(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026, was host to the Poster Session B: Prostate Cancer and Urothelial Carcinoma. Dr. Jeannie Hoffman-Censits presented the poster: ECOG ACRIN EA8291 Cohort C: A phase II trial of neoadjuvant gemcitabine/durvalumab in patients with high-grade upper tract urothelial carcinoma (UTUC) ineligible for cisplatin-based chemotherapy.
Dr. Hoffman-Censits began by noting that while neoadjuvant chemotherapy has increasing support in high-grade UTUC, the role of neoadjuvant chemoimmunotherapy remains less defined, particularly for cisplatin-ineligible patients, an area of clear unmet need.
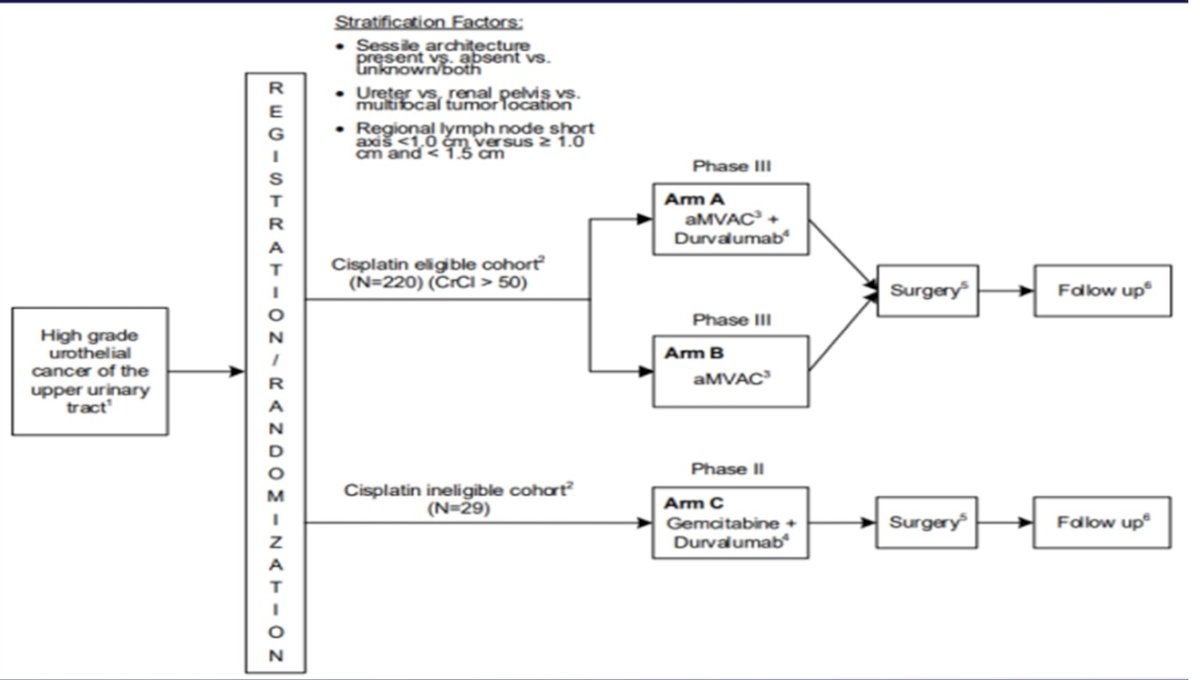
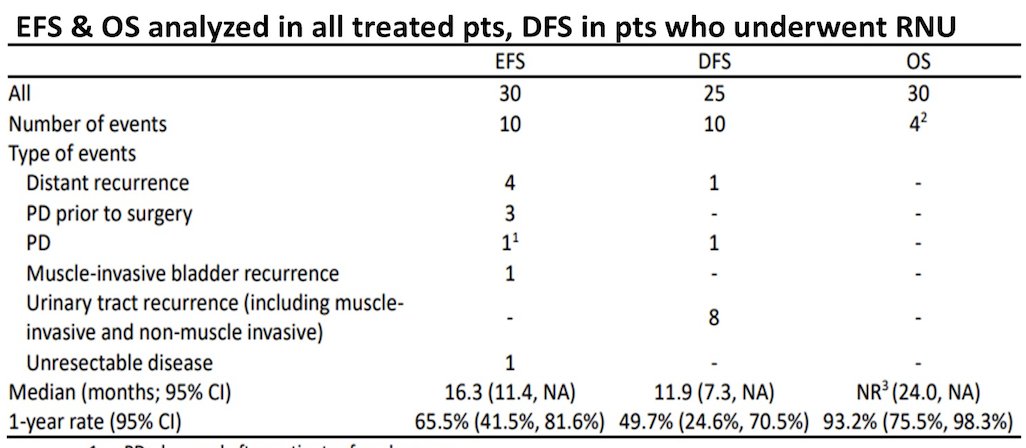
In this trial, cisplatin-ineligible patients with localized cN0 high-grade UTUC planned for radical nephroureterectomy were assigned to four cycles of gemcitabine plus durvalumab. The primary endpoint was pathologic complete response (ypT0N0/x), and Secondary endpoints included event-free and overall survival (EFS, OS).
Patients received planned neoadjuvant therapy consisting of four cycles of gemcitabine 1000 mg/m² on days 1 and 8 plus durvalumab administered intravenously on day 1 of each 21-day cycle. Nephroureterectomy with lymph node dissection was performed 21 to 60 days after the final dose of neoadjuvant therapy. The study design is shown below.
Between 2022 and 2025, 31 patients were enrolled. Thirty were eligible and received at least one dose of therapy; 23 completed all four planned cycles. Median age was 79 years, reflecting the older, cisplatin-ineligible population. Tumor location included renal pelvis (15 patients), ureter (15 patients), and one multifocal tumor. Five patients had a sessile appearance, and one unknown if sessile. Baseline characteristics are shown below.
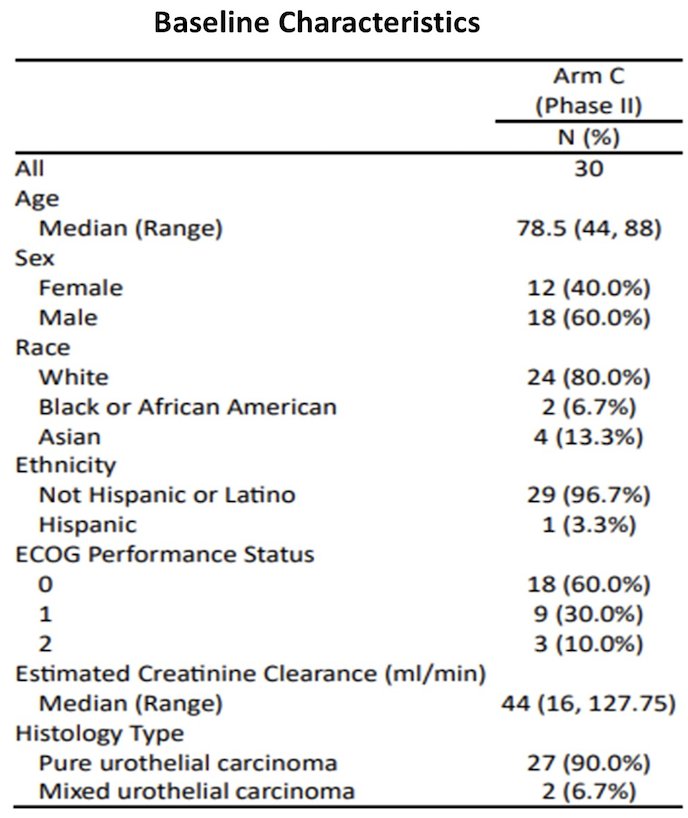
A total of 30 eligible patients received at least one dose of study therapy. Twenty-three completed all four planned cycles, and 14 required gemcitabine dose adjustments. All patients experienced treatment-related adverse events, with 13 experiencing grade 3–4 events. The most common grade 3–4 toxicities were anemia and neutropenia, each occurring in four patients. There were no grade 5 treatment-related adverse events, and no unexpected safety signals were observed overall.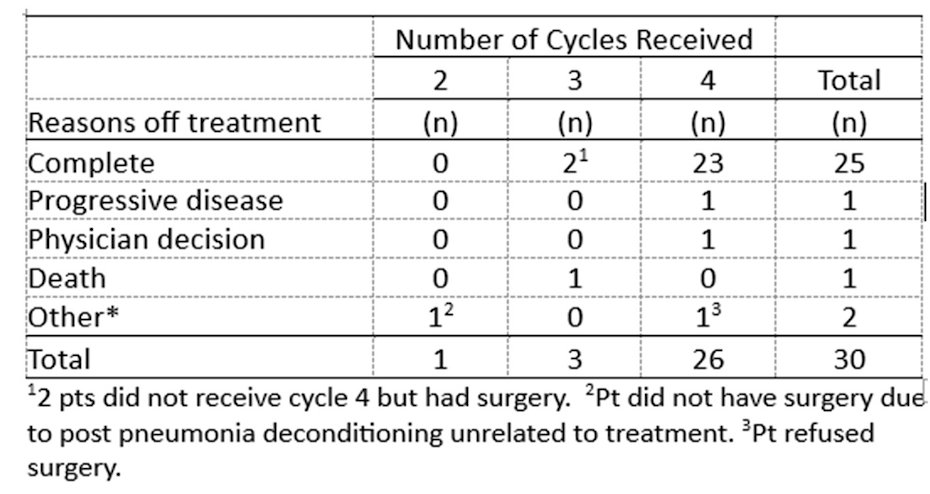
Three patients achieved a pathologic complete response, corresponding to a pCR rate of 10% (90% CI 3.0–25.2%). In addition, 10 patients (33%) were downstaged to less than ypT2N0/x. These results met the predefined threshold for success in this study design.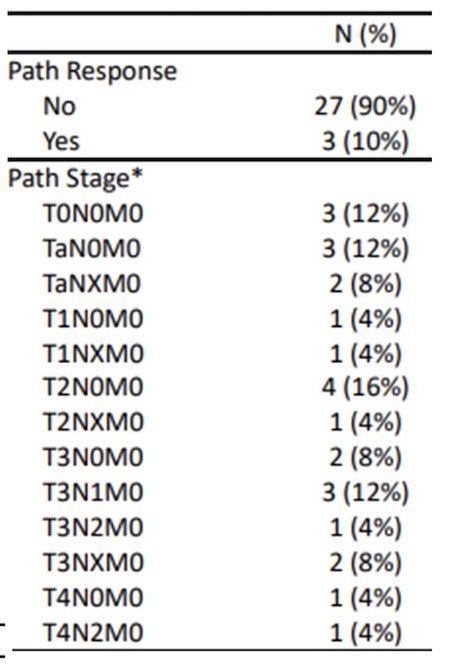
All treated patients experienced treatment-related adverse events. Grade 3–4 treatment-related events occurred in 13 patients, most commonly anemia and neutropenia (four patients each). There were no grade 5 treatment-related adverse events. Among those undergoing nephroureterectomy, the median time from the last neoadjuvant dose to surgery was 10 weeks. Five treated patients ultimately did not undergo surgery due to progression, unresectable disease, cancer-related death, refusal, or deconditioning.
With a median follow-up of 15.7 months, the estimated one-year event-free survival was 65.5% (95% CI 41.5%–81.6%).
Dr. Hoffman-Censits concluded with the following take-home messages:
- Neoadjuvant gemcitabine + durvalumab for high-grade UTUC was feasible and relatively well tolerated in this cohort.
- The pathologic complete response (ypT0N0/x) rate was 10% in the ITT population.
- A promising 1-year EFS rate was observed.
- Ongoing follow-up will further assess EFS, DFS, and OS, and planned biomarker analyses aim to better define predictors of response.
- Lymph node dissection remains a standard component of management in high-grade UTUC.
- aMVAC ± durvalumab is currently being evaluated in the ongoing phase III portion of this trial in cisplatin-eligible patients (NCT04628767).
Presented by: Jeannie Hoffman-Censits, MD, The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins, Johns Hopkins Greenberg Bladder Cancer Institute, Baltimore, MD
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.