(UroToday.com) The 2026 ASCO GU Annual Symposium was host to a trials-in-progress prostate cancer poster session. Dr. Umang Swami presented OPTIMAS, an ongoing randomized, decentralized, de-escalation phase II trial in patients with metastatic hormone-sensitive prostate cancer (mHSPC) achieving an optimal PSA response.
An optimal PSA response, defined as ≤0.2 ng/mL, is achieved by approximately 51% of mHSPC patients 6–8 months after treatment with androgen deprivation therapy (ADT) and androgen receptor pathway inhibitors (ARPIs) ± docetaxel and is associated with a 61% reduction in risk of death (HR 0.39, 95% CI 0.30–0.50).¹
Patients receiving continuous ADT experience numerous adverse effects, including fatigue, loss of bone density, muscle loss, weight gain, gynecomastia, hot flashes, sexual dysfunction, increased cardiovascular risk, and skeletal-related events.
Since achieving optimal PSA response is prognostic of prolonged overall survival, these patients may be candidates for a de-intensified treatment strategy, which may result in better quality of life. To investigate this, Dr. Swami and colleagues initiated a de-intensification trial in patients with mHSPC.
OPTIMAS is an IRB-approved, investigator-initiated, single-center, multi-cohort, phase II, randomized, open-label study that will enroll 160 patients across two cohorts. The study schema is structured into two sequential steps for Cohort A and a separate intermittent-treatment cohort (Cohort B).
Cohort AStep 1: Study Registration
Eligibility includes:
- Diagnosis of mHSPC without small cell histology
- Never received ADT for mHSPC
Patients receive continuous relugolix + ARPI ± standard of care prostate cancer treatment.
Step 2: Randomization
Patients who achieve PSA ≤0.2 ng/mL after 6–12 months of relugolix + ARPI are randomized 1:1 to:
- Continuous treatment with ADT/relugolix + ARPI
- Intermittent treatment with relugolix + ARPI (treatment reinitiation per protocol criteria; treatment held if PSA ≤0.2 ng/mL)
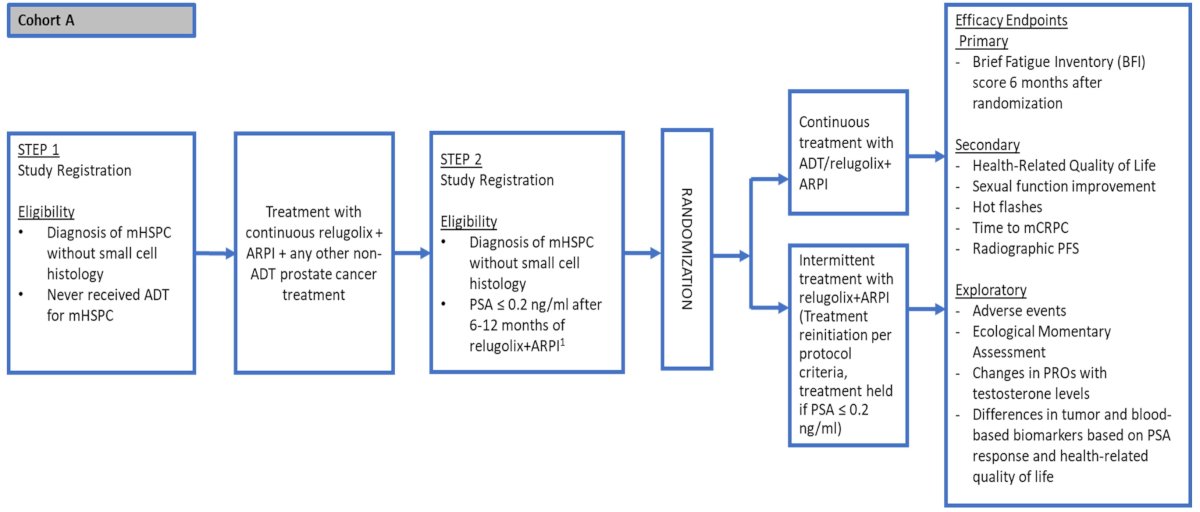
- Primary Endpoint: Difference in fatigue at 6 months after randomization between intermittent vs continuous arms (Brief Fatigue Inventory [BFI] score)
- Secondary endpoints:
- Health-related quality of life
- Sexual function improvement
- Hot flashes
- Time to mCRPC
- Radiographic PFS
- Sample size determination was based on prior data in mHSPC patients treated with ADT + ARPI, where the mean baseline worst fatigue (BFI3) score was 2.04 with SD 2.176.
- Null hypothesis: no difference in mean BFI3 between continuous vs intermittent arms at 6 months.
- Alternative hypothesis: ≥2-point difference.
- With 52 randomized patients (26 per arm), the study provides 90% power at one-sided 2.5% significance using a two-sample t-test assuming equal variance.
- With 100 patients enrolled in Step 1 and 60% expected to achieve PSA ≤0.2 ng/mL, approximately 58 evaluable patients will be randomized (dropout <10%).
- This design ensures that only biologically selected optimal responders undergo de-escalation testing.
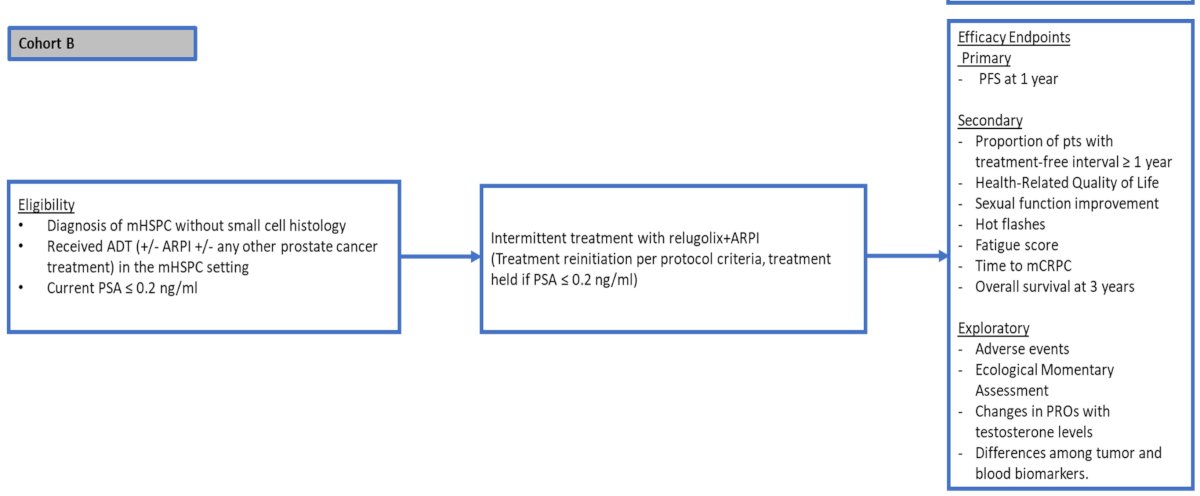
Cohort B will enroll 60 patients with mHSPC who initiated ADT for metastatic disease and achieved PSA ≤0.2 ng/mL. These patients are planned to receive intermittent relugolix + ARPI.
The primary endpoint of Cohort B is progression-free survival at 1 year. Assuming a 1-year PFS rate of 92%, the Clopper–Pearson exact method with 60 patients provides 95% confidence that the true PFS rate is no lower than 83.3%.
Secondary endpoints are as follows:
- Proportion of patients with a treatment-free interval ≥1 year
- Health-related quality of life
- Sexual function improvement
- Hot flashes
- Fatigue score
- Time to mCRPC
- Overall survival at 3 years
Exploratory endpoints are as follows:
- Adverse events
- Ecological momentary assessments
- Changes in PROs with testosterone levels
- Differences between tumor and blood biomarkers
Deep PSA responses in mHSPC are strongly prognostic.¹ Continuous therapy improves survival but at the cost of a significant toxicity burden.
OPTIMAS tests whether patients achieving optimal PSA response (≤0.2 ng/mL) can safely undergo intermittent therapy without compromising disease control while improving fatigue and quality of life.
The trial is notable for:
- Biologic selection based on PSA nadir
- Randomized comparison of intermittent vs continuous therapy
- Use of relugolix as an oral ADT backbone
- Integration of patient-reported outcomes and ecological momentary assessment
- Parallel cohort evaluating single-arm intermittent feasibility
This represents one of the first modern ARPI-era de-escalation studies in mHSPC incorporating both PRO-focused and survival endpoints.
Presented by: Umang Swami, MD, MS, Associate Professor, Division of Oncology, Department of Internal Medicine, Huntsman Cancer Institute at the University of Utah, Salt Lake City, UT
References:
- Nagai SAA, Riaz IB, Imran M, et al. Association of deep prostate-specific antigen response with survival outcomes in metastatic hormone-sensitive prostate cancer treated with androgen receptor pathway inhibitors. J Clin Oncol. 2023;41.
- Agarwal N, McQuarrie K, Bjarte L, et al. Deep PSA responses and long-term outcomes in metastatic hormone-sensitive prostate cancer. Lancet Oncol. 2019;20:1518-1530.