(UroToday.com) The 2026 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Daniel George discussing real-world outcomes of 177Lu-PSMA-617 in taxane-naïve patients with metastatic castration resistant prostate cancer (mCRPC). mCRPC represents an advanced stage of prostate cancer and is associated with a poor prognosis, with only 15% of patients with mCRPC surviving beyond 5 years.
In the PSMAfore clinical trial,1 177Lu-PSMA-617 achieved a PSA50 (defined as a ≥50% reduction in PSA from baseline) response rate in 58%, a median radiographic progression-free survival of 12 months, and a median overall survival of 25 months among taxane-naïve patients with mCRPC who had received one prior androgen receptor pathway inhibitor. The aim of the present study was to evaluate the real-world effectiveness of 177LuPSMA-617 in taxane-naïve patients with mCRPC who had received one or more prior androgen receptor pathway inhibitors.
This retrospective, observational study included taxane-naïve adults with mCRPC initiating 177Lu-PSMA-617 between March 23, 2022, and June 27, 2025, after ≥1 prior androgen receptor pathway inhibitor:
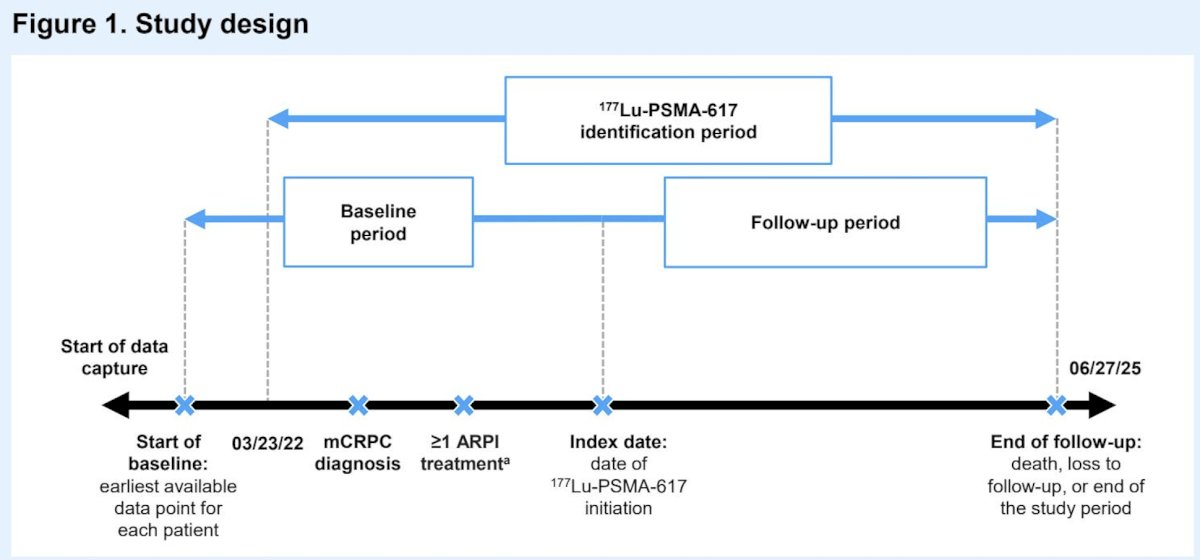
All data for the study were extracted from the PRECISION data platform, a harmonized dataset of patients with advanced prostate cancer in the US treated in a variety of clinical settings. The index date was the date of 177Lu-PSMA-617 initiation. Patient characteristics and PSA response rates were evaluated descriptively. Progression free survival, defined as the time from 177Lu-PSMA-617 initiation to progression or death, was estimated using Kaplan–Meier methodology.
A total of 500 patients were included. The median age was 72 years, 75% of patients were White, and 8% Black. Overall, 18% were treated in urology centers while 82% were treated in oncology centers. The most common site of metastasis was bone (77%), followed by lymph node (21%), visceral (12%), and unknown (5%). The median baseline PSA was 26.7 ng/mL (IQR 10−105 ng/mL), and the median time from mCRPC diagnosis to 177Lu-PSMA-617 initiation was 23.6 months:
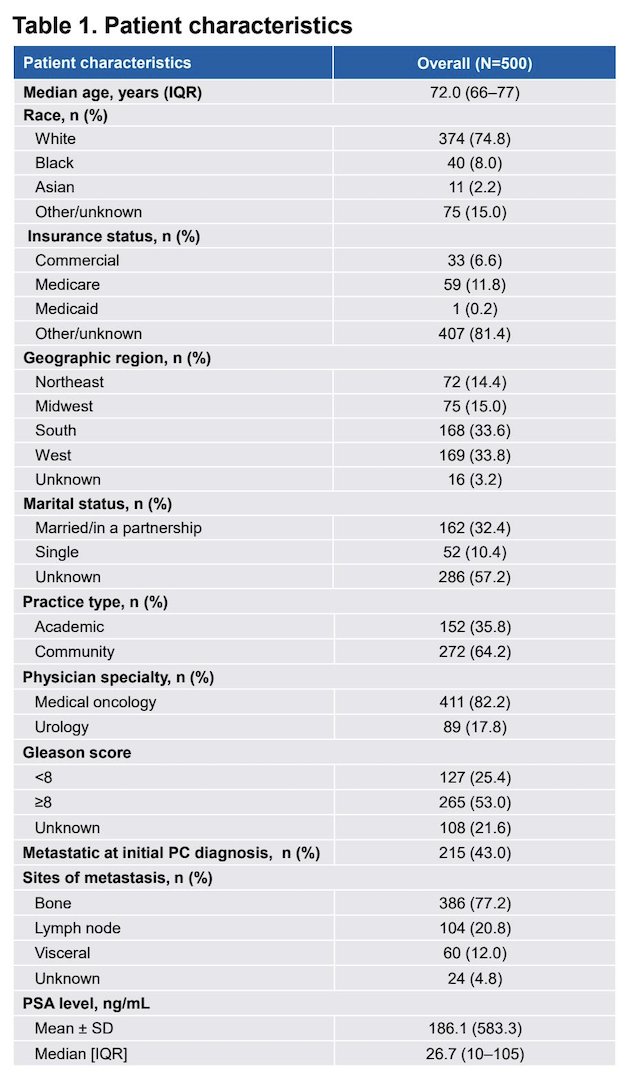
Overall, 51% of patients had received 1 previous androgen receptor pathway inhibitor, while 49% had received >1 androgen receptor pathway inhibitor. The median time from prostate cancer diagnosis to ¹⁷⁷Lu-PSMA-617 initiation was 6.8 years, and from mCRPC diagnosis to ¹⁷⁷Lu-PSMA-617 initiation was 1.9 years. The median duration of ¹⁷⁷Lu-PSMA-617 therapy was 139 days (IQR 45–216 days), and the median number of ¹⁷⁷Lu-PSMA-617 cycles received was 4 (IQR 2–6). The majority of patients (42%) had ¹⁷⁷Lu-PSMA-617 as their third-line therapy post-mCRPC diagnosis.
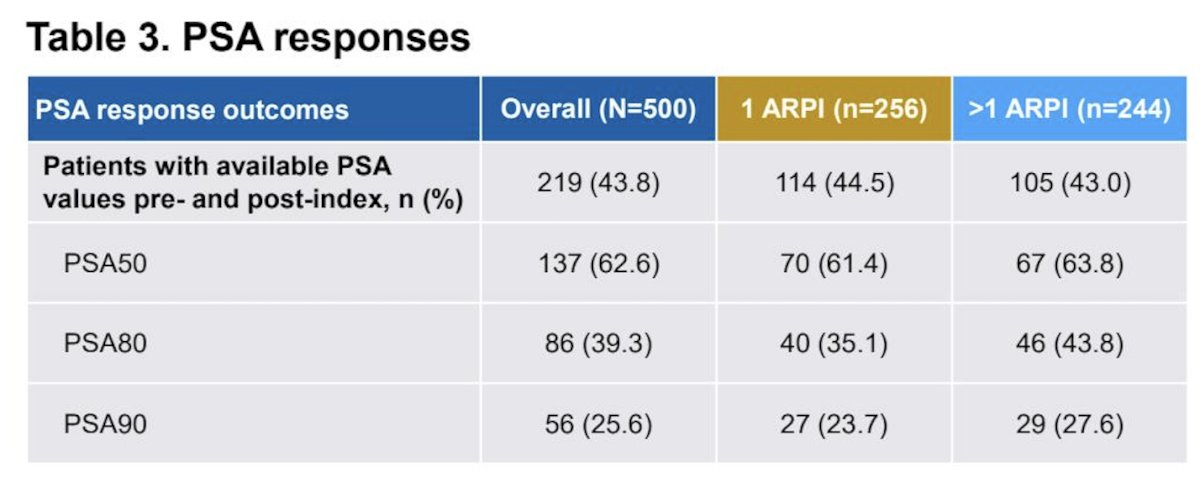
Overall, among 219 patients with available PSA, PSA responses included a PSA50 of 63%, PSA80 of 39%, and PSA90 of 26%. PSA response outcomes were similar, with only 1 or >1 prior androgen receptor pathway inhibitor therapy:
The median progression-free survival in the study was 13.5 months (95% CI 11.7-14.7), which was 15.8 months (95% CI 11.7-18.6) in patients with 1 versus 12.7 months (95% C 10.7-14.0) in those with >1 androgen receptor pathway inhibitor therapy: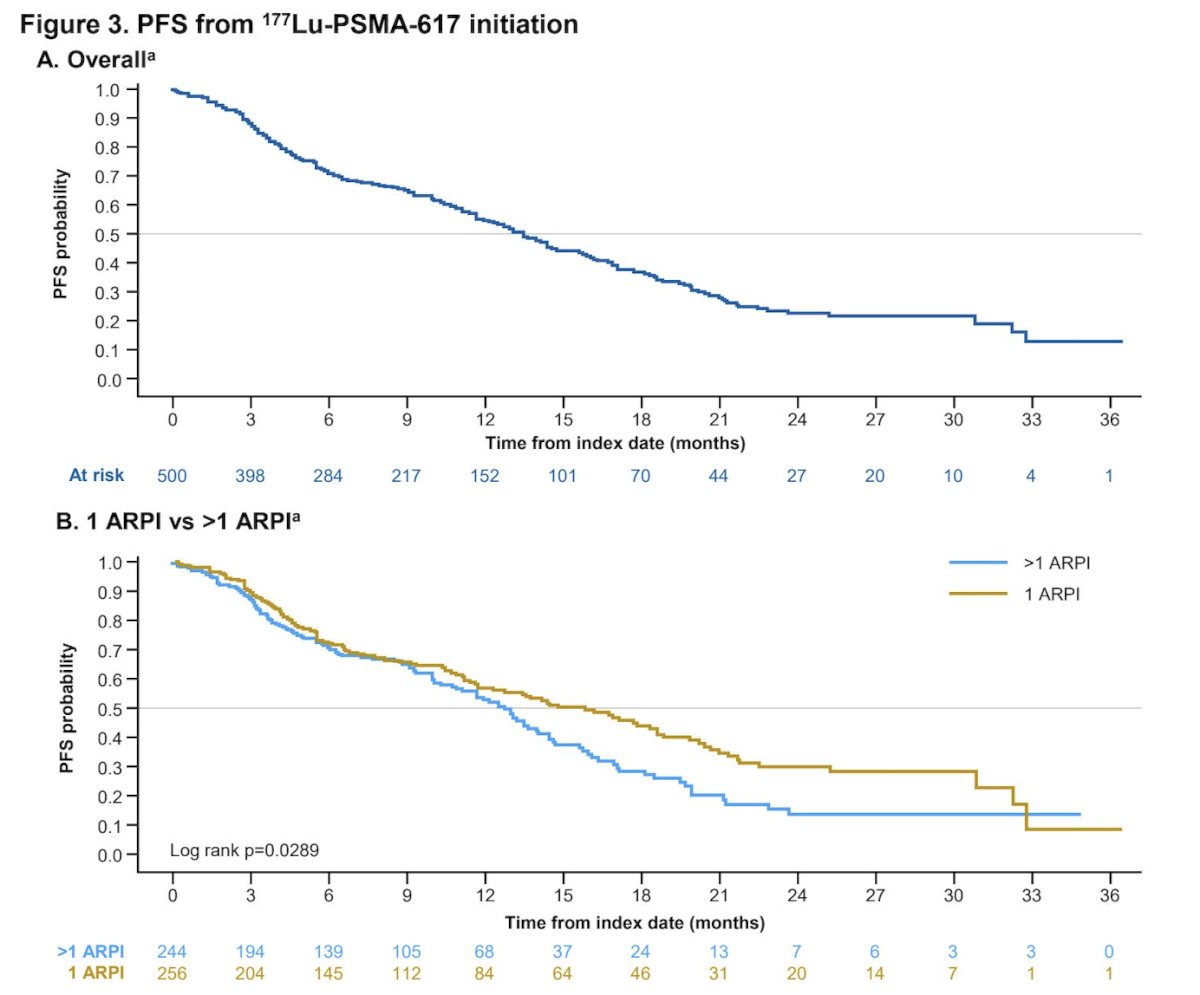
Dr. George concluded his presentation discussing real-world outcomes of 177Lu-PSMA-617 in taxane-naïve patients with mCRPC with the following take-home points:
- In this real-world study of taxane-naïve patients with mCRPC initiating ¹⁷⁷Lu-PSMA-617, approximately half had received 1 prior androgen receptor pathway inhibitor, and half >1 prior androgen receptor pathway inhibitor
- The rate of PSA50 response was 63%, PSA80 was 39%, and PSA90 was 26%, with no notable difference between patients with 1 versus >1 prior androgen receptor pathway inhibitor
- The median PFS was 13.5 months, which was significantly longer in patients with only 1 prior ARPI compared with those with >1 prior androgen receptor pathway inhibitor
- Overall, these results indicate that the effectiveness of ¹⁷⁷Lu-PSMA-617 as a standard-of-care treatment in the real-world for taxane-naïve patients with mCRPC is consistent with the results of the PSMAfore trial, confirming the applicability of those findings to the real-world population now eligible for ¹⁷⁷Lu-PSMA-617
- Prompt initiation in patients treated with 1 prior ARPI showed superior clinical outcomes versus initiation later in their treatment journey. These results may help to guide treatment sequencing in clinical practice
Presented by: Daniel George, MD, Medical Oncologist, Professor, Departments of Medicine and Surgery, Duke Cancer Institute, Duke University, Durham, NC
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 26 – Sat, Feb 28, 2026.
Reference: