(UroToday.com) The 2026 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Ashesh Jani discussing the genomic risk classifier performance in PET-guided post-prostatectomy patients. Genomic risk assessment with genomic classifiers has enhanced risk stratification in post-prostatectomy patients; however, validation studies have relied on conventional imaging workup to guide secondary radiation treatment. The hypothesis of this study is that genomic classifiers will remain prognostic in a population receiving PET-guided secondary radiation treatment.
The investigators performed a protocol-specified whole-transcriptome assay (Decipher genomic classifier) on prostatectomy specimens from patients enrolled on a randomized trial studying event-free survival (biochemical/clinical/radiologic progression or systemic therapy initiation) of 18F-fluciclovine or 68Ga-PSMA-11 guided secondary radiation treatment with incorporated PET-guided dose escalation. Treatment volumes and prescription doses were rigidly defined on protocol:
- No uptake/prostate bed only - prostate bed radiotherapy (64.8-70.2 Gy at 1.8 Gy/fx)
- Pelvic nodal +/- prostate bed uptake – pelvic nodal (45-50.4 Gy at 1.8 Gy/fx) + prostate bed radiotherapy
- Extrapelvic – no radiotherapy
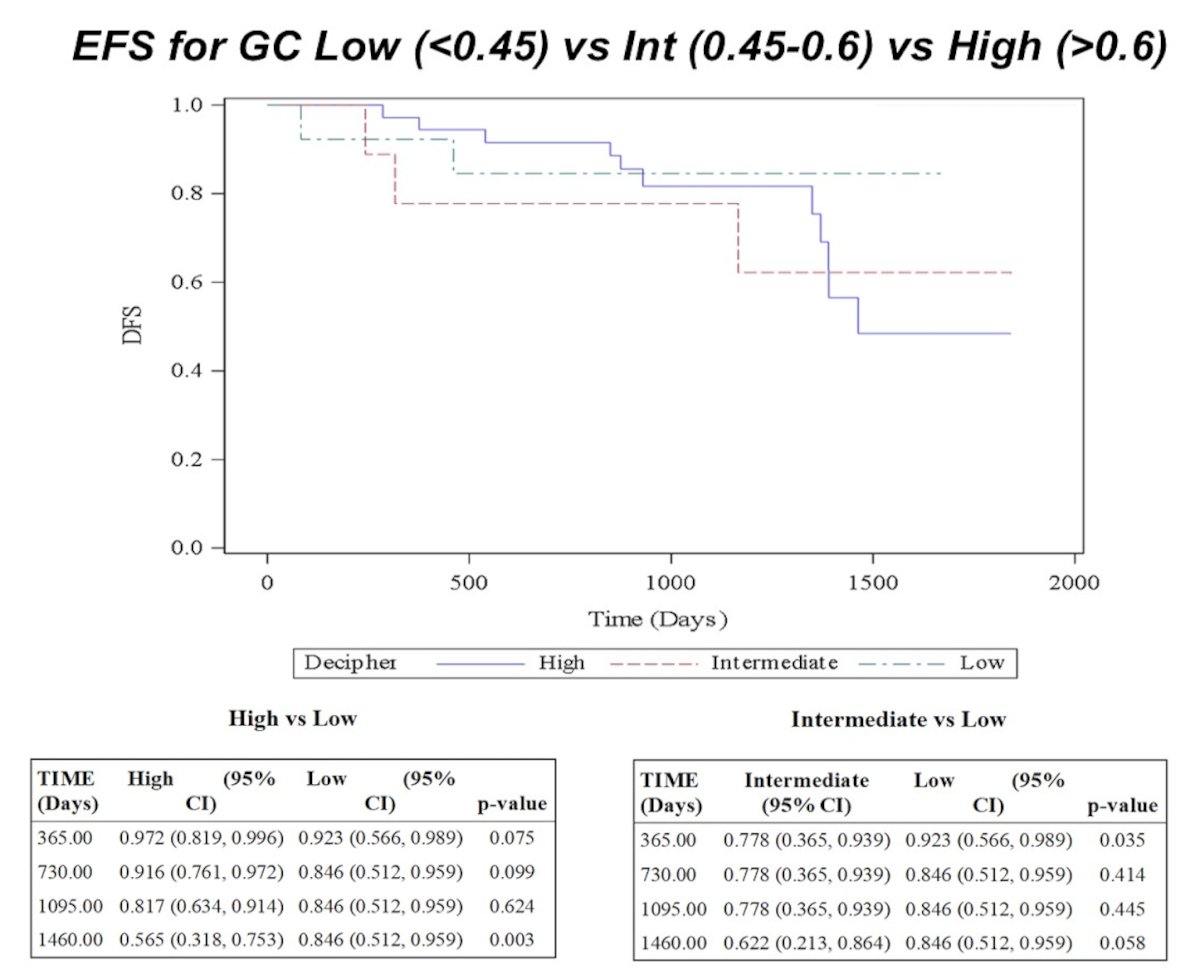
Sites of PET uptake received simultaneous integrated boosts of 74-76 Gy at 2 Gy/fx in the prostate bed and 54-56 Gy at 2 Gy/fx in the pelvic nodal. Genomic classifiers were categorized as low (0-0.44), intermediate (0.45-0.6), and high (>0.6) as reported for commercial testing. An optimal cutoff maximizing separation above versus below the maximal cutoff was identified using a bias-adjusted log-rank test. A Z-test was performed at specified time points to assess event-free survival between cohorts per study protocol.
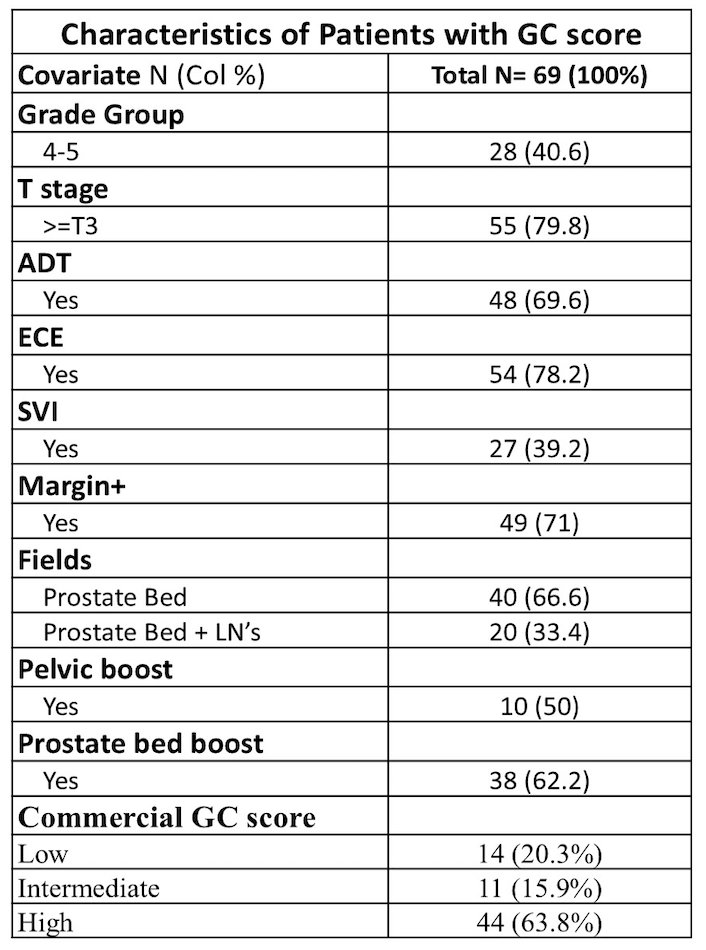
Of 140 patients enrolled on trial, 69 (49.3%) had prostatectomy specimens available for genomic classifier analysis, with 44 (63.8%) high, 11 (15.9%) intermediate, and 14 (20.3%) low scores. ADT was given in 4/14 (28.6%) low, 8/11 (72.7%) intermediate, and 36/44 (81.8%) high genomic classifier patients based on clinical characteristics:
Minimum follow-up was 2.0 years (median 2.9 years, range: 2.0-5.0 years). High genomic classifier was associated with worse 4-year event-free survival compared to low genomic classifier (56.5% versus 84.6%, p < 0.01):
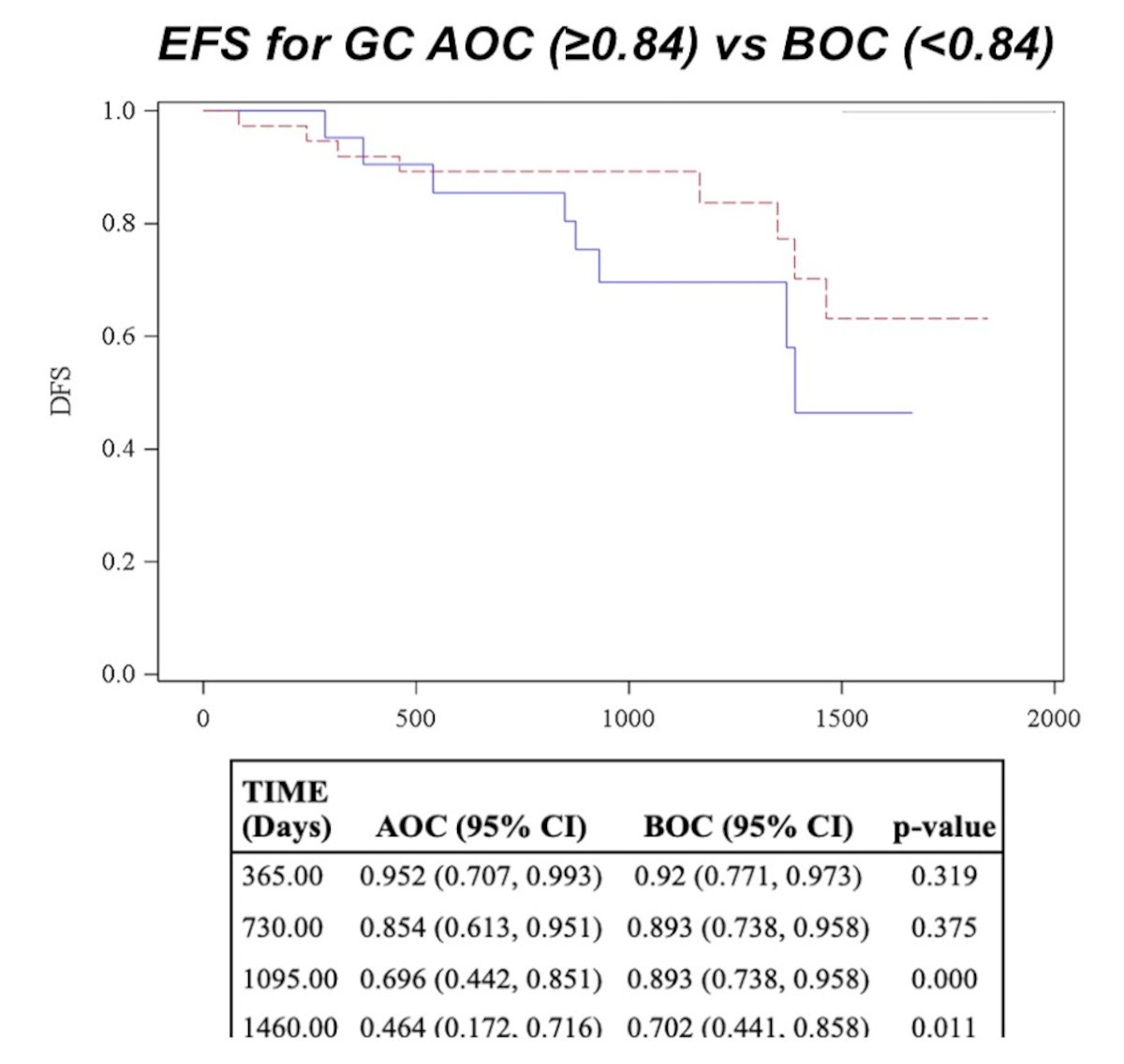
The optimal genomic classifier cutoff was 0.84, with 28 above the maximal cutoff (23/28 with ADT) and 41 below the maximal cutoff (25/41 with ADT). Score above the maximal cutoff was associated with worse 3-year (69.6% versus 89.3%, p < 0.01) and 4-year (46.4% versus 70.2%, p = 0.01) event-free survival compared to below the maximal cutoff:
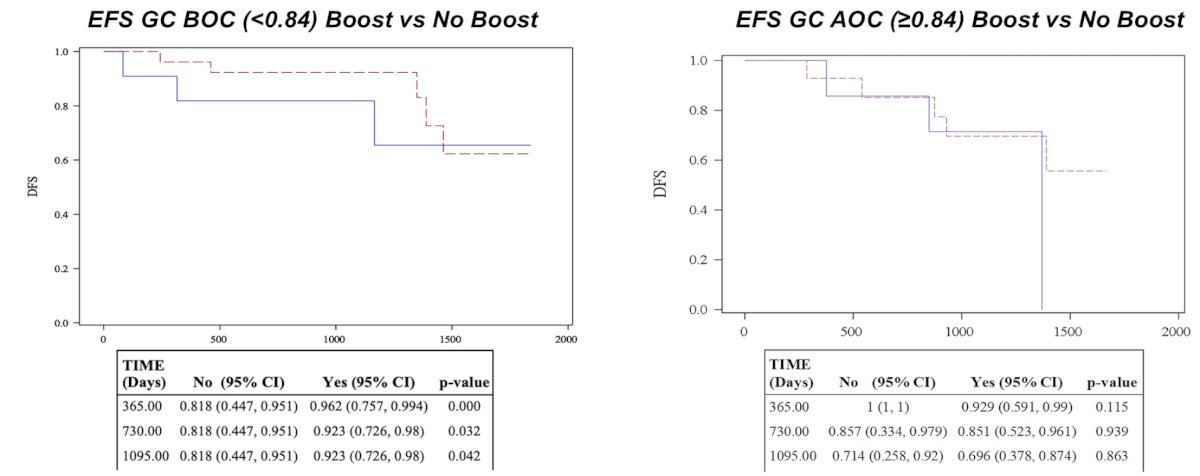
Use of simultaneous integrated boosts was associated with improved event-free survival in scores below the maximal cutoff at 2 and 3-years post treatment (81.8% versus 92.3% at both time points, p = 0.03); however, simultaneous integrated boosts were not associated with improved event-free survival in scores above the maximal cutoff at 2 years or beyond:
Dr. Jani concluded this presentation discussing the genomic risk classifier performance in PET-guided post-prostatectomy patients with the following take-home points:
- The genomic classifier remained prognostic for event-free survival in post-prostatectomy patients treated with PET-guided radiation when assessed at commercial and optimal cutoff values
- Dose escalation to sites of PET uptake was associated with improved event-free survival at 2+ years in patients below the maximal cutoff (<0.84) patients
- Creation of an integrated radiogenomic model based on PET findings and a genomic classifier is forthcoming
Presented by: Ashesh B. Jani, MD, MSEE, FASTRO, Emory University, Atlanta, GA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 26 – Sat, Feb 28, 2026.