(UroToday.com) At ASCO GU 2026, Dr. Nil Navarro-Gorro presented results from an ongoing phase I study evaluating obrixtamig, a DLL3/CD3 T-cell engager, in patients with extrapulmonary neuroendocrine carcinomas (epNECs) of genitourinary origin.
Extrapulmonary neuroendocrine carcinomas (epNECs) are a heterogeneous, poorly differentiated group of aggressive extrapulmonary cancers arising from neuroendocrine cells, and are associated with poor clinical outcomes.1 Currently, there is no approved second-line standard of care for epNEC; prospective trials for chemotherapy in this setting showed objective response rates (ORRs) of approximately 10–25%.2
DLL3 is widely expressed in epNECs, including those of GU origin (epNEC GU), but is minimally expressed in normal tissues, making it a potential therapeutic target.3-5
This phase I study (NCT04429787) is assessing obrixtamig monotherapy in patients with DLL3-positive SCLC, LCNEC-L, or epNEC who had failed standard treatment.6 In a previous sub-analysis in patients with epNEC, confirmed ORR (40% vs 3%) and median duration of response (7.9 vs 2.8 months) were greater in patients with tumors expressing high versus low levels of DLL3.7 This sub-analysis further examined the efficacy and safety of obrixtamig specifically in patients with GU epNEC according to DLL3 expression.

Mechanistically, obrixtamig is a novel IgG-like T-cell engager targeting DLL3 expressed on tumor cells and CD3 on T cells, redirecting cytotoxic T cells to DLL3-expressing cancer cells and inducing apoptosis. The rationale for biomarker enrichment is therefore biologically compelling.
This was a first-in-human, phase I dose-escalation study evaluating obrixtamig in patients with advanced SCLC, LCNEC-L, or extrapulmonary NEC, including genitourinary origin tumors. The portion presented focuses specifically on epNEC GU patients treated under Regimens B2 and B3.
The trial utilized a BLRM (Bayesian Logistic Regression Model) design for dose escalation, allowing model-based assessment of dose-limiting toxicity probability rather than traditional 3+3 escalation. This is important, as it enables more refined identification of the maximum tolerated dose (MTD) while minimizing patient exposure to subtherapeutic or excessively toxic doses.
Two key step-up dosing regimens were evaluated:
- Regimen B2: Dose levels progressed sequentially (B2.1 → B2.2 → B2.3 → B2.n).
- Regimen B3: Dose levels progressed (B3.1 → B3.2 → B3.n), with escalation building upon the B2 experience.
Importantly, both B2 and B3 included step-up dosing, which is particularly relevant for T-cell engagers, where early cytokine release syndrome (CRS) risk can be mitigated through gradual dose escalation.
All patients received active doses ranging from 90–1080 µg/kg. The infusion schedule evolved as follows:
- Intravenous weekly (IV qw)
- Then IV weekly for 6 weeks followed by every 3 weeks (q3w)
This transition from intensive weekly induction to maintenance-style dosing reflects an attempt to balance immune activation with long-term tolerability.
The primary endpoints in this phase I study were:
- Maximum tolerated dose (MTD)
- Dose-limiting toxicities (DLTs) during the MTD evaluation period
This confirms the study was fundamentally safety-driven in early phases, with efficacy as a secondary signal.
The secondary endpoints included:
- Objective response rate (RECIST v1.1)
- Pharmacokinetic parameters
This dual emphasis is important because T-cell engagers often demonstrate exposure-response relationships that inform optimal dosing.

A total of 20 patients with epNEC of GU origin were included, divided into DLL3-high (n=12) and DLL3-low (n=8) cohorts. The table summarizing baseline characteristics shows that the two subgroups were largely balanced, minimizing confounding from clinical heterogeneity.
The median age across the cohort was 69 years (range 36–81), with similar ages in DLL3-high (67 years) and DLL3-low (70 years) groups. Eighty percent of patients were male. ECOG performance status was favorable overall, with 30% ECOG 0 and 65% ECOG 1, reflecting a population fit enough to tolerate immunotherapy.
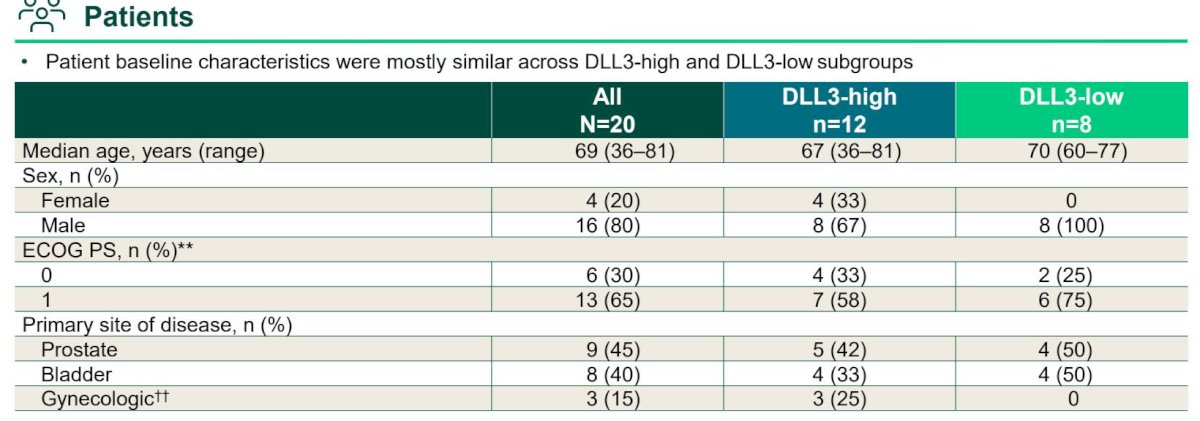
The primary sites were well distributed: prostate (45%), bladder (40%), and gynecologic (15%). Importantly, responses were not restricted to a single GU primary, allowing for cross-site interpretation of activity.
Efficacy OutcomesThe efficacy table demonstrates a striking signal driven entirely by DLL3-high tumors.
The confirmed objective response rate (ORR) was:
- 30% overall (6/20; 95% CI 15–52%)
- 50% in DLL3-high tumors (6/12; 95% CI 25–75%)
- 0% in DLL3-low tumors
This sharp dichotomy reinforces DLL3 expression as a predictive biomarker.

The disease control rate (DCR) further emphasizes the biological separation:
- 55% overall
- 75% in DLL3-high
- 25% in DLL3-low
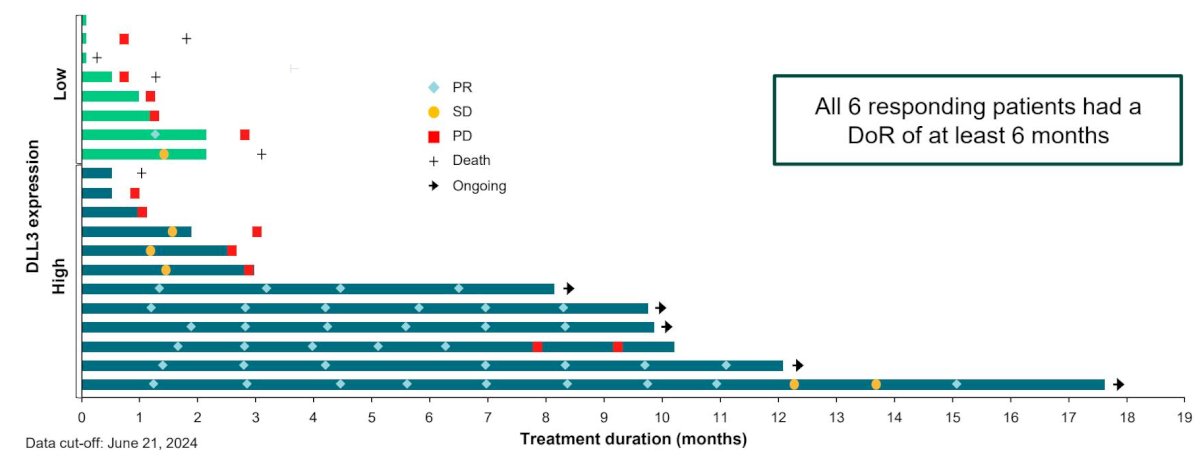
The median duration of response was 6 months overall, and all responding patients had responses lasting at least 6 months. Notably, 5 of 6 responding DLL3-high patients (83%) remained on treatment at data cutoff, suggesting durability beyond the median.
The waterfall plot provides critical visual confirmation of this biomarker effect. Deep tumor regressions are almost exclusively confined to DLL3-high patients, with several patients demonstrating substantial reductions in tumor burden. DLL3-low patients largely show stable disease or progression. The clustering of partial responses within the DLL3-high cohort is visually compelling.
The site-specific donut charts further reinforce that activity was observed across GU primaries when DLL3 expression was high:
- Prostate (DLL3-high): ORR 50%, DCR 83%
- Bladder (DLL3-high): ORR 75%, DCR 75%
- Gynecologic (DLL3-high): ORR 67%, DCR 67%
This suggests that DLL3 expression, rather than tumor origin, is the dominant predictor of response.

The swimmer plot and treatment duration graph show several DLL3-high patients remaining on therapy beyond 10–15 months, highlighting the durability of benefit.
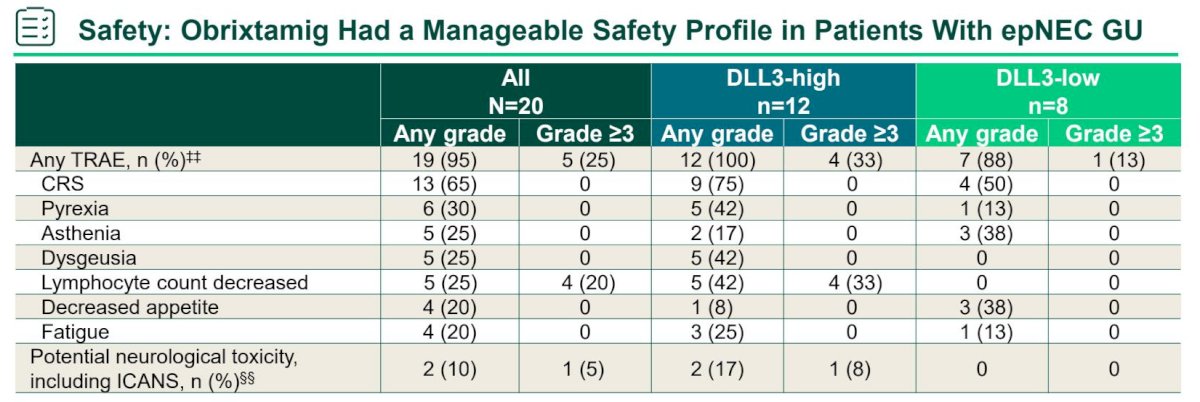
Safety ProfileThe safety table demonstrates a manageable toxicity profile. Grade ≥3 treatment-related adverse events occurred in 20% of patients overall (12% DLL3-high; 38% DLL3-low). The most common adverse events were immune-mediated and cytokine-related, consistent with T-cell engager biology.
Any-grade adverse events included:
- Cytokine release syndrome (CRS): 65%
- Pyrexia: 65%
- Asthenia: 25%
- Fatigue: 20%
- Lymphocyte count decreased: 25%
- Decreased neutrophil count: 20%
Importantly, all CRS events were grade 1–2, with no grade ≥3 CRS observed. Neurologic toxicity, including ICANS, was uncommon and low grade. The frequency of neurologic toxicity was low, supporting tolerability.
The absence of high-grade CRS or ICANS distinguishes obrixtamig favorably from some other T-cell–redirecting platforms.
Dr. Nil Navarro-Gorro concluded as follows:
- Obrixtamig monotherapy showed a manageable safety profile in patients with epNEC GU
- Obrixtamig showed encouraging and durable responses in heavily pretreated patients with DLL3-high epNEC GU
- The ORR of 50% is promising in the context of typical response rates with chemotherapy in this setting (~10-25%)
- An ongoing Phase II trial (DAREON®-5) is assessing obrixtamig in patients with relapsed/refractory DLL3-high epNEC, including those of a GU origin
- Obrixtamig has been granted Orphan Drug Designation (from EMA and FDA) and Fast Track designation (from FDA) for epNEC, highlighting its strong potential as a targeted therapy in an area of high unmet need
Presented by: Nil Navarro-Gorro, MD, Medical Oncology Department, Hospital del Mar, Barcelona, Spain
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
Related content: Obrixtamib Monotherapy Assessed in DLL3-Selected Extrapulmonary Neuroendocrine Tumors - Nil Navarro-Gorro
References:
- Stumpo S, Navarro-Gorro N, Capdevila J, et al. Delta-like ligand 3 (DLL3) expression in extrapulmonary neuroendocrine carcinomas and its potential as a therapeutic target. J Clin Med. 2023;12:7715.
- Weaver J, Wolf J, Wermke M, et al. DLL3 as a therapeutic target in neuroendocrine carcinomas: biological rationale and clinical implications. Cancers (Basel). 2023;15:4951.
- Lozada R, Wermke M, Capdevila J, et al. Targeting DLL3 in neuroendocrine malignancies: emerging strategies and clinical development. Cancer Res Commun. 2025;5:318–326.
- Yao J, Capdevila J, Wermke M, et al. Clinical landscape and unmet needs in extrapulmonary neuroendocrine carcinoma. Oncologist. 2022;27:940–951.
- Matsuo K, Wermke M, Wolf J, et al. Preclinical characterization of DLL3-directed T-cell engager therapy in neuroendocrine carcinoma models. Cancer Sci. 2021;112:2984–2992.
- Wermke M, Wolf J, Capdevila J, et al. Phase I study of obrixtamig, a DLL3/CD3 bispecific T-cell engager, in relapsed/refractory neuroendocrine carcinomas. J Clin Oncol. 2025;43:3021–3031.
- Capdevila J, Wermke M, Wolf J, et al. Efficacy and safety of obrixtamig in patients with DLL3-positive neuroendocrine carcinomas: results from a phase I study. J Clin Oncol. 2025;43(Suppl 16):3004.