(UroToday.com) The 2026 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Xiao Wei discussing the real-world effectiveness of systemic therapies after 177Lu-PSMA-617 treatment in patients with metastatic castration resistant prostate cancer (mCRPC). mCRCP is one of the most advanced forms of prostate cancer and is associated with poor outcomes, with most patients dying within 2-4 years.
In March 2025, the indication for 177Lu-PSMA-617 was expanded to include PSMA-positive patients with mCRPC treated with ≥1 androgen receptor pathway inhibitor and considered appropriate to delay taxane-based chemotherapy. With 177Lu-PSMA-617 moving earlier in the treatment journey, it is important to understand the clinical activity of other systemic therapies after 177Lu-PSMA-617. The aim of this study was to evaluate the clinical outcomes among patients with mCRPC receiving systemic therapy after 177Lu-PSMA-617 treatment.
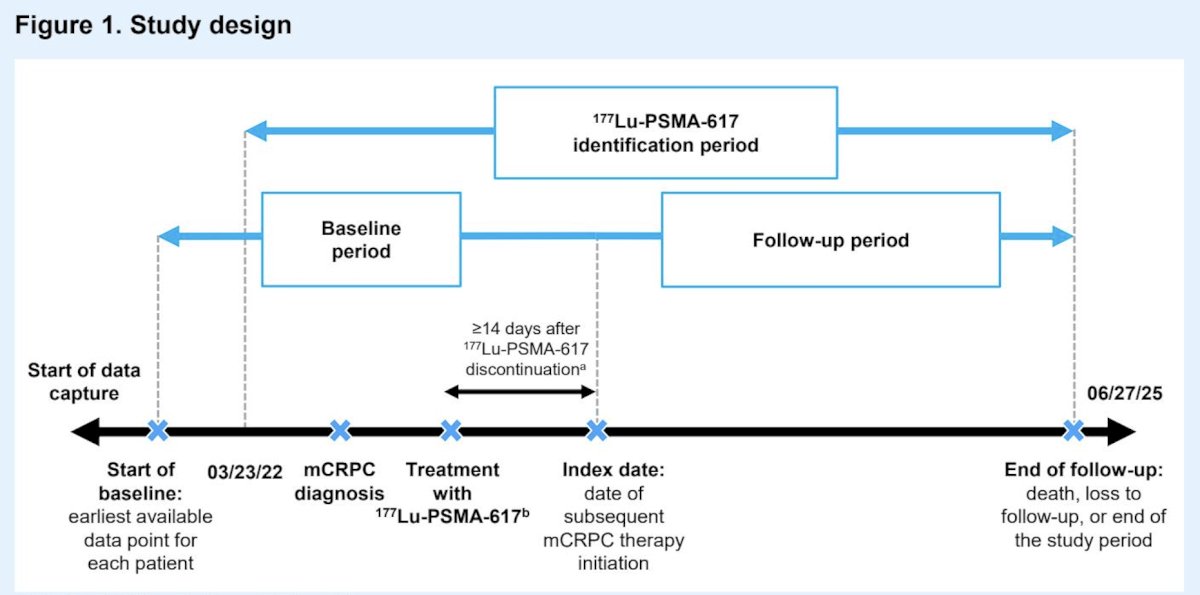
This retrospective, observational study used real-world data from the PRECISION data platform, a proprietary dataset developed by Novartis representing patients with advanced prostate cancer in the US from diverse clinical settings. Patients with mCRPC treated with 177Lu-PSMA-617 who received a systemic therapy ≥14 days after treatment with 177Lu-PSMA-617 between March 23, 2022, and June 27, 2025, were included:
Systemic therapies included androgen receptor pathway inhibitors (abiraterone, enzalutamide, darolutamide, apalutamide), chemotherapy (cabazitaxel, docetaxel, carboplatin, cisplatin, etoposide, mitoxantrone), immunotherapy (pembrolizumab, sipuleucel-T), PARP inhibitors (niraparib, olaparib, talazoparib, rucaparib), and radium-223. Patient characteristics and PSA response were evaluated descriptively, and progression-free survival from subsequent therapy initiation was estimated using Kaplan–Meier methodology.
A total of 442 patients receiving any subsequent systemic therapy after 177Lu-PSMA-617 were included. The median age was 71.0 years (IQR 65.5-76.0), and the median PSA was 41.8 ng/mL (IQR 9.15-183.83):

The median duration of ¹⁷⁷Lu-PSMA-617 therapy was 206 days (IQR 93–218 days), and the median number of cycles was 4 (IQR 2–6). The duration of ¹⁷⁷Lu-PSMA-617 therapy was slightly shorter among patients with subsequent taxane therapy, but the median number of cycles was the same across all subgroups. Among the entire study population, the median times from prostate cancer and mCRPC diagnosis to ¹⁷⁷Lu-PSMA-617 initiation were 6.2 years and 2.5 years, respectively, and were similar across subgroups. Overall, >90% of patients had evidence of ≥1 androgen receptor pathway inhibitor prior to ¹⁷⁷Lu-PSMA-617 initiation in all subgroups examined. Among all patients, 24% had no prior taxane experience, which was 31% among patients who started a subsequent androgen receptor pathway inhibitor and 20% among those who started a subsequent taxane. Post-mCRPC diagnosis, most patients (86%) initiated ¹⁷⁷Lu-PSMA-617 in the third line of therapy or later. The median times from the first and last ¹⁷⁷Lu-PSMA-617 cycle to subsequent therapy initiation were 255 days and 70 days, respectively.
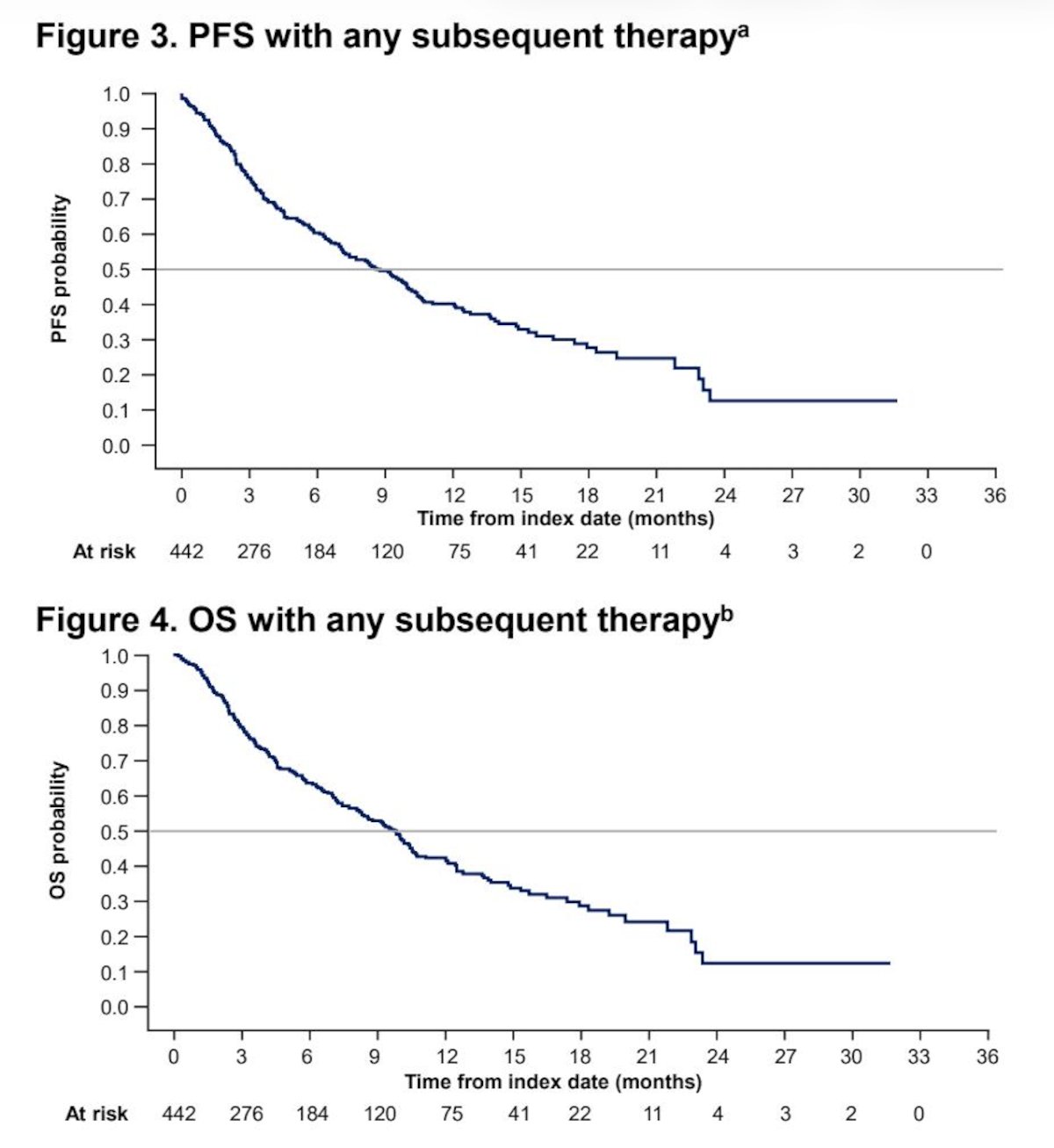
Among 299 patients receiving a systemic therapy after 177Lu-PSMA-617 with PSA values available both preindex and during subsequent treatment, 48% achieved a ≥50% reduction in PSA from baseline (PSA50), 31% a PSA80, and 18% a PSA90. The median progression-free survival from the initiation of subsequent therapy was 8.6 months (95% CI 7.2-10.1) in the entire cohort, and the median overall survival was 9.8 months (95% CI 8.2-10.5) from initiation of subsequent systemic therapy in the overall study population:
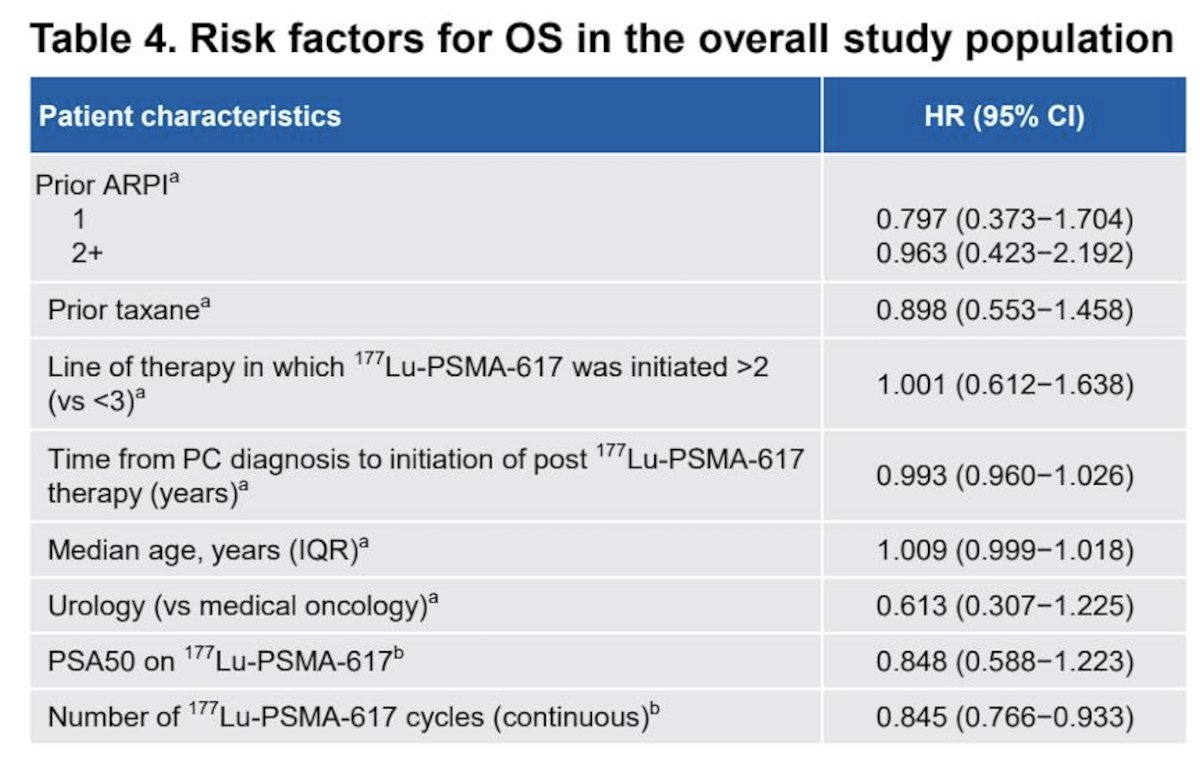
In the multivariable analysis, after adjusting for key baseline characteristics such as age and time from prostate cancer diagnosis to 177Lu-PSMA-617, the only factor significantly associated with better overall survival outcomes from subsequent therapy was increasing the number of 177Lu-PSMA-617 cycles:
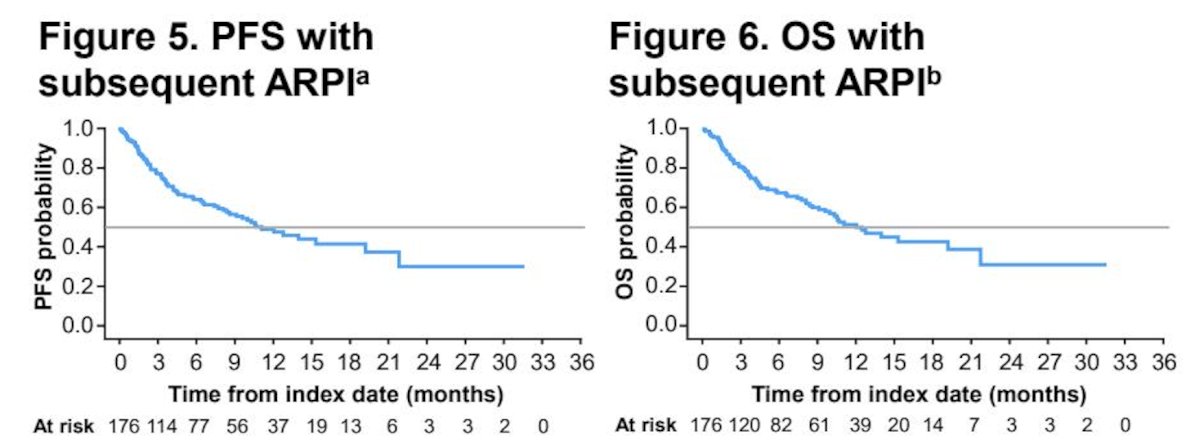
Among 123 patients initiating an androgen receptor pathway inhibitor as subsequent therapy, 52% achieved a PSA50, 33% a PSA80, and 20% a PSA90. The median progression-free survival was 10.7 months (95% CI 8.1-19.3), and the median overall survival was 12.5 months (95% CI 9.6-21.8) among patients receiving a subsequent androgen receptor pathway inhibitor:
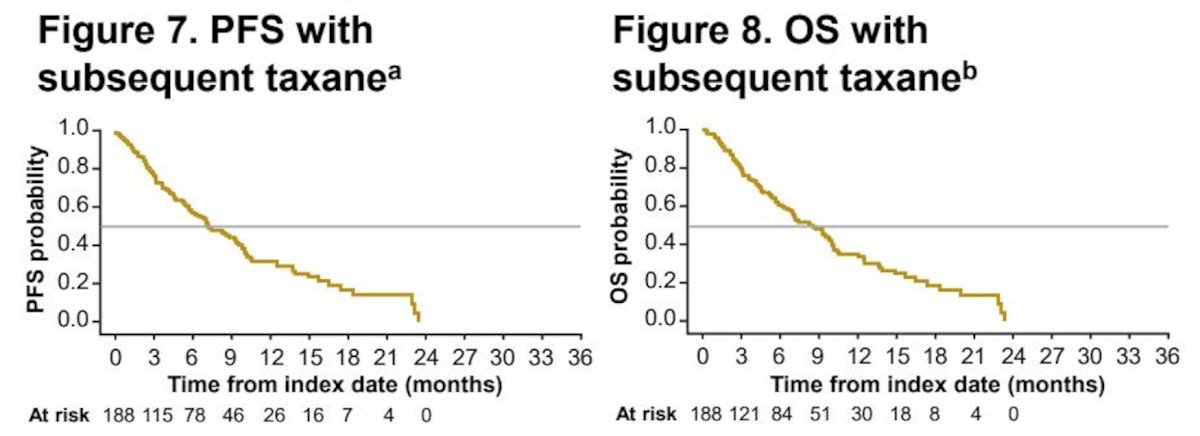
Among 127 patients initiating a taxane as subsequent therapy, 41% achieved a PSA50, 26% a PSA80, and 13% a PSA90. The median progression-free survival was 7.2 months (95% CI 5.9-9.4), and the median overall survival was 8.3 months (95% CI 6.6-10.0) among patients treated with a subsequent taxane:
Dr. Wei concluded her presentation discussing the real-world effectiveness of systemic therapies after 177Lu-PSMA-617 treatment in patients with mCRPC with the following take-home points:
- In this real-world analysis, meaningful clinical responses were observed in patients who received subsequent systemic therapy following discontinuation of ¹⁷⁷Lu-PSMA-617
- Among patients initiating a subsequent therapy, PSA50 responses were observed in 48%, PSA80 in 31%, and PSA90 in 18%
- The median progression-free survival was 9 months from initiation of subsequent therapy overall, which was 11 months in patients treated with a subsequent androgen receptor pathway inhibitor and 7 months in those treated with a subsequent taxane
- The median overall survival was 10 months overall, 13 months with subsequent androgen receptor pathway inhibitor, and 8 months with subsequent taxane. Patient selection may account for differences in outcomes between cohorts
- Interestingly, a higher number of ¹⁷⁷Lu-PSMA-617 cycles was associated with a lower risk of death following initiation of subsequent therapy
- Overall, these results suggest that ¹⁷⁷Lu-PSMA-617 treatment does not preclude response to other subsequent systemic therapies; however, longer follow-up is needed. The optimal patient selection and sequencing of therapies remain important challenges to maximize clinical benefit
Presented by: Xiao X. Wei, MD, MAS, Lank Center for Genitourinary Oncology, Dana-Farber Cancer Institute, Boston, MA
Related content: Real-World Data Explores Post-177Lu-PSMA-617 Therapies in Advanced Prostate Cancer - Xiao Wei