(UroToday.com) The 2026 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Fred Saad discussing dose-escalation results of the phase 1 PAnTHA study assessing a first-in-human assessment of 225Ac-PSMA-Trillium (BAY 3563254) in metastatic castration resistant prostate cancer (mCRPC).
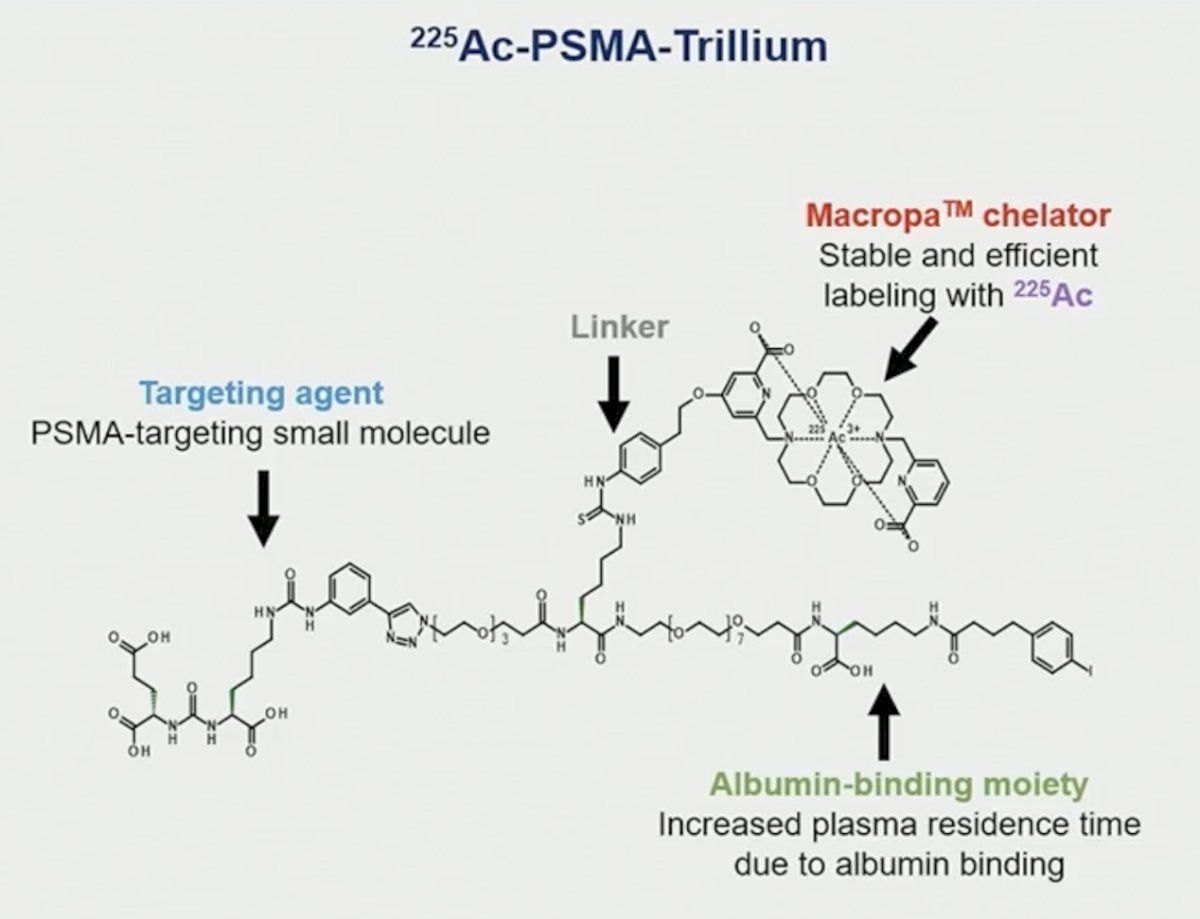
There is proven tolerability and efficacy of radium-223 and 177Lu-PSMA-617 in mCRPC, which provides a rationale for developing alpha-emitting PSMA targeting agents. Compared with beta particles, alpha particles have significantly higher linear energy transfer, thus requiring fewer radiation events or “hits” to achieve a cytotoxic effect. Additionally, they have a shorter penetration range, which means there is potentially less impact on nearby healthy tissues. Dr. Saad and colleagues investigated 225Ac-PSMA-Trillium, a novel PSMA-targeting molecule which comprises a highly specific PSMA-binding motif, an albumin-binding domain to optimize the agent’s pharmacokinetic profile, and a Macropa chelator complexed with the alpha-emitter 225Ac:
At ASCO GU 2026, Dr. Saad presented results of the global, phase 1 PAnTHA (NCT06217822) study, assessing the safety and efficacy of 225Ac-PSMA-Trillium in patients with mCRPC.
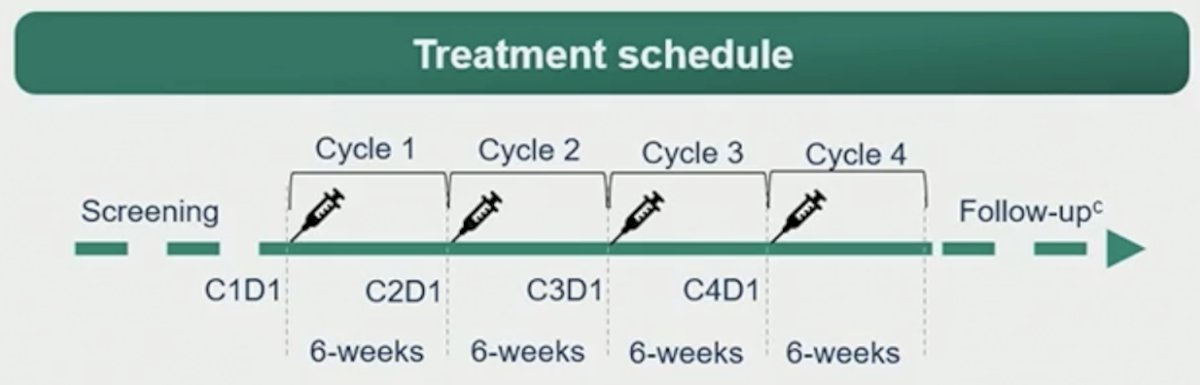
PAnTHA consists of dose-escalation and dose-expansion parts, with the dose-escalation results reported at ASCO GU 2026. Patients had mCRPC with metastases overexpressing PSMA on PET imaging (uptake >liver in ≥1 lesion), ≥1 prior androgen receptor pathway inhibitor, and (if eligible) 1 or 2 prior taxanes, and no prior radiopharmaceutical. 225Ac-PSMA-Trillium was given intravenously every 6 weeks for up to 4 doses:
Dose escalation used a 2-stage joint TITE-CRM design with ≥3 patients per dose level, and ≤9 further patients could be added to any dose level considered tolerable with evidence of antitumor activity.
The dose-escalation primary objectives were to determine the safety, tolerability, and recommended dose for expansion of 225Ac-PSMA-Trillium. Dose-limiting toxicities were assessed in cycles 1–3, and exploratory analyses included baseline PSMA PET SUVmean and longitudinal ctDNA.
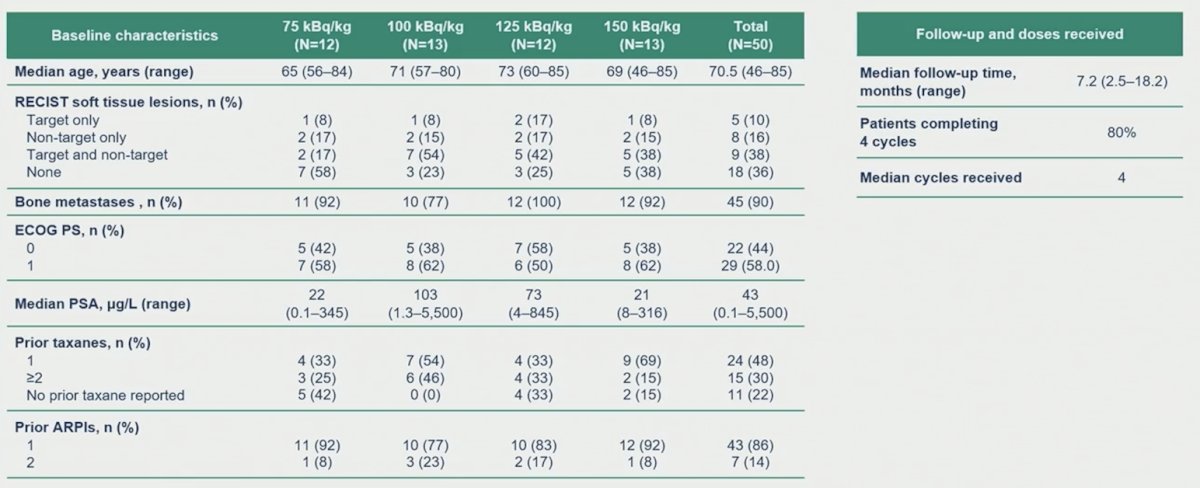
At the data cut-off (September 18, 2025), 50 patients had received ≥1 dose of 225Ac-PSMA-Trillium (range: 75 to 150 kBq/kg; 12–13 patients/cohort). The median age was 70.5 years (range: 46-85), 90% had bone metastases, 48% had measurable disease, 48% and 30% had received 1 or 2 prior taxanes, respectively, and all received ≥1 prior androgen receptor pathway inhibitor:
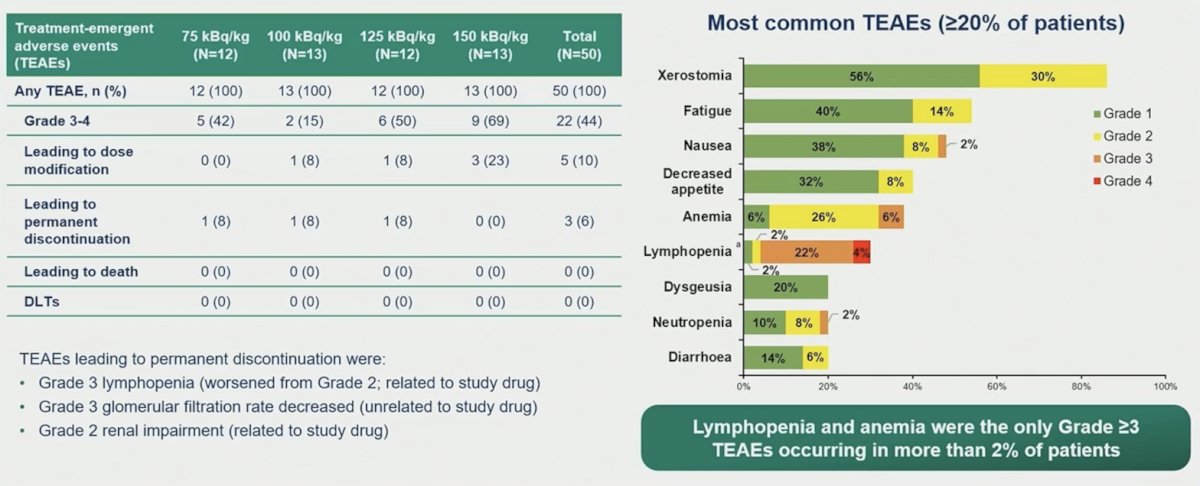
There were no dose-limiting toxicities or treatment-related deaths. Treatment emergent adverse events occurred in 100% of patients, most commonly dry mouth (86%; 56% grade 1, 30% grade 2, 0 grade ≥3). Other common treatment emergent adverse events were fatigue (54%) and nausea (48%). Overall, 44% had grade ≥3 treatment emergent adverse events, most commonly lymphopenia (20%), 16% had serious treatment emergent adverse events, and 6% discontinued treatment due to treatment emergent adverse events:
The overall response rate per PCWG3 criteria across all doses in patients with measurable disease at baseline was 42%, and the disease control rate was 79%. In the 125 kBq/kg dose (n = 12), the PSA50 rate was 83%, and the PSA90 rate was 67%:
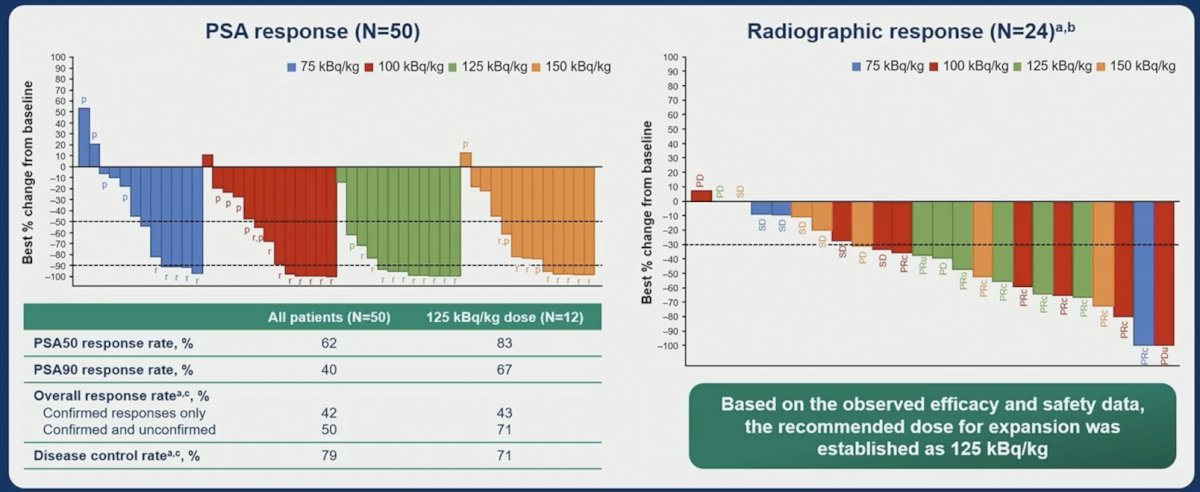
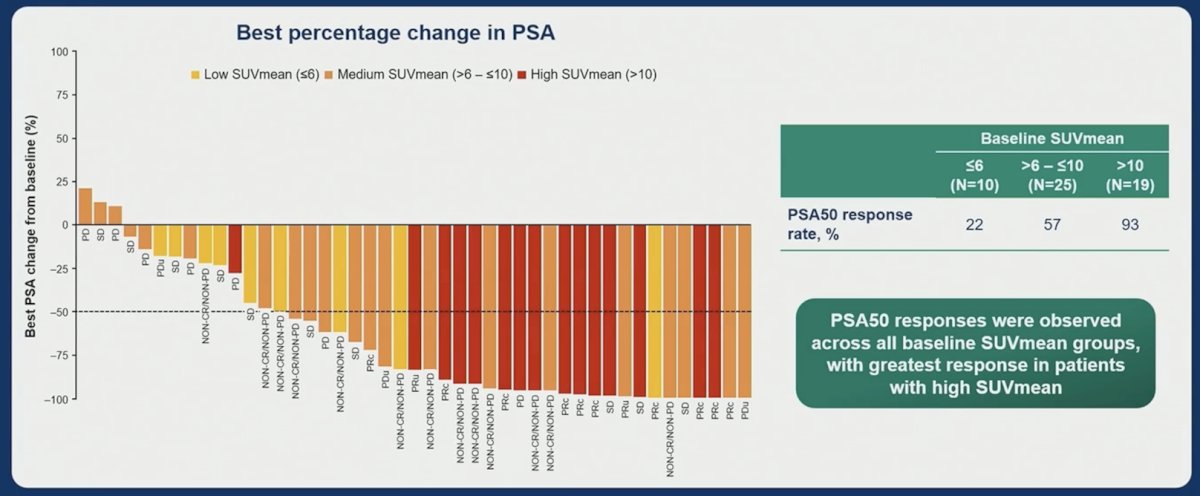
Based on safety and preliminary antitumor activity data, 125 kBq/kg was selected as the recommended dose for expansion. PSA responses were seen in 93% of patients with high PSMA expression at baseline (SUVmean >10):
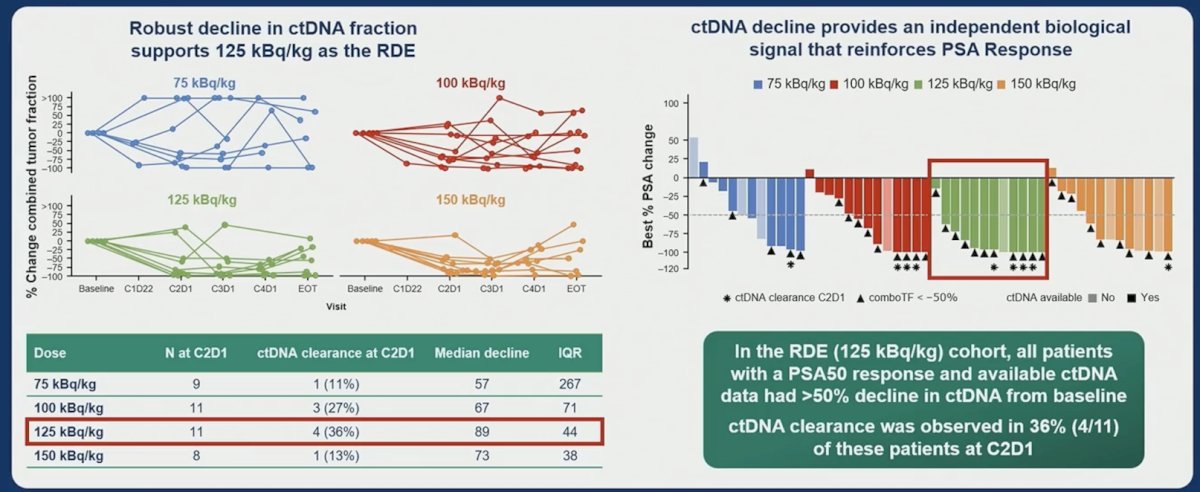
A dose-dependent trend in ctDNA clearance was seen up to the recommended dose for expansion by the start of the second cycle:
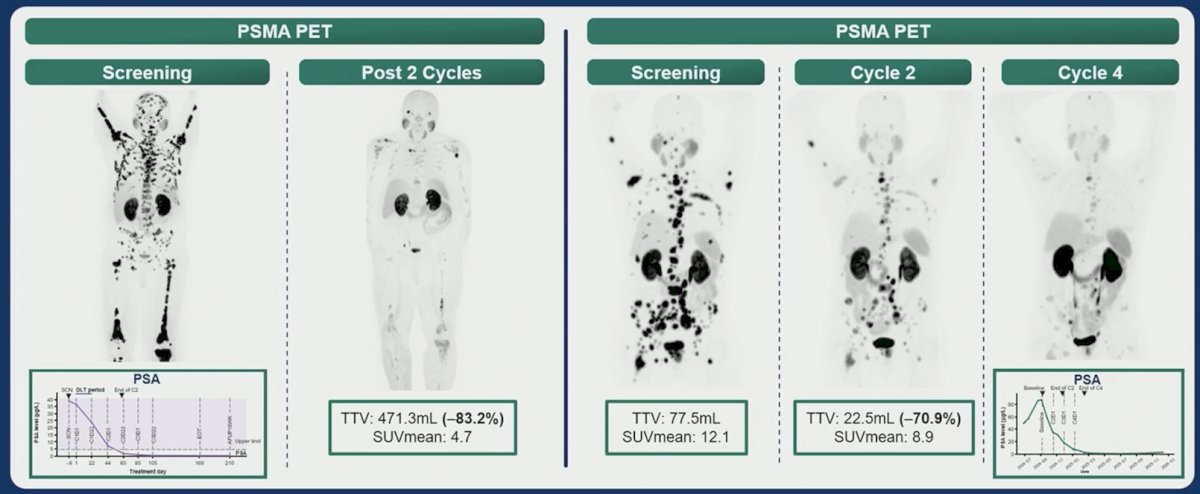
The following highlights two patient cases demonstrating impressive responses, even after only two cycles of 225Ac-PSMA-Trillium:
Dr. Saad concluded his presentation discussing dose-escalation results of the phase 1 PAnTHA study with the following take-home points:
- 225Ac-PSMA-Trillium was well-tolerated with no dose-limiting toxicities or grade 3 xerostomia
- For patients with measurable disease, the objective response was 50%, with 62% of patients having a PSA50 response, and 93% for patients with high PSMA expression
- Based on the safety and efficacy, the recommended dose for expansion will be 125 kBq/kg, and at this dose, the objective response rate was 71%, and the PSA50 response rate was 83%
- The dose expansion part of the study is currently ongoing and is assessing the recommended dose for expansion in three cohorts: post-chemotherapy, prior to chemotherapy, and post 177Lu-PSMA-617
- Findings from the PAnTHA phase 1 study will inform the phase 3 trial in patients with mCRPC
Presented by: Fred Saad, CQ, MD, FRCS, FCAHS, Professor, Department of Surgery, Raymond Garneau Chair in Prostate Cancer, Director of Prostate Cancer Research, Director of GU Oncology, Université de Montréal, University of Montreal Hospital Centers, CRCHUM, Montréal, QC
Related content: Phase I PAnTHA Study Evaluates PSMA-Targeted Actinium-225 in mCRPC Patients - Fred Saad