(UroToday.com) The 2026 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Anna Wilkins discussing external validation of a digital pathology-based MMAI-derived prognostic biomarker in the randomized phase III CHHiP trial. Risk stratification in localized prostate cancer based on clinicopathological parameters is inadequate, leading to under- and over-treatment. As such, Dr. Wilkins and colleagues used the CHHiP trial1 data to externally validate a previously-developed MMAI prognostic model with potential for cost-effective improved treatment personalization.
H&E slides from the CHHiP translational substudy patients were centrally reviewed by a uropathologist between 2013 and 2015, with Gleason grade group rescored using contemporary guidelines. The Gleason grade group was reassigned in 52% of cases. The investigators evaluated the locked ArteraAI prostate MMAI algorithm v1.2, which combines age, T-stage, and PSA with digital prostate biopsy H&E images. Multivariable Cox regression analysis of biochemical/clinical recurrence (trial primary endpoint) and development of distant metastases was performed with models including age and MMAI as continuous (per 0.1 increase) and categorical (ArteraAI pre-validated 3-tier risk groups) variables. The additional prognostic value of MMAI beyond UK-recommended Cambridge Prognostic Group (CPG) and NCCN risk group models was assessed by change in Concordance Index and Likelihood Ratio Test (LRT):

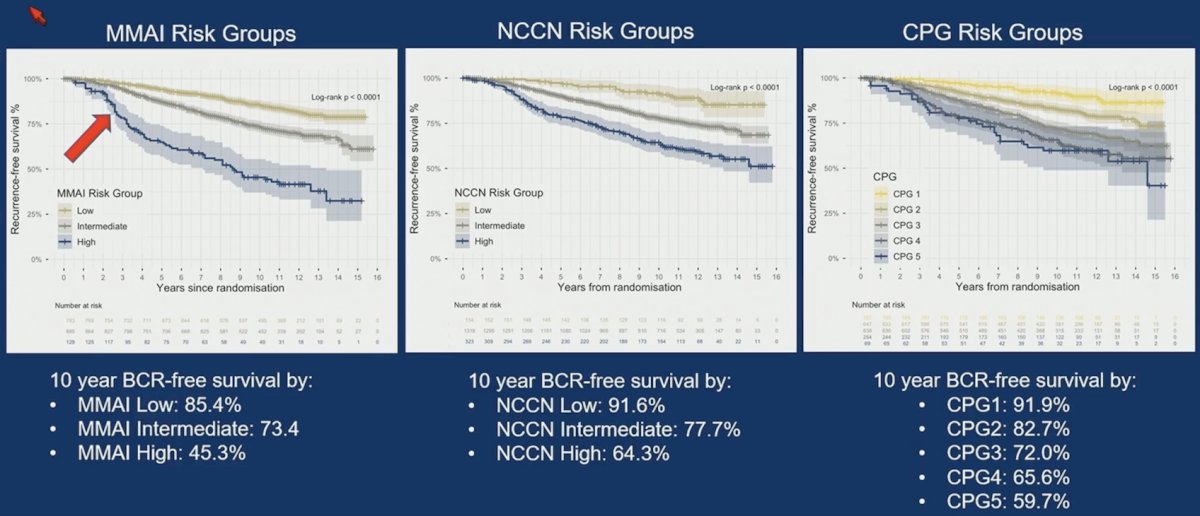
Of 1,854 patients with centrally-reviewed pathology, 1,797 (97%) had clinical data and H&E with sufficient tumour for MMAI analysis. The median follow-up was 14.3 years. Patients were classified as MMAI High (n = 129, 7.2%), Intermediate (n = 885, 49.2%), or Low (n = 783, 43.6%). In univariable analysis, high MMAI score was significantly associated with increased biochemical/clinical recurrence risk, as both a categorical variable (MMAI High risk HR 5.07, 95% CI 3.77-6.81, p < 0.001, MMAI Intermediate-risk HR 1.90, 1.52-2.36, p < 0.001), and continuous variable (MMAI raw score HR 1.55, 1.44-1.67, p < 0.001):
Similarly, MMAI was also significantly associated with distant metastases: 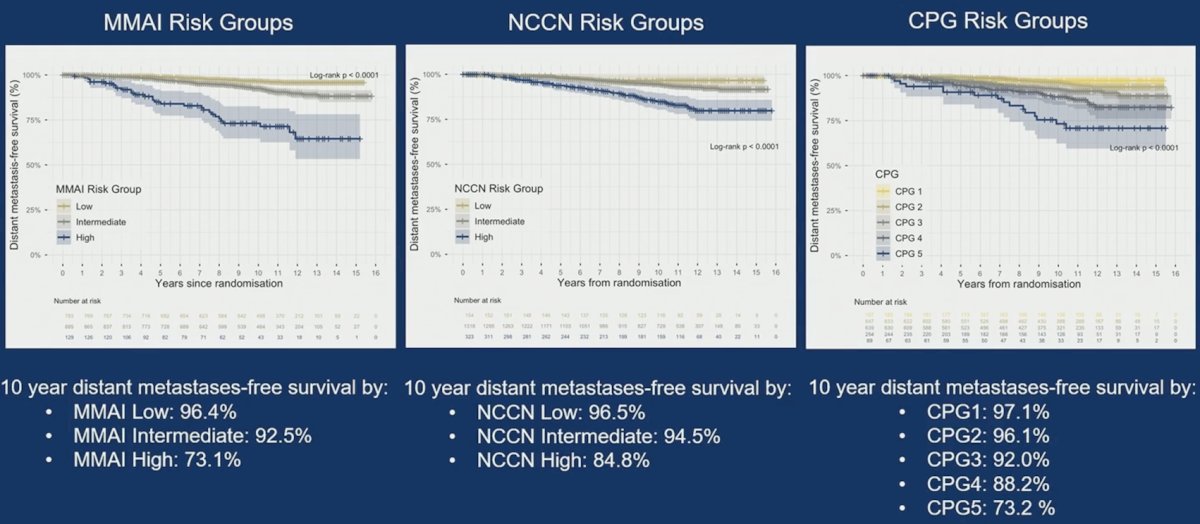
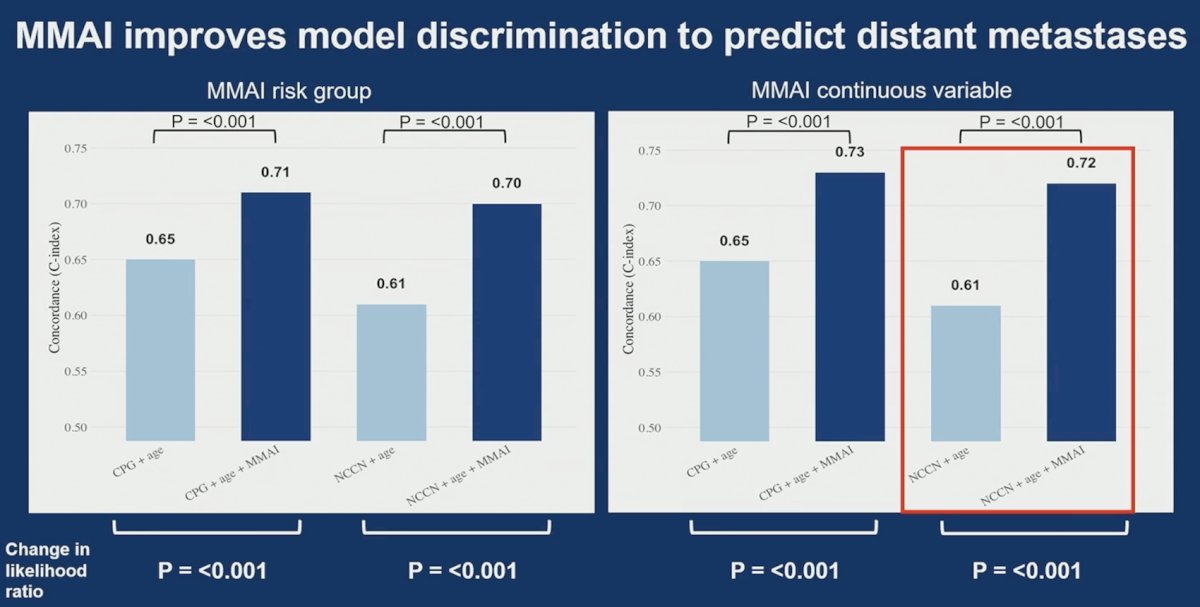
The addition of MMAI to CPG and NCCN multivariable models significantly improves discrimination (C-index) and overall fit (change in LRT) for biochemical/clinical recurrence and distant metastases: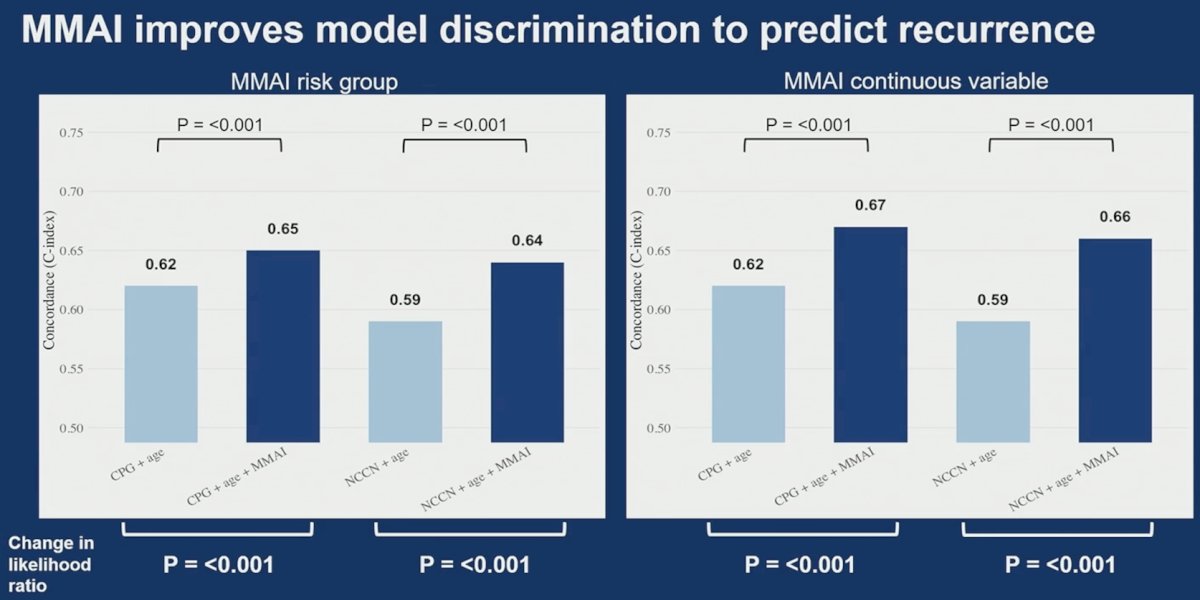
Dr. Wilkins concluded her presentation discussing external validation of a digital pathology-based MMAI-derived prognostic biomarker in the randomized phase III CHHiP trial with the following take-home points:
- ArteraAI MMAI improves the prediction of biochemical/clinical recurrence and distant metastases in CHHiP over standard criteria
- This first large-scale external validation in a contemporary UK cohort of localized prostate cancer with rigorously standardized care will inform future prospective trials of MMAI biomarker-guided prostate cancer treatment selection
Presented by: Anna C. Wilkins, Clinician Scientist, The Institute of Cancer Research, London, UK
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 26 – Sat, Feb 28, 2026.
Related content: CHHiP Trial Evaluates a Multimodal AI Biomarker in Localized Prostate Cancer - Anna Wilkins