(UroToday.com) The 2026 GU ASCO annual meeting featured a prostate cancer session and a discussant presentation by Dr. Evan Yu, discussing two abstracts, “Final overall survival results from the EORTC 1333/PEACE-3 trial: Enzalutamide with or without radium-223 in metastatic castration-resistant prostate cancer” by Dr. Enrique Gallardo, and “Overall survival from the phase 2 trial of abiraterone, olaparib, or abiraterone + olaparib in first-line metastatic castration resistant prostate cancer (mCRPC) with DNA repair defects (BRCAAway)” by Dr. Maha Hussain.
Dr. Yu started his presentation by emphasizing what the data actually says. For the EORTC-1333 PEACE-3 trial, the final overall analysis confirms a 5.6-month median overall survival benefit of enzalutamide + radium-223 (38.2 months) over enzalutamide alone (32.6 months) for an HR of 0.75 (95% CI 0.60-0.95; one-sided stratified log rank p-value = 0.0078) for patients with asymptomatic/mildly symptomatic bone mCRPC. The BRCAAway trial reports median overall survival for combination abiraterone/olaparib (68 months) compared with abiraterone (28 months), with a HR of 0.39 (95% CI 0.16-0.93), and compared with olaparib (37 months), with a HR of 0.51 (95% CI 0.22-1.18) for patients with BRCA1/2 or ATM alterations receiving treatment for first line mCRPC.
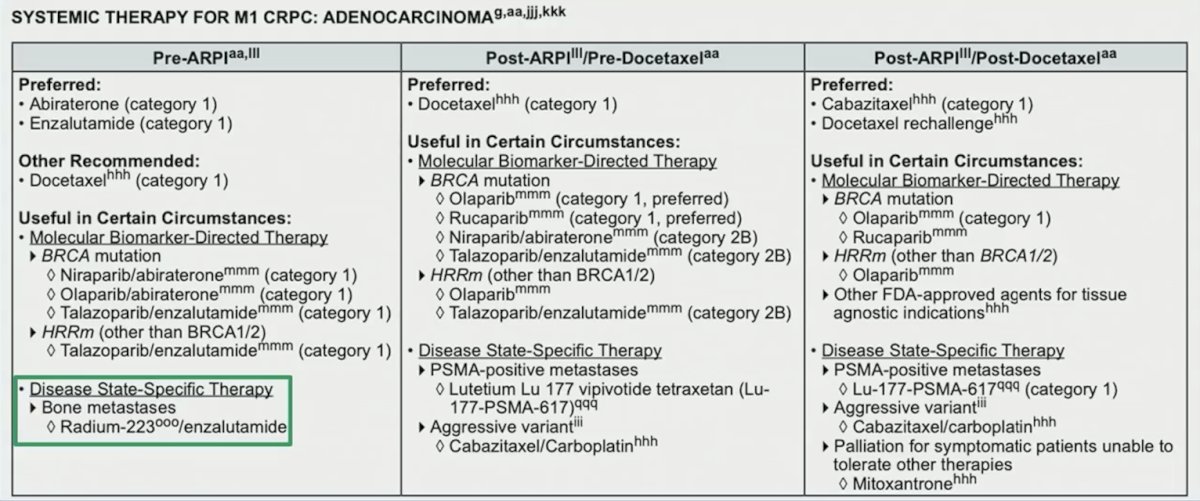
Discussing the EORTC-1333 PEACE-3 trial, Dr. Yu notes that this regimen of enzalutamide + radium-223 has already made the NCCN guidelines, albeit with limitations:
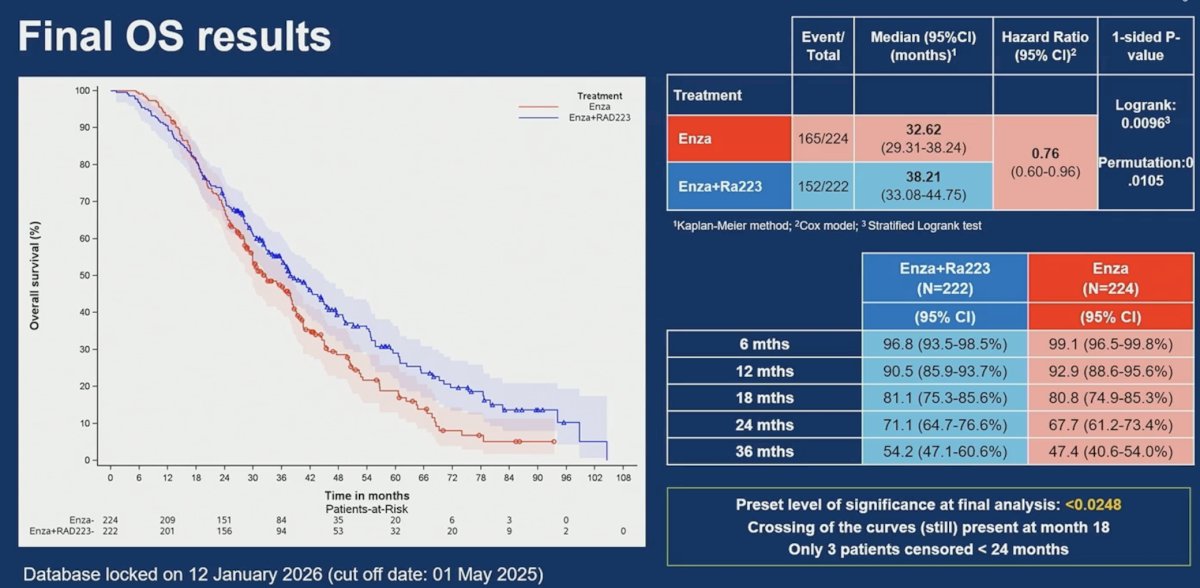
In the final analysis of EORTC-1333 PEACE-3, the median overall survival was 38.21 months for enzalutamide + radium 223 and 32.62 months for enzalutamide alone, corresponding to a hazard ratio of 0.76 (95% CI 0.60–0.96; one-sided stratified log rank p-value 0.0096, with a preset level of significance at final analysis of < 0.0248). Based on the permutation test, the statistical test on overall survival is significant (resulting in a 1-sided p-value of 0.0088 < 0.0248):
Dr. Yu posed the question, is this surprising? PREVAIL1 showed an improvement in overall survival for enzalutamide versus placebo, and ALSYMPCA2 showed an improvement in overall survival for radium-223 versus placebo:
![Dr. Yu posed the question, is this surprising? PREVAIL1 showed an improvement in overall survival for enzalutamide versus placebo, and ALSYMPCA [2] showed an improvement in overall survival for radium-223 versus placebo:](/images/com-doc-importer/247-asco-gu-2026/asco-gu-2026-discussant-choosing-a-treatment-strategy-for-patients-with-mcrpc---all-in-or-play-the-long-game/image-2.jpg)
Additionally, we have other examples for patients with metastatic castration sensitive prostate cancer (mCSPC) of additive or synergistic overall survival effects, including PEACE-13 and ARASENS.4 For mCRPC, we have fewer such overall survival effects from combination therapy, although TALAPRO-25 was successful.
Regarding the overall survival curves crossing, how do we deal with this from a trial statistician's standpoint? Log-rank p-value is the standard non-parametric method used in clinical trials to compare survival curves; however, it is most powerful when proportional hazards assumptions hold. Alternative methodologies when overall survival curves cross include:
- Restricted Mean Survival Time – instead of comparing “risk,” this measures the average survival time (area under the curve) for each group up to a specific point
- Weighted log-rank tests – apply weights to different parts of the trial
- Max-combo test – runs multiple versions of log-rank with different weights and picks the one that finds the most evidence, while adjusting the p-value for the multiple looks
Dr. Yu also highlighted several limitations of the EORTC-1333 PEACE-3 trial:
- The patient population is not contemporary, where many patients have received prior androgen receptor antagonists or abiraterone
- It is tough to rationalize enzalutamide + radium-223 in patients progressing on prior ADT with enzalutamide, apalutamide, or darolutamide
- But if prior abiraterone? This could be considered since there are still responses to enzalutamide after abiraterone
- There was no crossover for patients on the enzalutamide alone control arm
- But why would there be? There is no label for radium for asymptomatic patients
- Could overlapping toxicities with early radium-223 limit the use of future 177Lu-PSMA-617 or chemotherapy?
To address the last limitation, Dr. Yu discussed the RALU study,6 which published an interim analysis in 2023, showing that the median time between treatment with radium-223 and 177Lu-PSMA-617 therapy was 9.3 months (range: 0.9-41.9), with an acceptable toxicity given the grade 3-4 treatment-emergent adverse event rate was 41%. The median overall survival from the first radium-223 injection was 31.4 months, and the overall survival from the first 177Lu-PSMA-617 injection was 12.6 months. Thus, in patients with bone-predominant disease, radium-223 before 177Lu-PSMA-617 treatment was clinically feasible and well tolerated, with a similar survival outcome to those reported in previous studies.
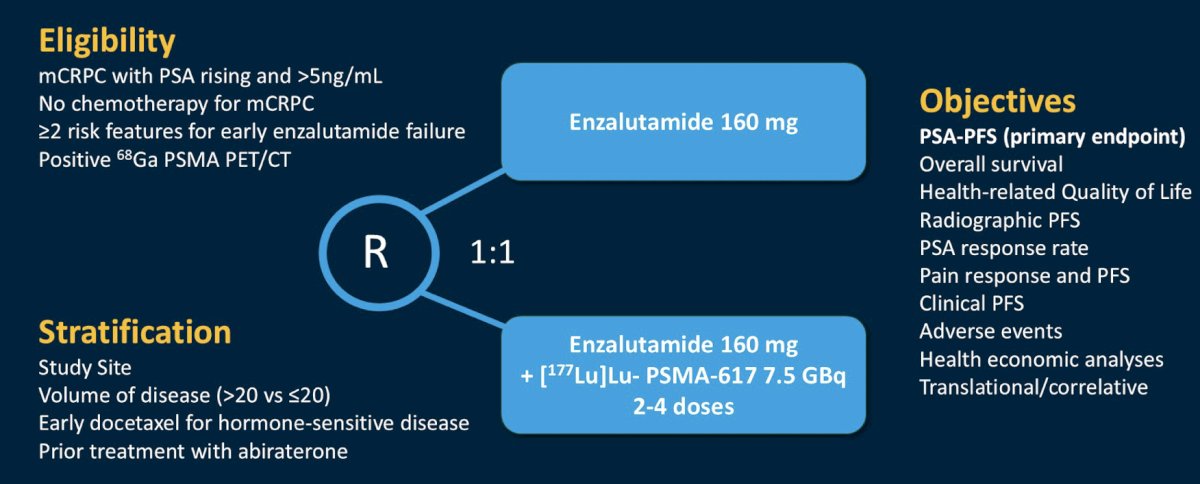
The second study mentioned by Dr. Yu was the ENZA-p trial, which randomly assigned 162 participants to enzalutamide 160 mg daily alone, or in combination with (2 or 4 doses) LuPSMA 7.5 GBq. Eligible participants had mCRPC not previously treated with chemotherapy or an androgen receptor pathway inhibitor for mCRPC, 68Ga-PSMA PET-avid disease, and at least 2 risk factors (LDH >= ULN, ALP >= ULN, albumin <35 g/L, de novo metastatic disease at diagnosis, <3 years since initial diagnosis, >5 bone metastasis, visceral metastasis, PSA doubling time < 84 days, pain requiring opiates > 14 days, prior abiraterone) for early disease progression on enzalutamide-alone:
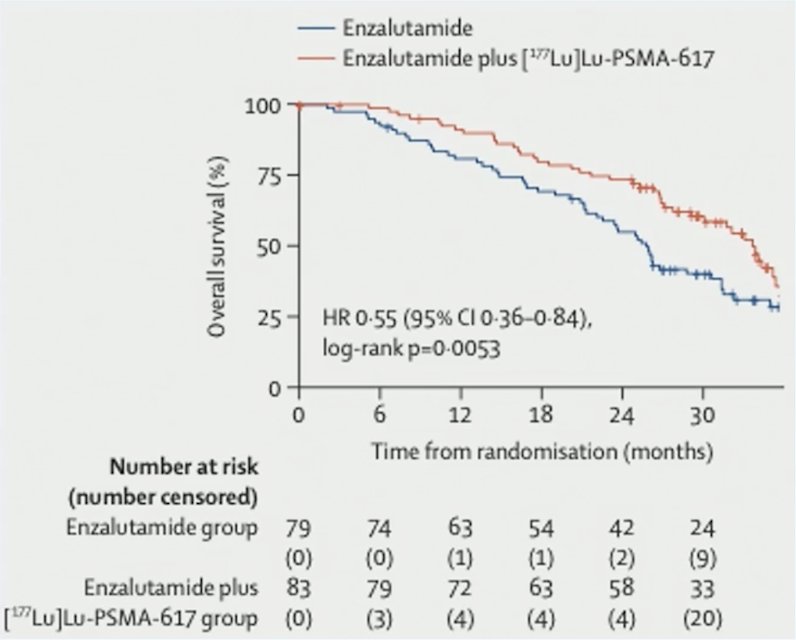
A total of 96 deaths were reported after a median follow-up of 34 months (IQR 29-39): 53 among those assigned enzalutamide-alone and 43 among those assigned enzalutamide + LuPSMA. Overall survival was longer in the enzalutamide + LuPSMA group than the enzalutamide-alone group: median 34 months versus 26 months (HR 0.55, 95% CI 0.36 to 0.84; p = 0.005):
To conclude his discussion of PEACE-3, Dr. Yu offered the following clinical context and application of this data:
- It is easy to consider this data as not applicable to a population that has received prior treatment intensification with an androgen receptor pathway inhibitor for mCSPC
- However, radium-223 has now been shown to offer an overall survival benefit in an earlier patient population and should not be reserved for the heavily pre-treated, symptomatic patients
- Recall that enzalutamide, after abiraterone, still has some patient responses
- Do you need to respond to enzalutamide to benefit from the combination with radium-223?
- Theoretical statement: enzalutamide and 177Lu-PSMA-617 technically hit intersecting pathways that can transiently increase PSMA expression, but then PSMA expression decreases, whereas enzalutamide with radium-223 has the potential to increase bone turnover with a healing flare and facilitate radium-223 incorporation into bone
- How do we sequence with 177Lu-PSMA-617?
- Remember that 177Lu-PSMA-617 requires receipt of a prior androgen receptor pathway inhibitor
- We can give 177Lu-PSMA-617 after radium-223
- Do not forget to provide the patient with bone protective agents and encourage good dental care as there was a 6.4% risk of osteonecrosis of the jaw with the combination in this trial
To start his presentation discussing BRCAAway, Dr. Yu notes that the BRCAAway/PROPEL [8] regimen has already made the NCCN guidelines, albeit with limitations:
![To start his presentation discussing BRCAAway, Dr. Yu notes that the BRCAAway/PROPEL [8] regimen has already made the NCCN guidelines, albeit with limitations:](/images/com-doc-importer/247-asco-gu-2026/asco-gu-2026-discussant-choosing-a-treatment-strategy-for-patients-with-mcrpc---all-in-or-play-the-long-game/image-5.jpg)
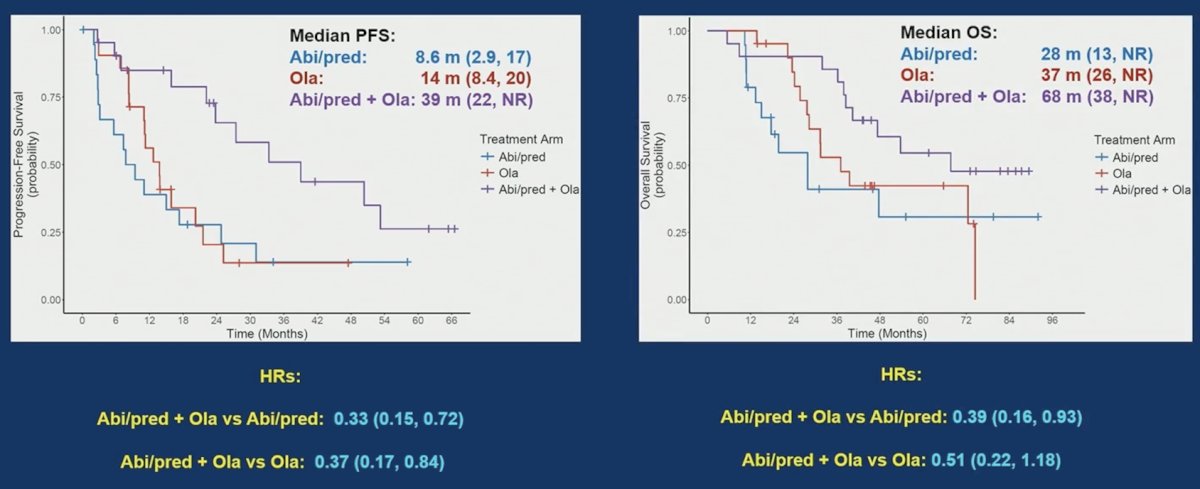
In BRCAAway, progression-free survival showed an HR for abiraterone + prednisone + olaparib versus abiraterone + prednisone of 0.33 (95% CI 0.15-0.72) and for abiraterone + prednisone + olaparib versus olaparib of 0.37 (95% CI 0.17-0.84). For overall survival, abiraterone + prednisone + olaparib had the longest median overall survival of 68 months (95% CI: 38–not reached), compared to abiraterone + prednisone median of 28 months (95% CI: 13– not reached), with a HR of 0.39 (95% CI 0.16–0.93), and compared to olaparib median of 37 months (95% CI 26– not reached), with a HR of 0.51 (95% CI 0.22–1.18):
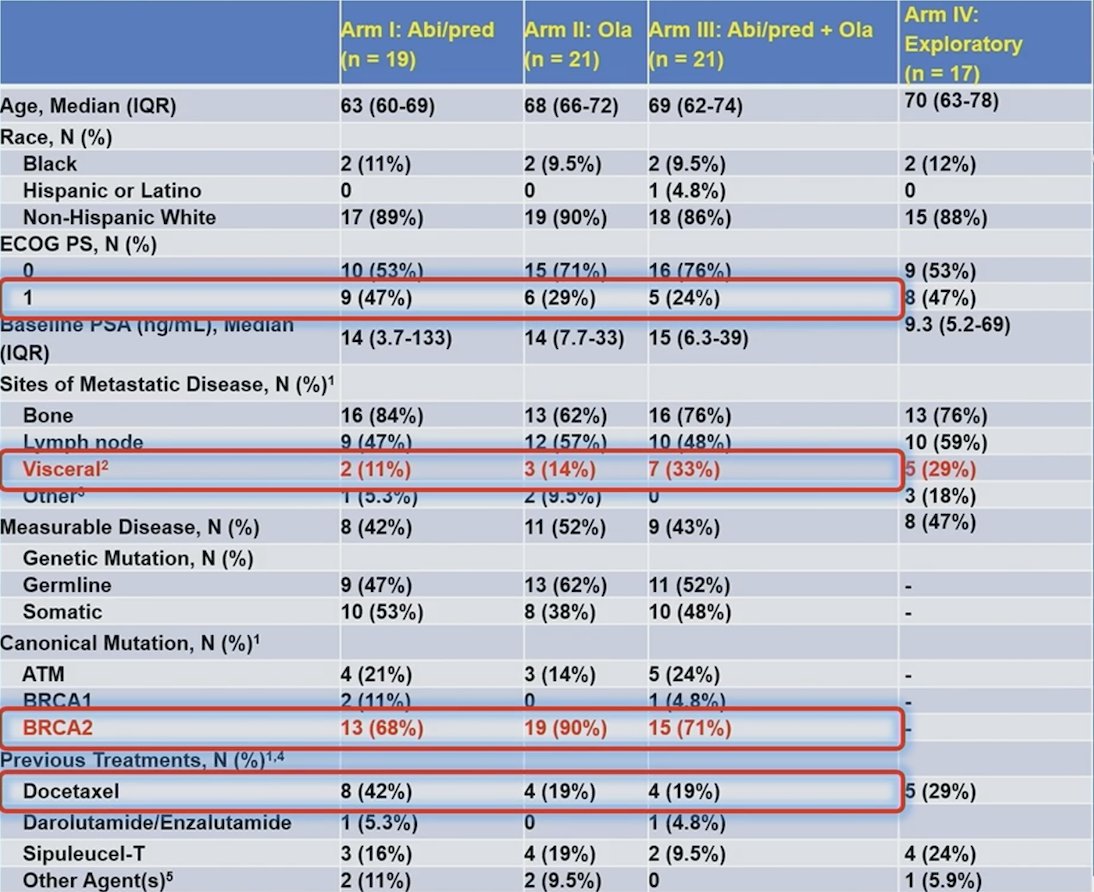
Dr. Yu cautions that we must interpret these results within the context of a small trial/sample size. Notably, it is hard to balance treatment arms:
Are the overall survival outcomes surprising for BRCAAway? Dr. Yu notes that perhaps not for the BRCA1/2 population, based on previously reported PARP inhibitor trials:

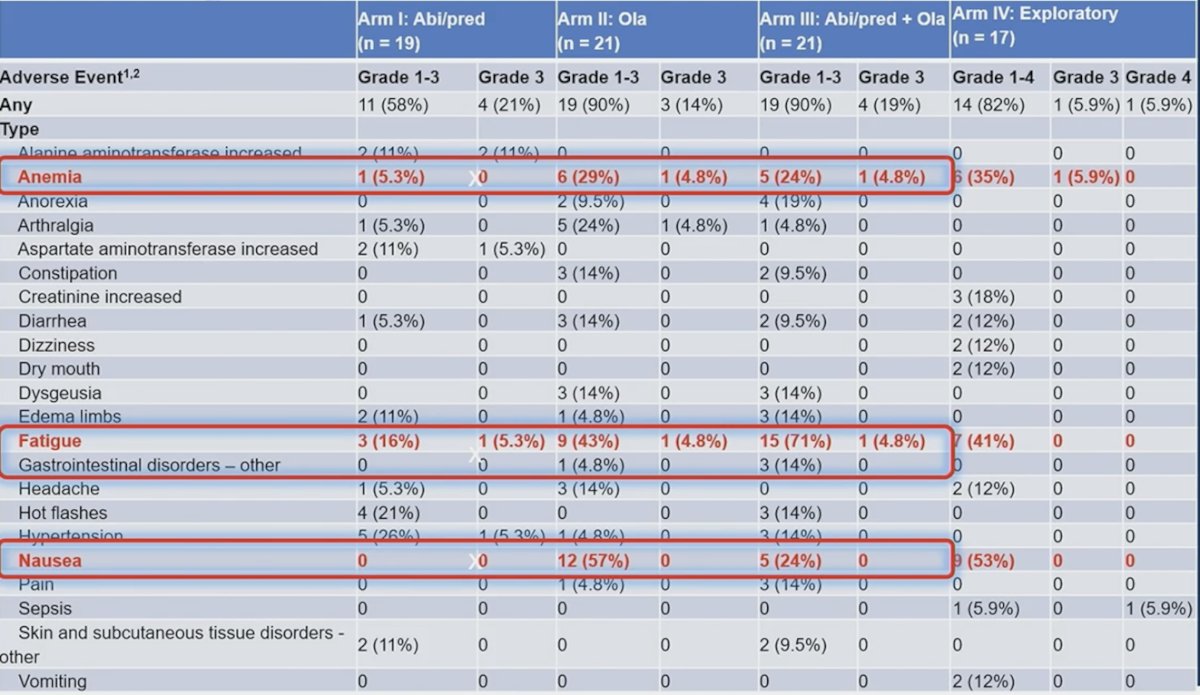
Dr. Yu notes that we should also take this data within the context of assessing adverse events, specifically anemia, fatigue, and nausea:
Dr. Yu emphasized the following limitations for BRCAAway:
- Trial design:
- A very small trial makes it more prone to imbalances in the arms
- Not statistically powered for overall survival
- Crossover was not mandated, and bias is introduced when you evaluate the self-selected patients who do crossover
- No prior androgen receptor pathway inhibitor use was allowed, and the NCCN guidelines have not listed the abiraterone + olaparib combination for prior androgen receptor pathway inhibitor patients
- Clinical and practical issues:
- Toxicity – seems acceptable, but there are subtleties with PARP inhibitor fatigue and gastrointestinal side effects
- MDS/AML – we need long-term data from larger populations
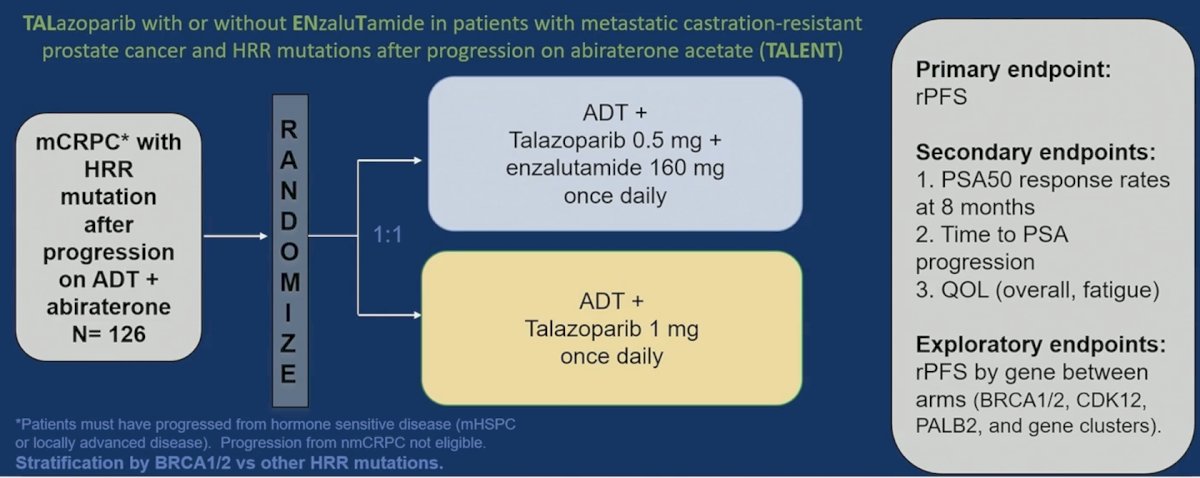
Whether we really need androgen receptor pathway inhibitors in those previously experienced patients will be answered by the ongoing TALENT trial:
To conclude his discussion of BRCAAway, Dr. Yu offered the following clinical context and application of this data:
- Is a combination of androgen receptor pathway inhibitor + PARP inhibitor for everyone with pathogenic BRCA1/2 alteration?
- No. This is a small trial and does not adequately address crossover and subsequent therapy issues
- However, it builds on the body of evidence for combination therapy
- This also supports the opportunity to give PARP inhibitors early
- We need better studies of clinical and molecular features of which BRCA1/2 altered patients will have very aggressive versus more indolent courses
- Always consider quality of life and the increased fatigue, gastrointestinal toxicity, and myelotoxicity issues
Dr. Yu concluded his discussant presentation with the following take-home points:
- These trials are not a perfect fit for most of our clinics, but they can provide a general guide
- Due to our successes, it is now difficult to achieve the gold standard of overall survival in clinical trials
- These combination therapy options are available to us now, but we need to carefully discuss the risks and benefits and individualize our approach for each patient
Presented by: Evan Yu, MD, Professor of Medicine, Division of Oncology, University of Washington School of Medicine, Section Head of Cancer Medicine, Medical Director of Clinical Research Support, Fred Hutchinson Cancer Center, The University of Washington School of Medicine, Seattle, WA
- Beer TM, Armstrong AJ, Rathkopf DE, et al. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med 2014;371(5):424-433.
- Parker C, Nilsson S, Heinrich D, et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med 2013;369(3):213-223.
- Fizazi K, Foulon S, Carles J, Roubaud G, et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): A multicentre, open-label, randomized, phase 3 study with a 2 x 2 factorial design. Lancet. 2022 Apr 30;399(10336):1695-1707.
- Smith MR, Hussain M, Saad F, et al. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med. 2022 Mar 24;386(12):1132-1142.
- Agarwal N, Azad AA, Carles J, et al. Talazoparib plus enzalutamide in men with metastatic-castration-resistant prostate cancer: final overall survival results from the randomized, placebo-controlled, phase 3 TALAPRO-2 trial. Lancet. 2025 Aug 2;406(10502):447-460.
- Rahbar K, Essler M, Pabst KM, et al. Safety and Survival Outcomes of 177Lu-Prostate-Specific Membrane Antigen Therapy in Patients with Metastatic Castration-Resistant Prostate Cancer with Prior 223Ra Treatment: The RALU Study. J Nucl Med. 2023 Apr;64(4):574-578.
- Emmett L, Subramaniam S, Crumbaker M, et al. Overall survival and quality of life with [177Lu]Lu-PSMA-617 plus enzalutamide versus enzalutamide alone in metastatic castration-resistant prostate cancer (ENZA-p): Secondary outcomes from a multicentre, open-label, randomized, phase 2 trial. Lancet Oncol. 2025 Mar;26(3):291-299
- Saad F, Clarke NW, Oya M, et al. Olaparib plus abiraterone versus placebo plus abiraterone in metastatic castration-resistant prostate cancer (PROpel): final prespecified overall survival results of a randomized, double-blind, phase 3 trial. Lancet Oncol. 2023 Oct;24(10):1094-1108.