e., ICOS, Tim-3, and LAG-3) and increases in highly proliferative CD4+ and CD8+ Ki67hi T-cells (all p < 0.05). TCR sequencing of 7,678,911 T-cells revealed that metastasis-directed therapy + hormone therapy was associated with TCR clonal expansion, remodeling of the TCR repertoire, and changes in dominant TCR motifs at end-metastasis-directed therapy and 3 mo F/U (all p < 0.05). Observed T-cell priming could be driven by signaling networks of canonical T-cell stimulatory cytokines (IL-2, IL-12, and IL-15), which were upregulated at end-metastasis-directed therapy and persisted at 3 month follow-up (all p < 0.05):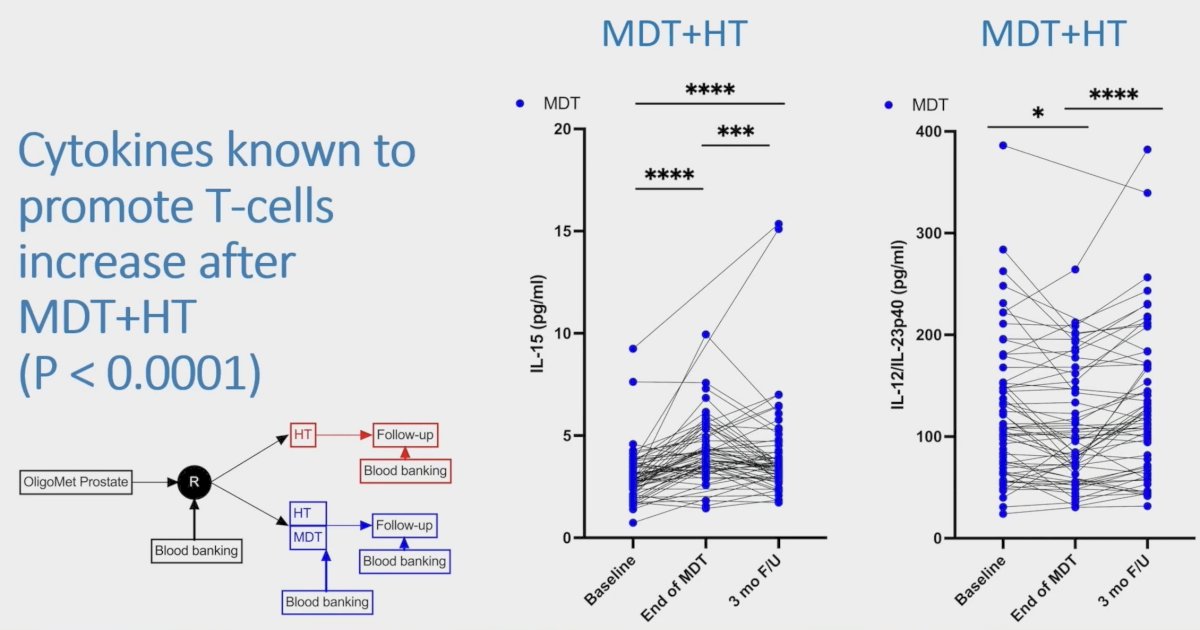
This modulation of T-cell phenotype, clonotype, and cytokine concentrations was not observed in the hormone therapy-monotherapy arm. At end-metastasis-directed therapy, systemic T-cell responses were associated with improved progression-free survival, most notably CD8+ T-cell expression of LAG-3 (aHR 0.24, 95% CI 0.07–0.72):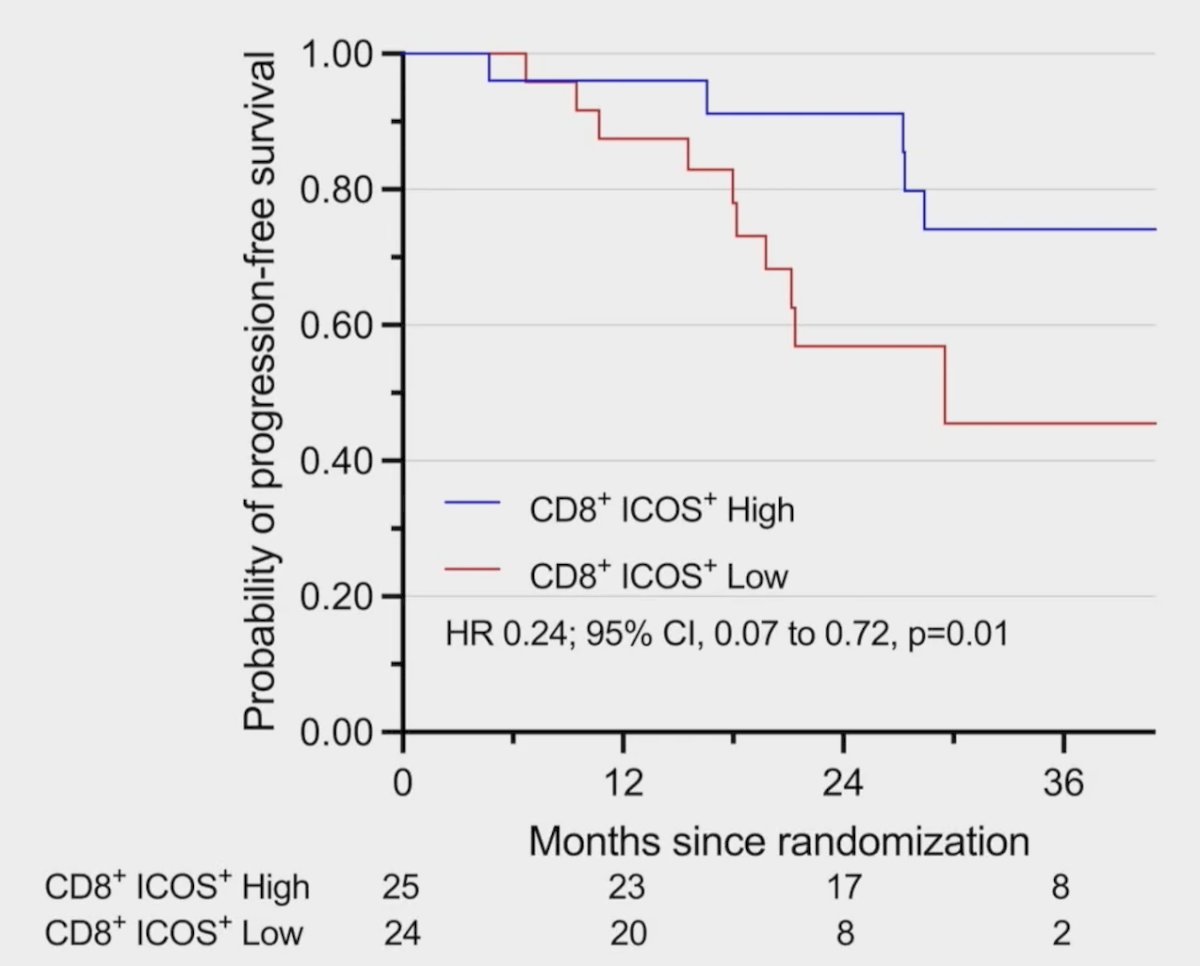
Additionally, rising IL-12/IL-23p40 versus stable/decreasing IL-12/IL-23p40 was associated with improved PFS (aHR 0.23, 95% CI 0.06-0.66): 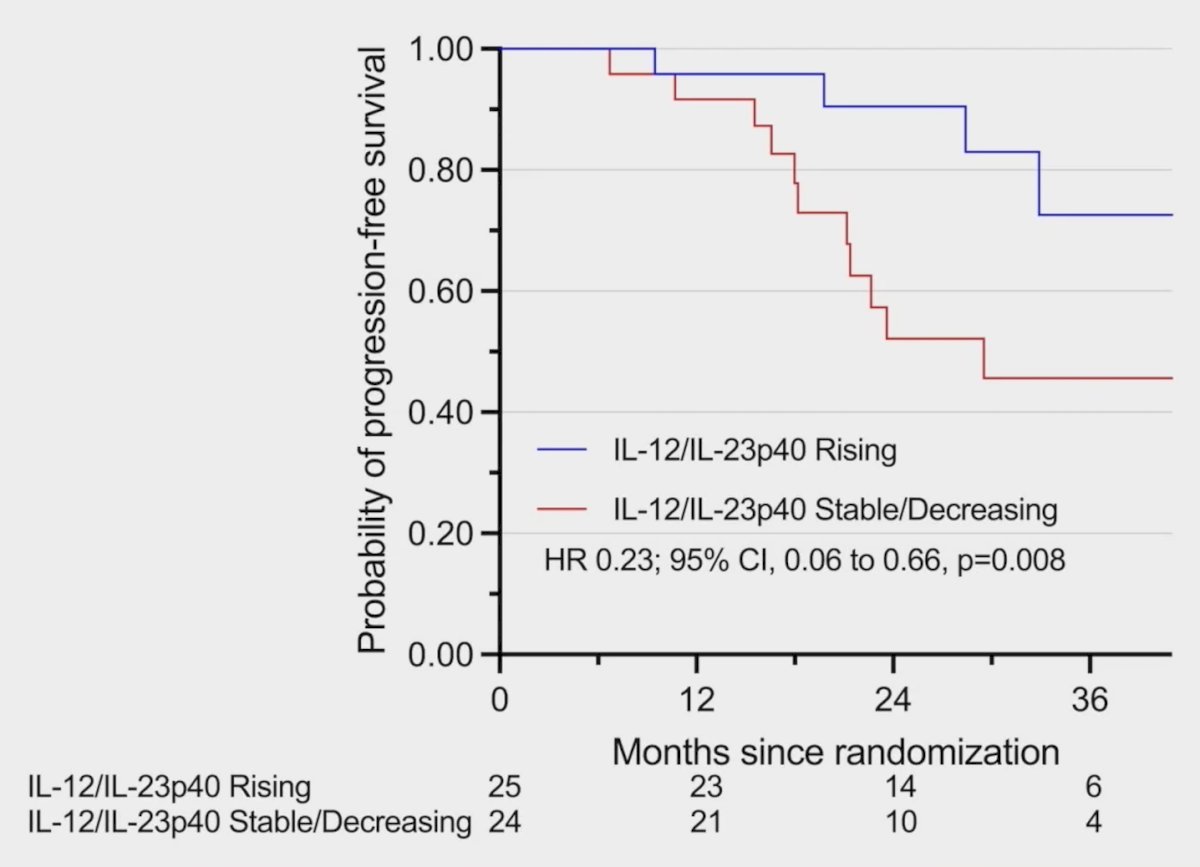
High ctDNA burden at end-metastasis-directed therapy correlated with worse progression-free survival (aHR 1.41, 95% CI 1.04–2.54), as did CD8+ T-cell expression of inhibitory receptor TIGIT at 3 month follow-up (aHR 1.03, 95% CI 1.01–1.06).
Dr. Sherry concluded his presentation discussing multidimensional immunogenomic profiling of oligometastatic prostate cancer in the EXTEND trial with the following take-home points:
- The addition of metastasis-directed therapy to hormone therapy induced systemic T-cell activation and expansion, which was not observed in the hormone therapy-only arm
- This systemic immune response was independently associated with improved progression-free survival
Presented by: Alexander Sherry, MD, University of Texas MD Anderson Cancer Center, Houston, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2023 American Society of Radiation Oncology (ASTRO) Annual Meeting, San Diego, CA, Sun, Oct 1 – Wed, Oct 4, 2023.
References: