(UroToday.com) The 2026 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Karim Fizazi discussing the first results of the PEACE-2 randomized phase III trial assessing ADT and radiotherapy with or without cabazitaxel in very high risk localized prostate cancer. In 2012, when this trial was designed, very high risk localized prostate cancer was defined as:
- 2+ risk factors among T3-T4, Gleason score 8-10, and/or PSA ≥20 ng/mL
- No detectable nodal disease or metastases by conventional imaging (bone scan + CT scan)
At that time, the standard therapy was radiotherapy + long term ADT (ie. 3 years). The role of pelvic radiotherapy was debated, but it did show improved relapse free survival with docetaxel in GETUG-12. Cabazitaxel has also been shown to improve overall survival in patients with mCRPC;1 thus, Dr. Fizazi and colleagues hypothesized that earlier use of cabazitaxel may prevent the onset of relapse or death.
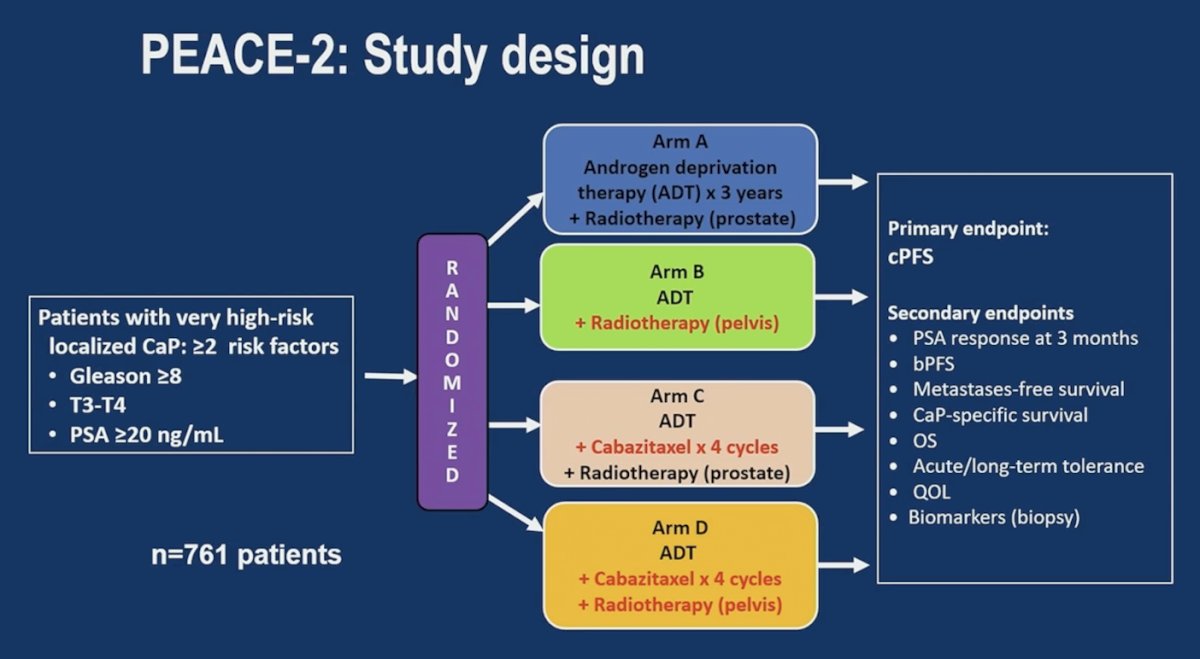
PEACE 2 (NCT01952223) is a 2x2 factorial design randomized trial for patients with very high-risk localized prostate cancer (defined by at least 2 criteria among: Gleason 8-10, T3/T4 disease (MRI T stage permitted), and PSA ≥20 ng/mL) and no detectable metastases on conventional imaging. Eligible patients all received standard of care, which consisted of prostate only fractionated radiotherapy (74-78 Gy in 37-39 fractions) and 3 years of ADT. Patients were then randomized 1:1:1:1 to receive:
- Standard of care only (Arm A)
- Standard of care + prophylactic pelvic radiotherapy (46-50 Gy in 23-25 fractions, Arm B)
- Standard of care + 4 cycles of cabazitaxel (20-25 mg/m2 3 weeks x 4 cycles) prior to radiotherapy (Arm C)
- Standard of care + both cabazitaxel and pelvic radiotherapy (Arm D)
The primary endpoint is clinical progression free survival with death, metastases, and proven local relapses as events:
Initially, 1,048 patients were planned to detect a treatment effect corresponding to a hazard ratio of 0.70 (absolute difference of 7.5% in clinical progression free survival at 6 years) for both comparisons. The accrual was closed early, but the analysis plan was maintained after the target event number was reached (n = 247 planned events), hence maintaining statistical power. Interaction was first tested between cabazitaxel and pelvic radiotherapy: if no interaction was detected, hazard ratios (Cox, log rank) for clinical progression free survival were reported for ADT + radiotherapy versus ADT + radiotherapy + cabazitaxel. The database was locked in October 2025.
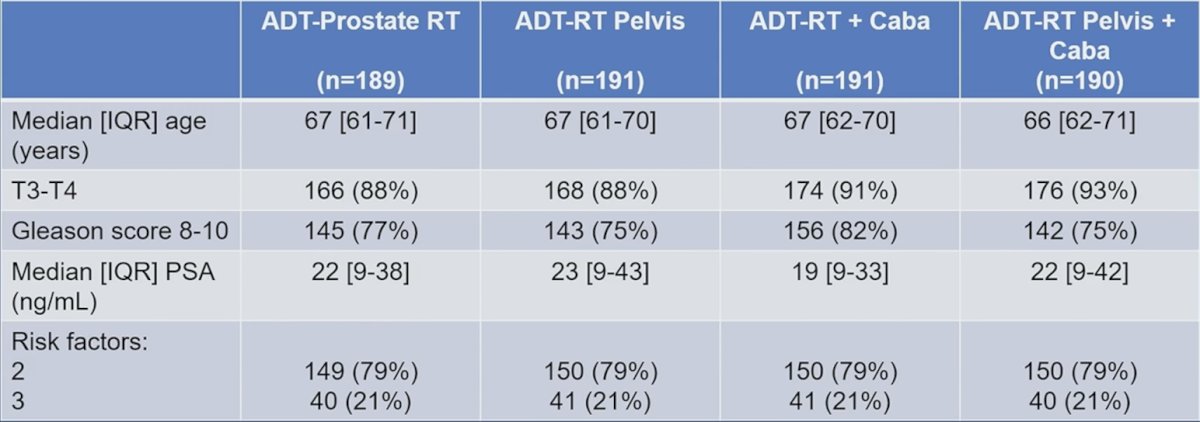
Overall, 761 patients were included from 2013 to 2021 from 4 European Union countries, with 2 (79%) or 3 (21%) risk factors. Patients were randomized to receive cabazitaxel (n = 381) or not (n = 380). Pet-choline was used as part of baseline imaging in 18% of patients. The median follow-up was 7.3 years (95% CI 7.1 – 7.5), and no interaction was found between cabazitaxel and pelvic radiotherapy. The median age was 67 years, and the complete baseline characteristics were as follows:
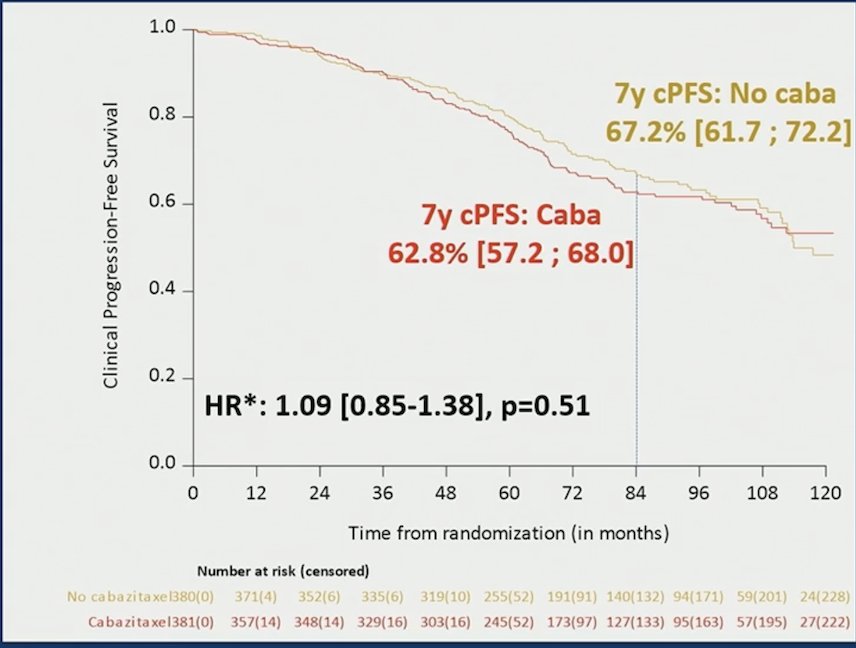
PEACE-2 found that there was no improvement in clinical progression free survival with cabazitaxel (HR 1.09, 95% CI 0.85-1.38), with 7-year clinical progression free survival rates of 62.8% versus 67.2%:
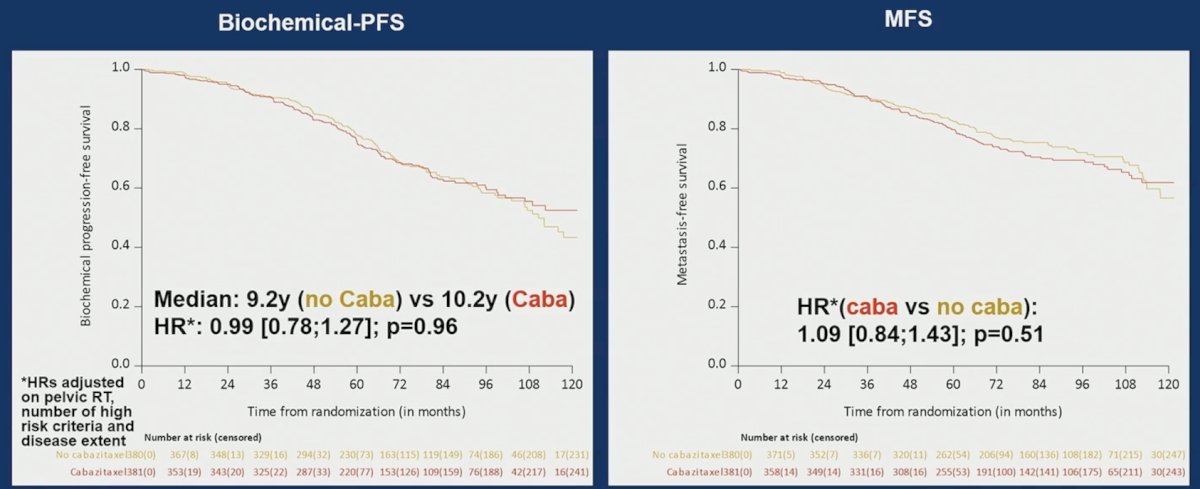
Moreover, there were no differences in biochemical progression free survival (HR 0.99, 95% CI 0.78-1.27) and metastasis free survival (HR 1.09, 95% CI 0.84-1.43):
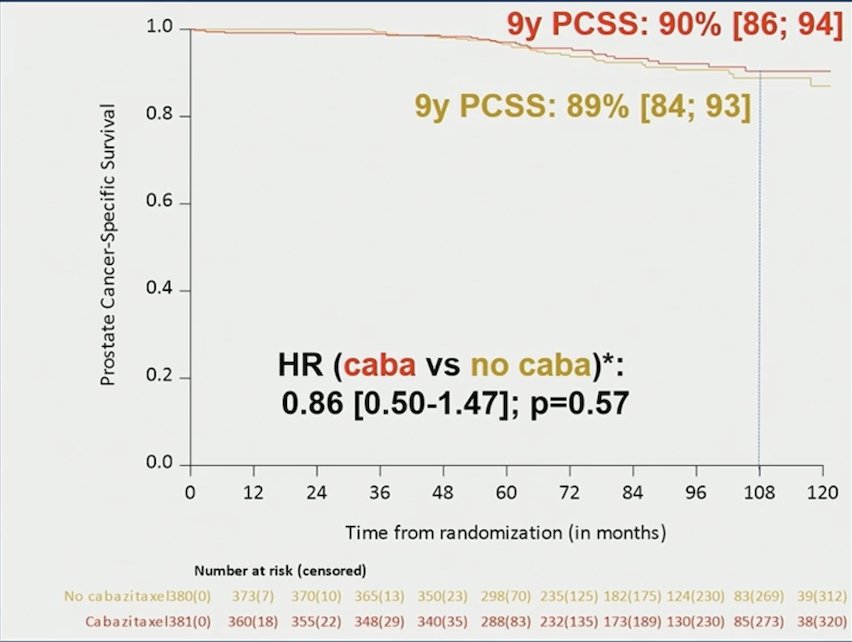
Prostate cancer specific survival had a 9 year rate of 90% with cabazitaxel versus 89% without cabazitaxel (HR 0.86, 95% CI 0.50-1.47):
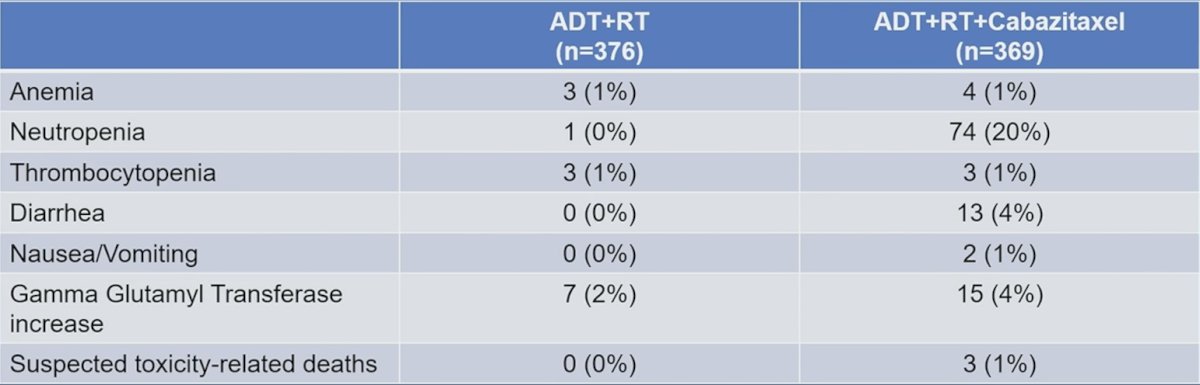
Grade >2 toxicity was reported in 65% and 47% respectively, with or without cabazitaxel, with the following grade 3-4 adverse events of interest in the safety population:
Dr. Fizazi concluded his presentation discussing the first results of the PEACE-2 randomized phase III trial with the following take-home points:
- Cabazitaxel does not improve outcomes in very high risk localized prostate cancer
- With approximately 1 out of 10 men dying from prostate cancer during the first decade, we may challenge the current definition of “very high risk” localized prostate cancer
- This may prove even more true when modern imaging (PSMA PET/CT) does not show nodal/metastatic dissemination
Presented by: Karim Fizazi, MD, PhD, Institut Gustave Roussy, Centre Oscar Lambret, University of Paris Saclay, Villejuif, France
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
References: