(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, was host to the Poster Session A: Prostate Cancer. Dr. Nobuaki Matsubara presented Poster 195: Efficacy and safety of mevrometostat in combination with enzalutamide in patients with mCRPC: Data from a phase 1 study.
Dr. Matsubara highlighted that enhancer of zeste homolog 2 (EZH2) is overexpressed in castration-resistant prostate cancer and plays an oncogenic role in cooperation with the androgen receptor. Mevrometostat (PF-06821497) is an oral, potent, selective small-molecule inhibitor of EZH2, and it is hypothesized that combining an EZH2 inhibitor with an androgen receptor pathway inhibitor may enhance ARPI activity and delay or prevent resistance.
In the randomized dose-expansion portion of a phase 1 study (NCT03460977), mevrometostat 1250 mg twice daily on an empty stomach plus enzalutamide 160 mg once daily improved outcomes compared with enzalutamide alone, with a manageable safety profile in patients with mCRPC. An alternate dosing regimen of mevrometostat 875 mg twice daily, administered with food, demonstrated improved tolerability compared with the higher-dose empty-stomach schedule, while maintaining equivalent drug exposure, supporting further development of the optimized regimen.
Cohort 2A included patients previously treated with abiraterone and/or enzalutamide, while cohort 2C included patients previously treated with abiraterone who were enzalutamide-naïve. All patients had received no more than one prior chemotherapy regimen and had disease progression per modified PCWG3 criteria. The primary endpoints were radiographic progression-free survival (rPFS) and safety, with secondary endpoints including objective response rate (ORR) and PSA50 response.
As of September 1, 2025, 29 patients had been treated (2A, n=15; 2C, n=14). Median age was 74 years in 2A and 73 years in 2C. In cohort 2A, 60% had received prior abiraterone and 60% prior enzalutamide; in cohort 2C, all patients had received prior abiraterone and were enzalutamide-naïve. Patient characteristics are shown below:

Patients enrolled in parts 2A and 2C were heavily pretreated. The median number of prior anticancer regimens was 3.0 (range 2–5) in part 2A and 2.0 (range 1–6) in part 2C. Prior taxane therapy had been received by 60.0% of patients in part 2A and 42.9% in part 2C. In part 2A, 40.0% had previously received abiraterone alone, 40.0% enzalutamide alone, and 20.0% both agents. In contrast, in part 2C, all patients had received prior abiraterone and were enzalutamide-naïve.
The median duration of treatment was 9.0 months (IQR 4.2–17.5) in part 2A and 5.9 months (IQR 4.5–15.9) in part 2C. Individual treatment durations are detailed in the study figures, reflecting sustained exposure in a subset of patients despite prior therapy.
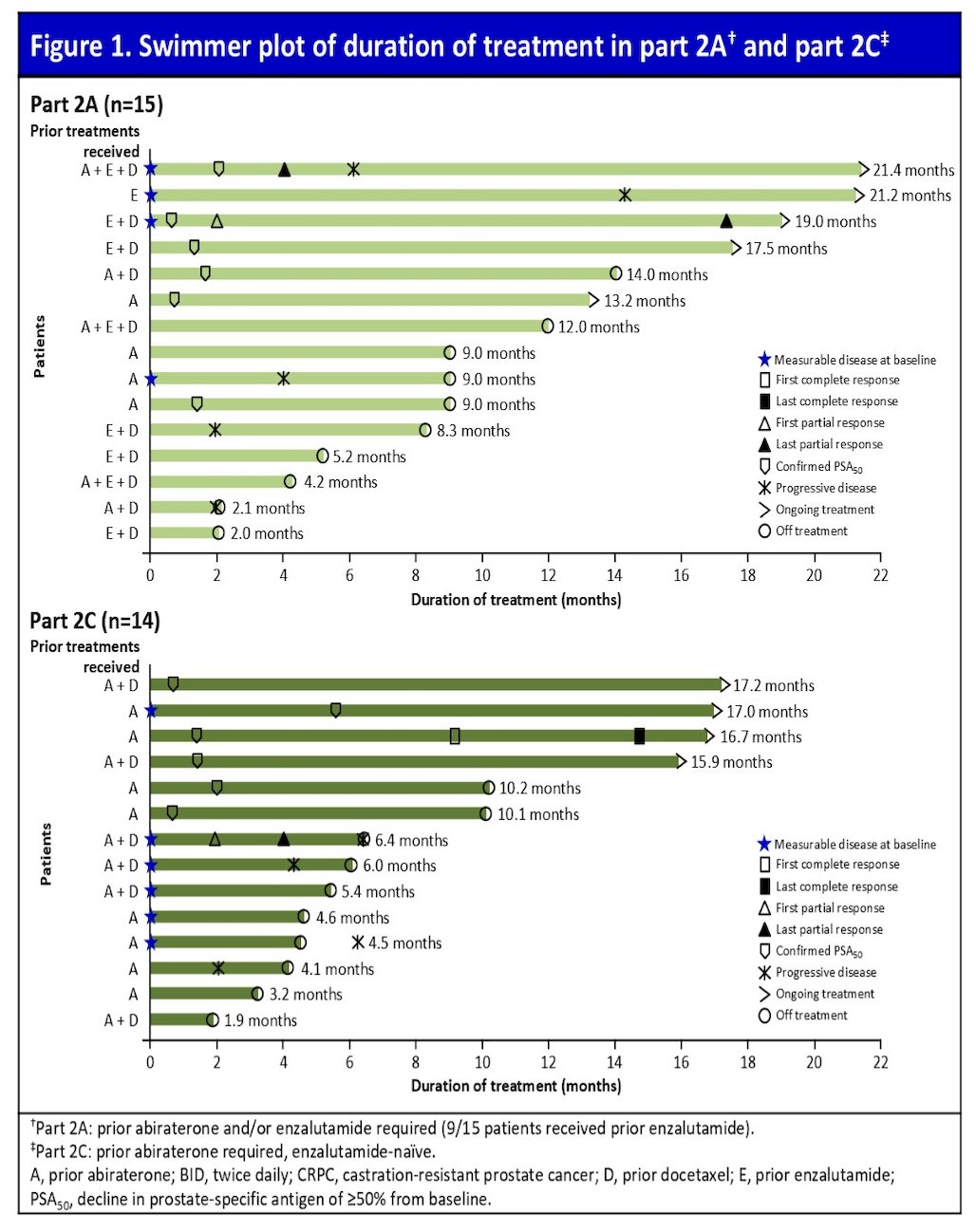
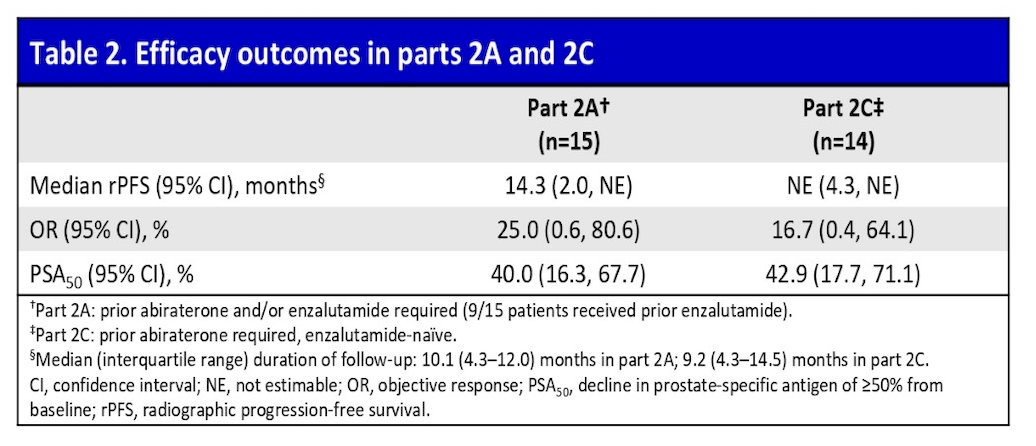
Confirmed PSA50 responses were seen in 40.0% of patients in cohort 2A and 42.9% in cohort 2C. Among patients with measurable disease at baseline, confirmed objective responses were observed in 25.0% of cohort 2A and 16.7% of cohort 2C, each including one partial response.
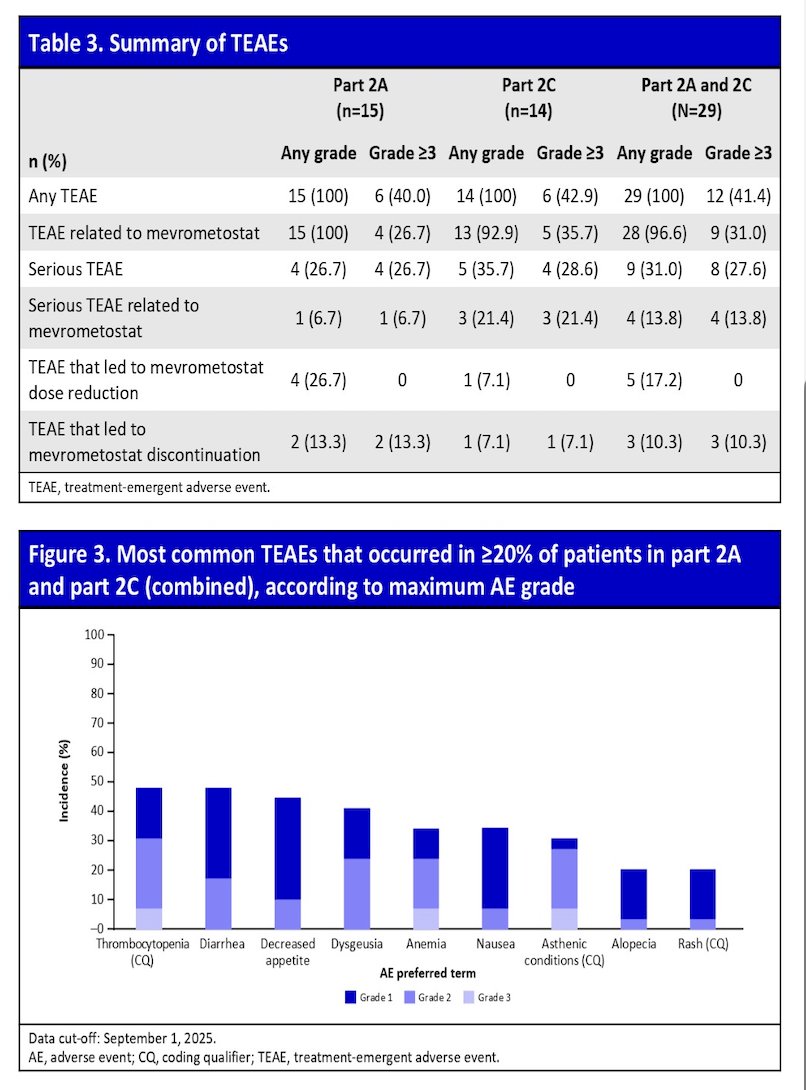
Across parts 2A and 2C combined, the most common treatment-related adverse events of any grade were diarrhea (44.8%) and thrombocytopenia (44.8%). Grade 2–3 treatment-related events occurred in 31.0% of patients and included two cases each of thrombocytopenia and anemia, and single cases of weight decrease, hypokalemia, abdominal discomfort, increased alanine aminotransferase, QT prolongation on electrocardiogram, hemorrhagic enterocolitis, hypocalcemia, and pneumonitis. Serious treatment-emergent adverse events were reported in 31.0% of patients, with 13% considered related to mevrometostat, including isolated cases of anemia, QT prolongation, hemorrhagic enterocolitis, and pneumonitis.
Dose reductions due to treatment-related adverse events occurred in 17.2% of patients and included dysgeusia (two cases) and single cases of asthenic conditions, nausea, thrombocytopenia, and urinary tract infection. Treatment discontinuation due to adverse events occurred in approximately 10% of patients, including isolated cases such as osteonecrosis of the jaw and pneumonitis. Importantly, there were no treatment-related deaths reported.
Dr. Matsubara highlighted the following points to summarize his presentation:
- M 875 mg twice daily with food plus enzalutamide demonstrated encouraging radiographic and PSA responses in previously treated mCRPC.
- Median rPFS was 14.3 months in cohort 2A and not yet reached in cohort 2C at the time of analysis.
- PSA50 responses were observed in approximately 40% of patients across both cohorts.
- The safety profile was manageable, with grade 3 or higher adverse events consistent with prior experience and no treatment-related deaths.
Presented by: Nobuaki Matsubara, MD, Department of Medical Oncology, National Cancer Center Hospital East, Kashiwa, Japan
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
Related content: EZH2 Inhibition Combined with ARPI Evaluated in Patients with Castration-Resistant Prostate Cancer - Nobuaki Matsubara