(UroToday.com) The 2026 ASCO GU Annual Symposium was host to a trials-in-progress prostate cancer poster session. Dr. Evan Yu presented OMAHA-003, an ongoing phase III trial of opevesostat, a CYP11A1 inhibitor, versus an androgen receptor pathway inhibitor (ARPI) switch in ARPI and taxane chemotherapy pre-treated metastatic castrate-resistant prostate cancer (mCRPC) patients.
Prostate cancer can remain dependent on androgen signaling even after progression on AR-directed therapies.1 Somatic activating point mutations in the AR ligand-binding domain (AR-LBD) are a common mechanism of resistance to AR-directed therapies in mCRPC.2-4
Opevesostat (MK-5684; ODM-208) is a nonsteroidal inhibitor of cytochrome P450 11A1 (CYP11A1), which catalyzes the first and rate-limiting step of steroid biosynthesis from cholesterol.5,6 Inhibition of CYP11A1 by opevesostat suppresses the production of all steroid hormones and precursors that may promiscuously activate the AR signaling pathway.
In the phase 1/2 CYPIDES trial, opevesostat demonstrated antitumor activity in participants with heavily pretreated mCRPC, particularly in the subset with AR-LBD mutations.1 The randomized, open-label, phase 3 OMAHA-003 trial (NCT06136624) will evaluate the efficacy and safety of opevesostat versus ARPI switch in participants with molecularly unselected mCRPC previously treated with ARPI and taxane-based chemotherapy
Randomization is stratified by:
• Presence versus absence of measurable disease
• Detection of AR-LBD mutations in circulating tumor DNA
• Prior receipt of cabazitaxel
Eligible participants are randomized to:
- Arm 1: Opevesostat 5 mg PO BID + Fludrocortisone 0.1 mg QD
- Arm 2 (ARPI switch): Abiraterone acetate 1000 mg QD + prednisone 5 mg BID or enzalutamide 160 mg QD
Treatment continues until radiographic progression, unacceptable toxicity, or withdrawal of consent. Upon progression, participants may receive post-treatment follow-up.

The key eligibility criteria are as follows:
Inclusion
- Age ≥18 years
- Histologically or cytologically confirmed adenocarcinoma of the prostate
- Disease progression after prior ARPI and 1–2 taxane-based chemotherapy regimens for mCRPC
- Participants previously treated with PARP inhibitors are allowed.
- Ongoing ADT or prior orchiectomy (testosterone <50 ng/dL)
- ECOG PS 0–1
Exclusion
- Known hypersensitivity to study components
- Significant active cardiovascular or cerebrovascular disease
- Clinically significant arrhythmias
- Active CNS metastases
- Prior treatment with CYP11A1 inhibitors
- Prior treatment with 177Lu-PSMA-617 is permitted
The primary objective is to evaluate overall survival (OS) for opevesostat versus abiraterone acetate or enzalutamide in participants with AR-LBD mutation–positive and –negative mCRPC, separately.
The secondary outcomes are as follows:
- Radiographic progression-free survival (rPFS) per PCWG3-modified RECIST v1.1 (BICR)
- Time to first subsequent therapy (TFST)
- Objective response rate (ORR) and duration of response (DOR)
- Time to pain progression (TTPP)
- Time to PSA progression
- Time to first symptomatic skeletal-related event (SSE)
- Safety and tolerability
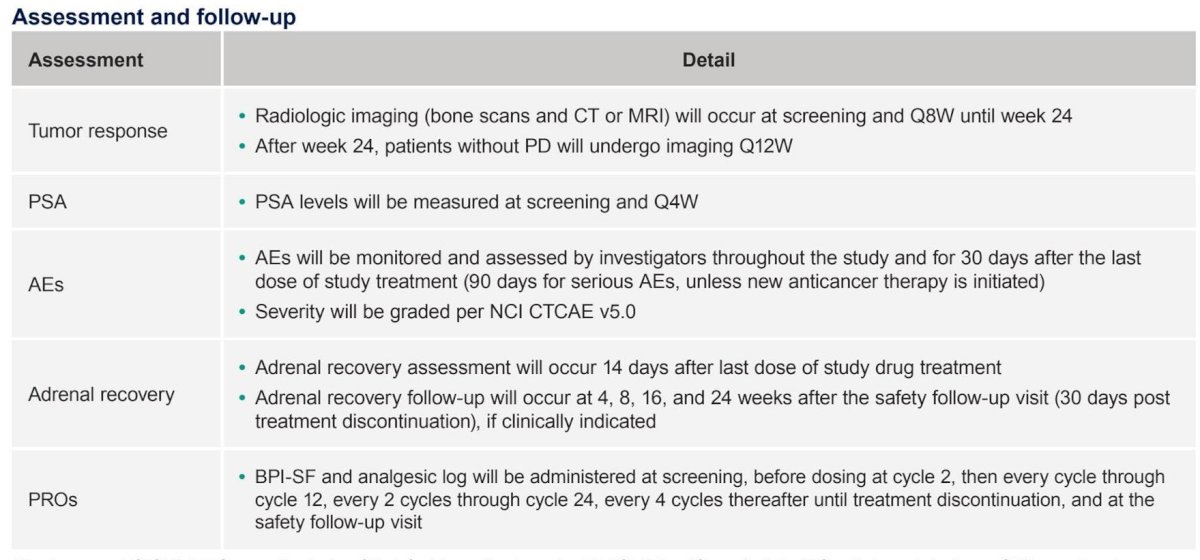
Planned assessments and follow-up are as detailed below:
The statistical analysis plan is as follows: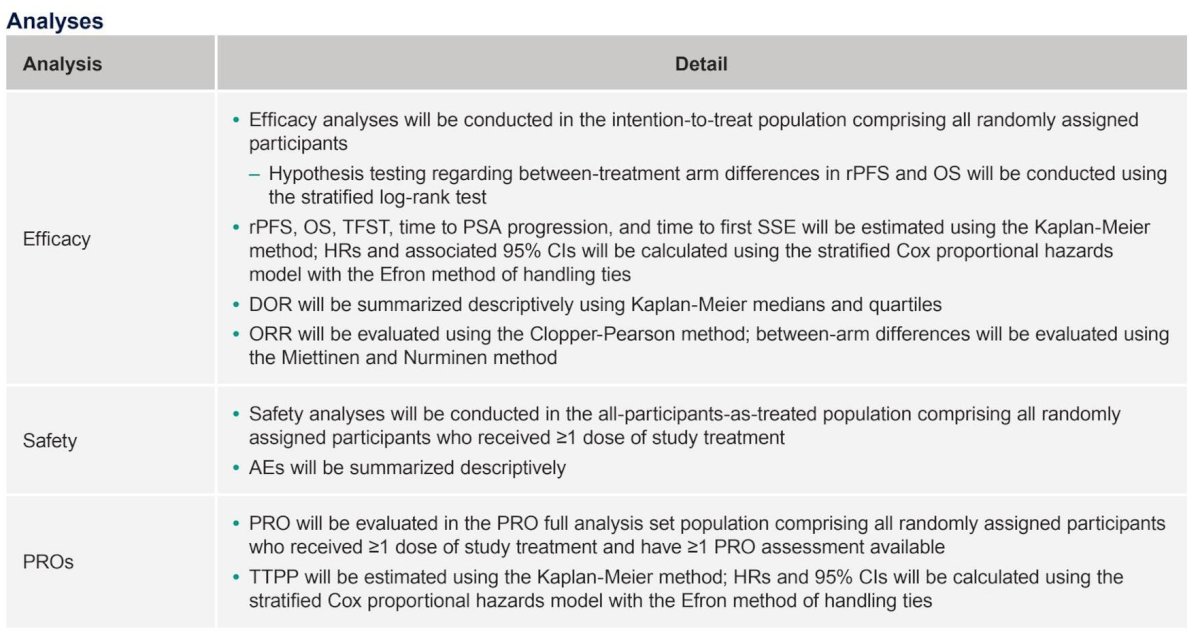
OMAHA-003 is actively enrolling globally, with participating sites across North America, South America, Europe, Asia, and Australia.
Presented by: Evan Yu, MD, Professor of Medicine, Division of Oncology, University of Washington School of Medicine, Section Head of Cancer Medicine, Medical Director of Clinical Research Support, Fred Hutchinson Cancer Center, The University of Washington School of Medicine, Seattle, WA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 ASCO GU Annual Symposium, San Francisco, CA, February 26th–28th, 2026Related content: OMAHA-003 Trial Explores CYP11A1 Inhibition in Metastatic Castration-Resistant Prostate Cancer - Evan Yu
- Fizazi K, Smith MR, Tombal B, et al. Efficacy and safety of CYP11A1 inhibition with opevesostat in metastatic castration-resistant prostate cancer: results from the CYPIDES study. NEJM Evid. 2024;3:EVIDoa2300171.
- Tan MH, Li J, Xu HE, Melcher K, Yong EL. Androgen receptor: structure, role in prostate cancer and drug discovery. Acta Pharmacol Sin. 2015;36:3-23.
- Bernard-Tessier A, Asselah J, Baciarello G, et al. Clinical activity of CYP11A1 inhibition in molecularly selected metastatic castration-resistant prostate cancer. J Clin Oncol. 2022;40(16_suppl):Abstract 5057.
- Yehya A, Ali M, Ibrahim M, et al. Mechanisms of resistance to androgen receptor–targeted therapies in metastatic castration-resistant prostate cancer. Cancer Drug Resist. 2022;5:667-690.
- Neunzig J, Bernhardt R, et al. Inhibition of CYP11A1 as a strategy to suppress steroid hormone biosynthesis in prostate cancer. PLoS One. 2014;9:e89727.
- McCarty KD, Smith R, Johnson T, et al. Structural and biochemical characterization of CYP11A1 inhibition and its impact on steroidogenesis. J Biol Chem. 2024;300:105495.