(UroToday.com) The 2026 ASCO GU Annual Symposium was host to a trials-in-progress prostate cancer poster session. Dr. Louise Emmett presented OPTIMAL-PSMA, an ongoing randomized phase II trial that is evaluating dose optimization and PSMA receptor intensification with 177Lu-PSMA-597 in metastatic castrate-resistant prostate cancer (mCRPC).
[¹⁷⁷Lu]Lu-PSMA-617 therapy is standard of care for the management of mCRPC, with dosing of 7.4 GBq administered every 6 weeks for up to 6 doses using VISION PSMA PET criteria for patient selection. However, primary treatment resistance is common, and improvement in overall survival is limited.¹ Importantly, the standard dosing regimen for [¹⁷⁷Lu]Lu-PSMA-617 is not based on a dose escalation study and may be significantly underdosing patients for optimal efficacy.
[¹⁷⁷Lu]Lu-PSMA-597 is a novel PSMA-targeted small molecule with a low salivary gland/renal dose. Questions remain whether treatment responses can be improved with dose intensification to optimize the biologically effective dose early in treatment, and if dose intensification with [¹⁷⁷Lu]Lu-PSMA-597 is safe.
This study aims to determine the safety and efficacy of a dosing regimen comprised of an intense induction followed by a maintenance period of [¹⁷⁷Lu]Lu-PSMA-597 therapy, compared to standard-of-care 6 doses weekly in men with mCRPC.
OPTIMAL-PSMA is an open-label, randomized, two-arm, multicentre, phase II trial that randomizes 120 participants 2:1 to either dose-intensified [¹⁷⁷Lu]Lu-PSMA-597 or standard of care.
The eligibility criteria are as follows:
- mCRPC with progressive disease with rising PSA defined by PCWG3 criteria.
- Prior ARPI and prior docetaxel or considered unfit for docetaxel.
- Significant PSMA avidity on ⁶⁸Ga-PSMA PET/CT.
The study is structured with two sequential parts.
Part A (Participants 1–40)
Initial participants undergo dose intensification with three doses administered over 15 days, followed by maintenance dosing every 10 weeks, compared against standard-of-care 6-weekly dosing.
An independent data safety monitoring board evaluates the first 10 participants on the experimental arm at a minimum of 8 weeks after the first dose. If no safety concerns are identified, two protocol adaptations are implemented:
- Planned increase to 8.5 GBq per injection in the experimental arm (from participant 40 onward).
- Amendment of PSMA-PET screening criteria to require SUVmax >15 at ≥1 site and >10 at all larger disease sites (including bone) with no PSMA-negative soft tissue disease (ENZA-P criteria).
For the first 40 participants, eligibility requires ≥1 lesion with PSMA uptake above liver and no PSMA-negative soft tissue sites (VISION criteria). After participant 40, screening criteria are intensified to require SUVmax >15 at ≥1 site and >10 at all larger disease sites, with no PSMA-negative soft tissue disease on diagnostic CT (ENZA-P criteria).
This evolution of eligibility criteria reflects the study’s biologic emphasis on receptor density and potential for dose intensification benefit.
Part A in the figure below visually demonstrates the induction sequence (Days 1, 3, and 15) followed by extended-interval maintenance dosing. In contrast, the control arm receives standard 7.4 GBq dosing every 6 weeks for six cycles.
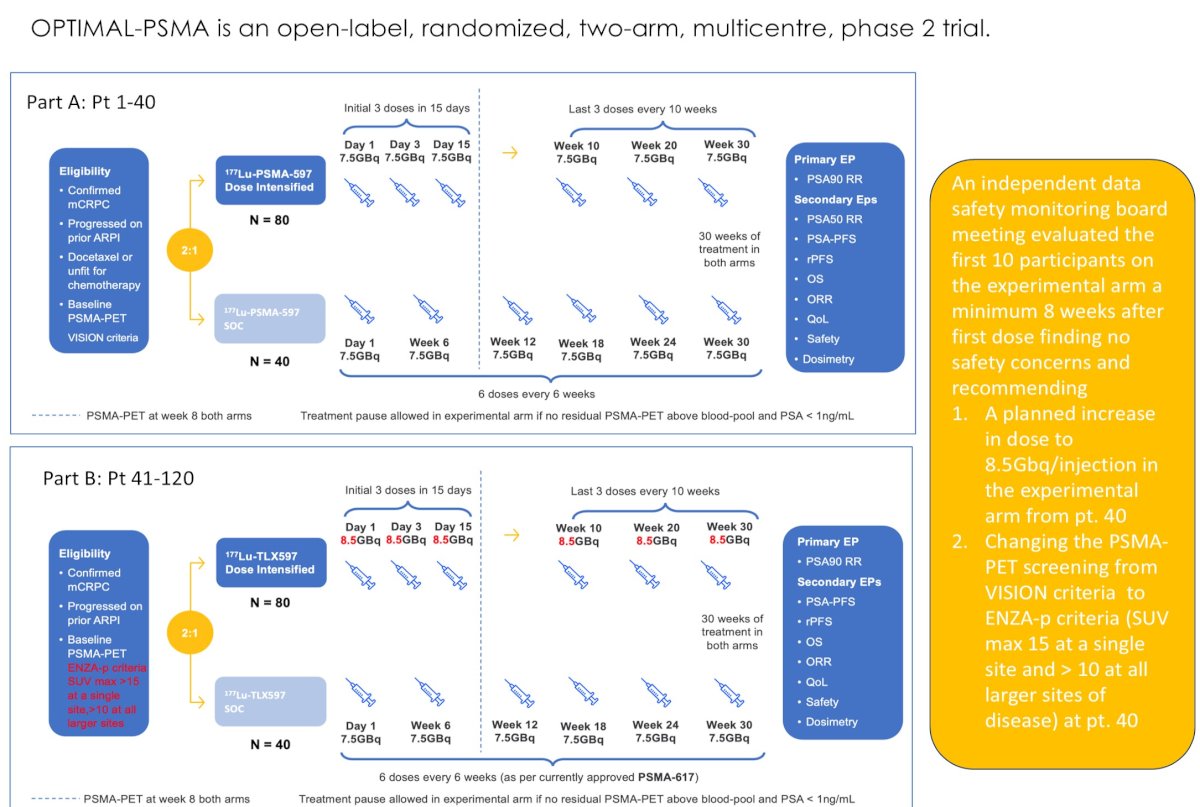
The primary endpoint is PSA50 response.
Secondary endpoints include:
- PSA30 response
- PSA progression-free survival (PSA-PFS)
- Imaging-based PFS (iPFS)
- Overall survival (OS)
- Objective response rate (ORR)
- Quality of life
- Safety
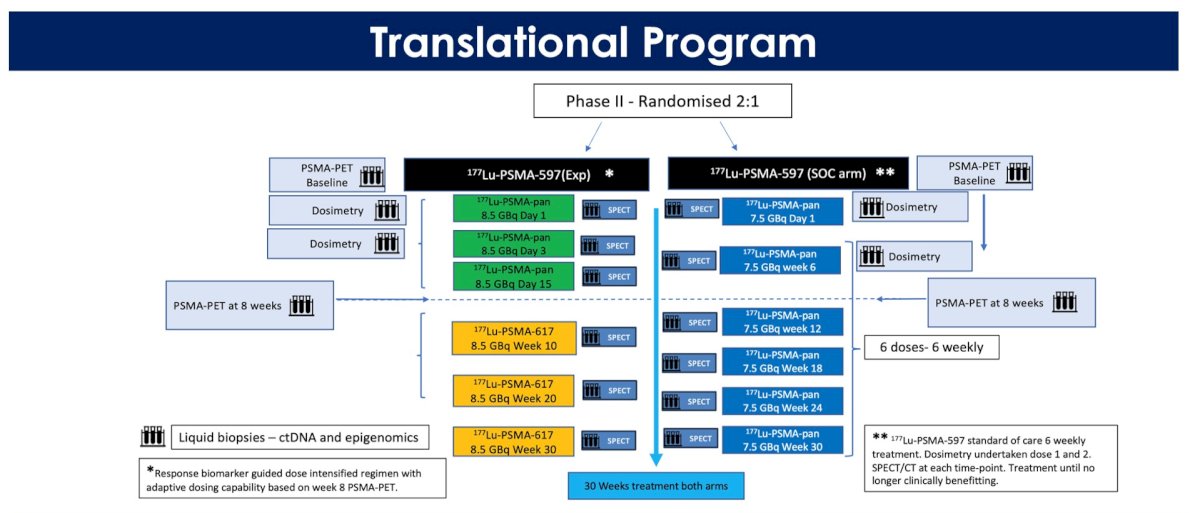
- Dosimetry
Translational bloods for circulating tumor DNA genomic and epigenomic analysis are undertaken on both arms at each treatment timepoint.
Statistical Consideration
Randomization will be (2:1). With an assumed 20% of participants achieving the primary endpoint in the standard dosing arm, the minimum effect size (difference in proportions) that will be detected with 80% power is 0.2451 with a sample size of 120 participants (80:40) recruited over 18 months.
Enrollment and Current StatusEthics approval was obtained on 25 June 2025. St Vincent’s Sydney and Austin Health, Melbourne are actively recruiting sites. Sixty-seven patients have been accrued and randomized.
Presented by: Louise Emmett, BSc(HONS), MBChB, FRACP, FAANMS, MD, The University of New South Wales (UNSW), Sydney, Australia
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
Reference:
- Sartor O, de Bono J, Chi KN, et al. Lutetium-177–PSMA-617 for metastatic castration-resistant prostate cancer. N Engl J Med. 2021;385:1091-1103.