(UroToday.com) The 2026 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Johann S. De Bono discussing preliminary phase 1 dose escalation results of VIR-5500 (AMX-500), a dual masked PRO-XTEN T-cell engager, in metastatic castration resistant prostate cancer (mCRPC).
VIR-5500 is designed to be specifically activated in the tumor microenvironment where protease activity is dysregulated relative to healthy tissues, potentially expanding the safety margin and therapeutic index. In this phase 1 study, VIR-5500 was administered IV weekly (QW) and every 3 weeks (Q3W) at doses of 30 - 4000 ug/kg to eligible participants with progressive mCRPC after receiving standard of care:

The objectives were to characterize safety, pharmacokinetics profiles, anti-tumor activity, and determine the dose(s)/regimen(s) for expansion (NCT05997615).
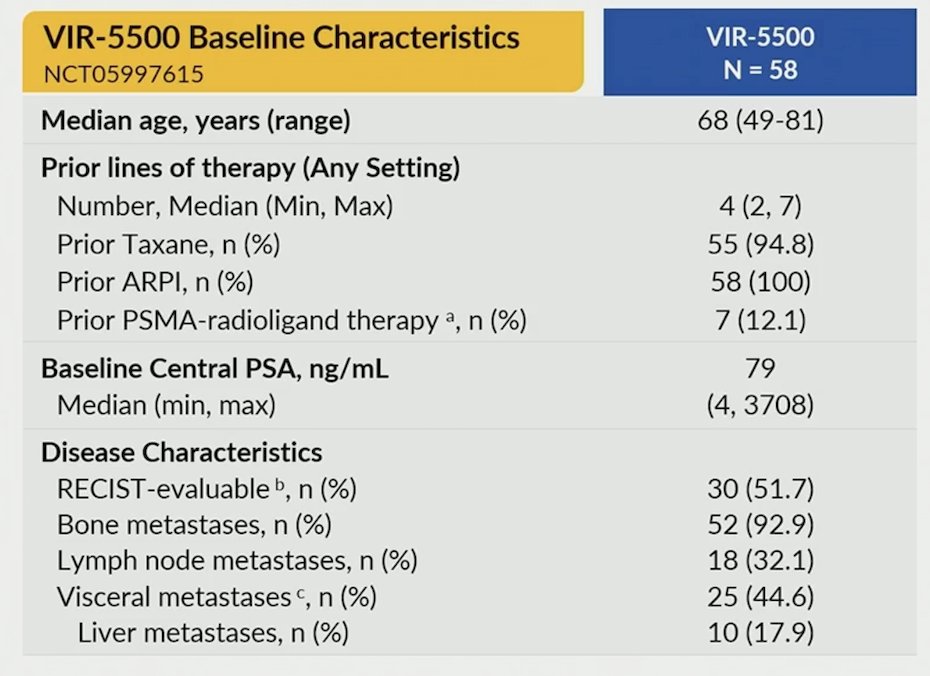
As of January 9, 2026, 58 heavily pretreated mCRPC participants (94.8% post-taxane) received ≥ 1 dose of VIR-5500. These were heavily pre-treated patients, with a median 4 prior lines of therapy:
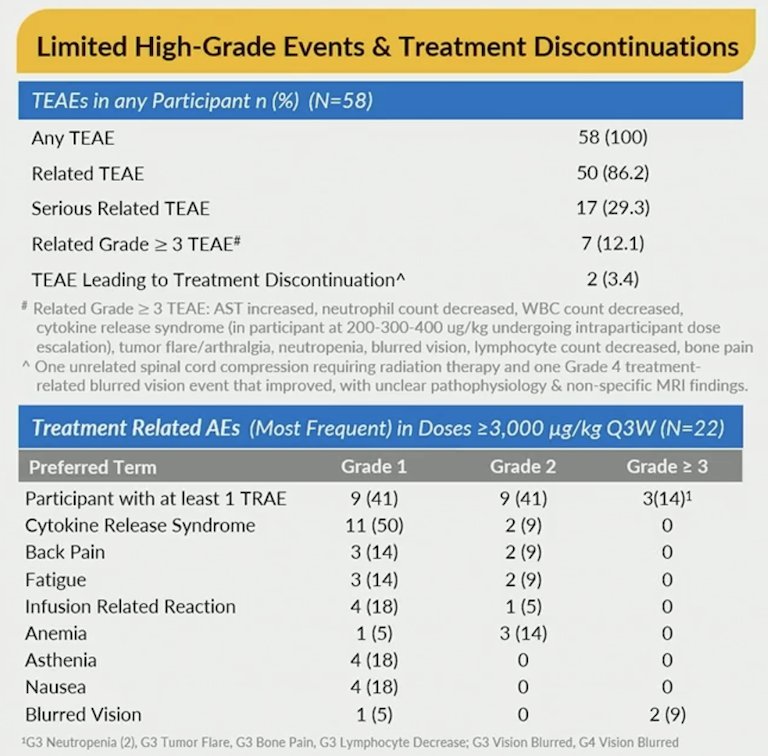
There were no dose-limiting toxicities (pre-defined toxicities occurring during cycle 1) reported. The incidence of related grade ≥ 3 adverse events was 12% and cytokine release syndrome was mostly limited to grade 1 and 2:
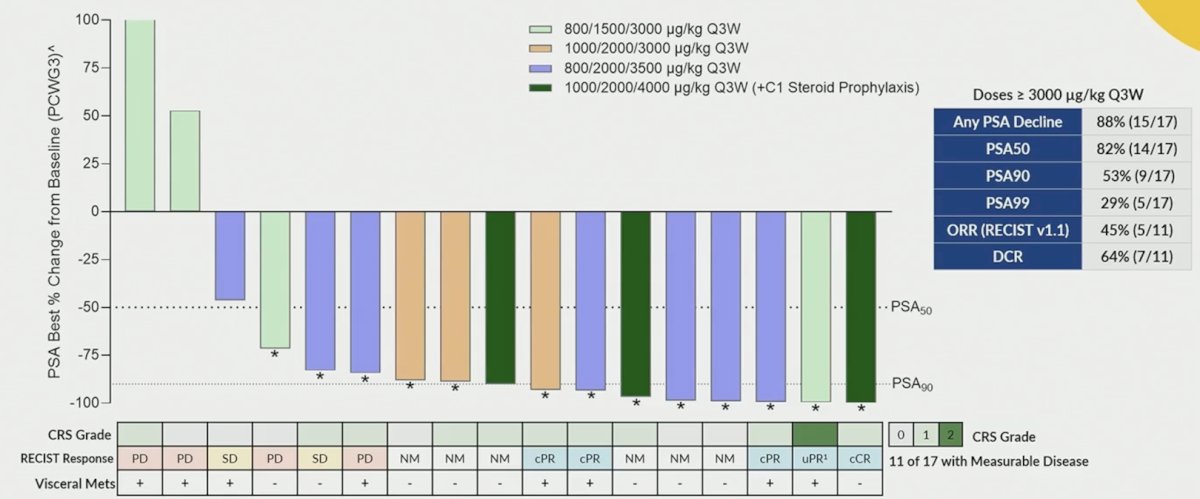
PSA declines were noted in all participants dosed at ≥ 3000 ug/kg Q3W, including clinically significant and deep PSA reductions (82% PSA50 and 53% PSA90). Preliminary evidence of durable PSA responses lasting over one year was noted in select patients undergoing intra-patient dose escalation. An objective response rate of 45% was observed in 5 out of 11 RECIST-evaluable patients treated at doses ≥ 3000 µg/kg Q3W:
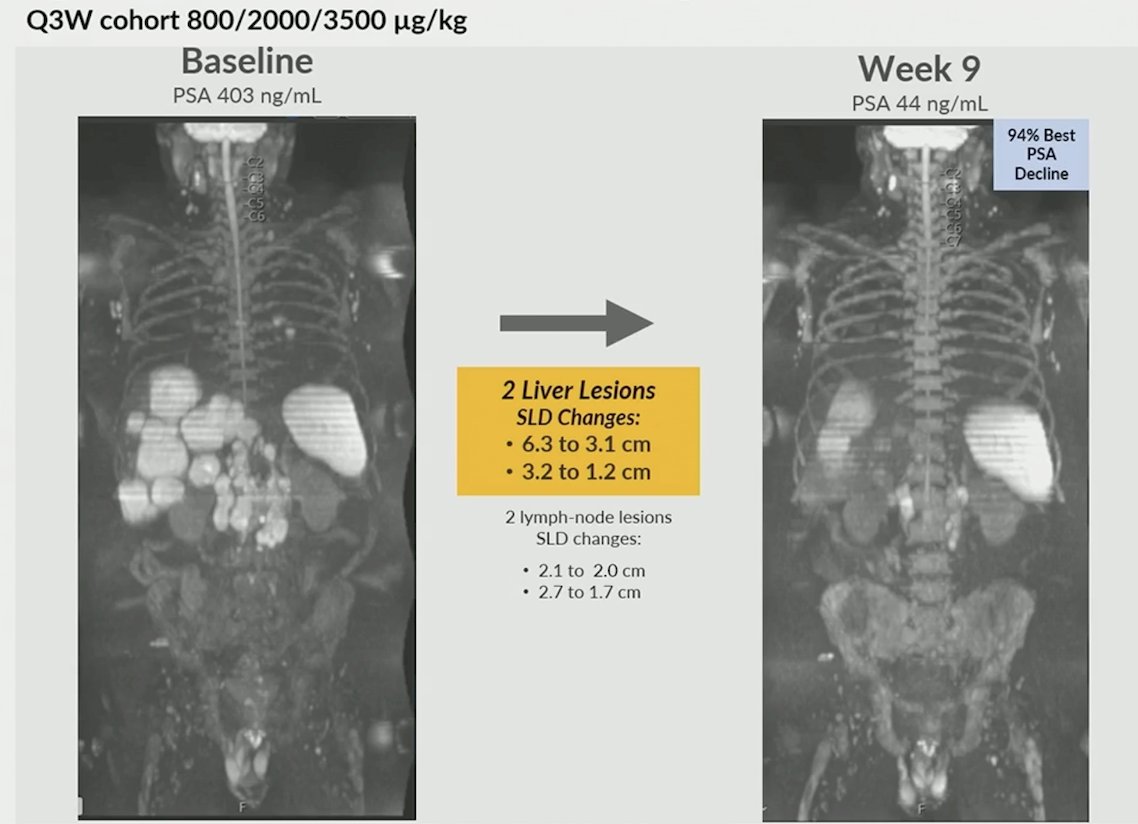
Dr. De Bono then provided two cases to highlight the clinical efficacy of VIR-5500. The first patient was a 75-year-old male with a high disease burden comprising liver and lymph node metastases. He had received 6 prior lines of therapy, including enzalutamide, docetaxel, cabazitaxel, and NX-1607. At week 9, he had a confirmed partial response, with a 94% PSA decline and metabolic response of PSMA-avid hepatic lesions. He continues on study and is on cycle 10 of therapy:
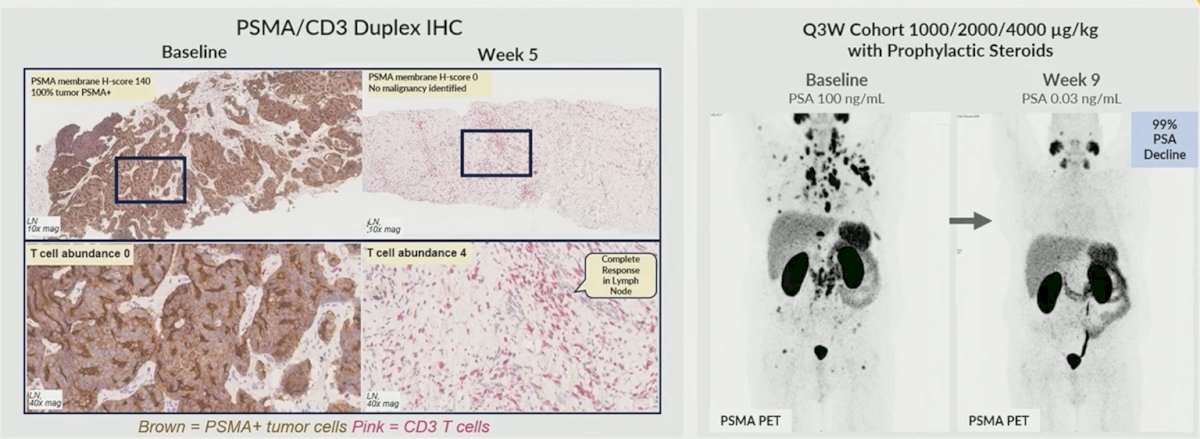
The second patient was a 63-year-old male with lymph node and bone lesions, who had received 5 prior lines of therapy, including enzalutamide, docetaxel, TAS AR antagonist, and radioligand therapy (225Ac-pelgifatamab). The patient had a complete response of target lesions and a non-complete response/non-progressive disease for non-target bone lesions. He also had a PSA99 response at cycle 2 day 1 (week 4). Importantly, he had an excellent quality of life, with a significant reduction in pain. The patient withdrew from the study on cycle 5, while in remission and deriving significant benefit:
Dr. De Bono concluded his presentation discussing preliminary phase 1 dose escalation results of VIR-5500 (AMX-500) in mCRPC with the following take-home points:
- This phase 1 study of VIR-5500 supports proof of concept for PRO-XTEN® masking technology, largely abrogating cytokine release syndrome toxicity that is primarily limited to grade 1 (fever only)
- The treatment was well tolerated with no dose-limiting toxicities
- There was a low rate of ≥ grade 3 treatment-related adverse events without prophylactic corticosteroids or anti-IL-6 at doses up to 3500 µg/kg Q3W
- Rapid and deep PSA declines (53% PSA90) were noted at higher doses with VIR-5500 monotherapy
- There was an objective response rate of 45%, and all 4 evaluable responders achieved confirmation at doses ≥3000 µg/kg Q3W
- There is emerging evidence of durable disease regression, most notable in the highest dose cohorts, but acknowledging limited follow-up
Presented by: Johann De Bono, MD, MSc, PhD, FRCP, The Institute of Cancer Research and the Royal Marsden NHS Foundation Trust, London, UK