(UroToday.com) The 2026 ASCO GU Annual Symposium featured a prostate cancer and urothelial carcinoma poster session. Dr. Harikrishnan Kunhiraman presented results from a PRISM-guided evaluation examining the implementability of cardiovascular risk scoring in oncology practice.
Cardiovascular disease remains the leading non-cancer cause of death among men with prostate cancer. Risk may increase during androgen deprivation therapy (ADT), highlighting the importance of cardiovascular risk assessment in this population. Although cardiovascular risk scores are well established in general medicine, their integration into oncology workflows remains limited. Importantly, barriers to implementing cardiovascular risk assessment within prostate cancer care have not been well characterized.
To address this gap, the investigators conducted a national cross-sectional survey of 45 U.S. physicians. Respondents represented multiple specialties involved in prostate cancer management, including medical oncology, urology, and radiation oncology. Participants spanned both academic and community practice settings and represented various career stages. Survey responses were mapped to the Practical, Robust Implementation and Sustainability Model (PRISM) and the RE-AIM (Reach, Effectiveness, Adoption, Implementation, Maintenance) frameworks to evaluate implementation feasibility.
Results demonstrated generally favorable perceptions of cardiovascular risk assessment tools, particularly when they are simple, rapid, and compatible with existing clinical workflows. Clinicians expressed a clear preference for lab-independent models to minimize disruption to clinical practice.
Across PRISM and RE-AIM implementation constructs, perceived effectiveness scored highest, with 87% of respondents indicating that cardiovascular risk tools would likely or very likely provide clinical utility. Equity in patient reach was also highly rated (75%), suggesting confidence that such tools could be broadly applied across diverse patient populations. Similarly, 73% of physicians believed these tools would perform consistently across clinical settings, and 71% reported high compatibility with existing workflows.
Cost and resource feasibility were viewed favorably by 65% of respondents, indicating that implementation may be feasible even in resource-limited settings. However, the perceived likelihood of adoption was somewhat lower at 60%, reflecting moderate readiness for implementation. Additional implementation challenges included equity in adoption (58%), reach to target populations (57%), and long-term sustainability (51%). Consistency of implementation scored lowest at 42%, highlighting the need for standardized protocols to support widespread integration.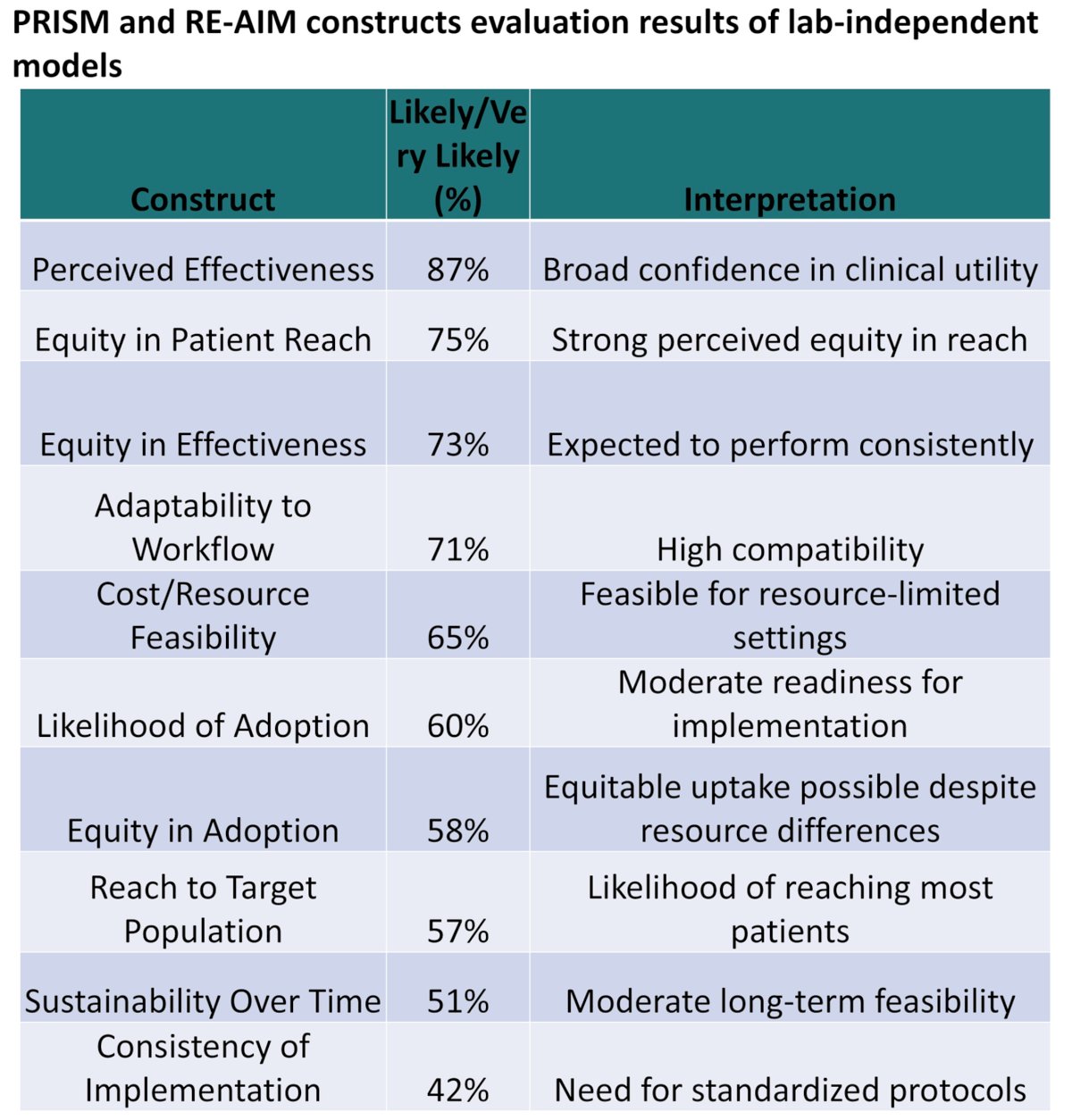
Taken together, these findings suggest that clinicians value cardiovascular risk assessment tools that are simple, fast, and workflow-compatible. Lab-independent models may be particularly attractive for clinical implementation because they minimize disruption to routine practice.
Presented by: Harikrishnan Hyma Kunhiraman, MBBS, Research Associate, Department of Medicine, Augusta University, Augusta, GA, USA