(UroToday.com) The 2026 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Amar Kishan discussing an individual patient data meta-analysis assessing hormone therapy use and duration with post-operative radiotherapy for recurrent prostate cancer.
Addition of hormonal therapy to definitive radiotherapy in localized prostate cancer improves overall survival. However, the effect of hormonal therapy on overall survival when added to postoperative radiotherapy after radical prostatectomy is less clear. Biochemical progression-based endpoints are consistently improved, but are not surrogates for overall survival and may simply reflect testosterone suppression itself. To date, there has been only one trial (RTOG 960)1 that has shown an overall survival benefit. Moreover, the study-level DADSPORT meta-analysis found no clear evidence of an overall survival benefit, with a non-significant estimated absolute effect of 2%.2 At ASCO GU 2026, Dr. Kishan and colleagues reported an individual patient data meta-analysis of randomized trials to quantify the benefit of adding hormonal therapy to postoperative radiotherapy.
The POSEIDON meta-analysis was an individual patient data meta-analysis of randomized phase 3 trials of postoperative radiotherapy ± hormonal therapy utilizing individual patient data from the MARCAP consortium. The primary outcome was overall survival. Meta-analyses evaluated the benefit of hormonal therapy to postoperative radiotherapy, the addition of short-term hormonal therapy (4-6 months), or the addition of long-term hormonal therapy (24 months) to postoperative radiotherapy. Tests for interaction based on pre-postoperative radiotherapy, PSA, and duration of hormonal therapy were evaluated, and non-linear associations between pre-postoperative radiotherapy, PSA, and overall survival were modeled with cubic splines.
Six phase 3 trials were eligible for inclusion in our analysis and had individual patient data available (6,057 patients, median follow-up of 9.02 years):

The addition of hormonal therapy to radiotherapy did not improve overall survival (HR 0.87, 95% CI 0.76-1.01, p = 0.06), but did improve metastasis-free survival (HR 0.79, 95% CI 0.70-0.89):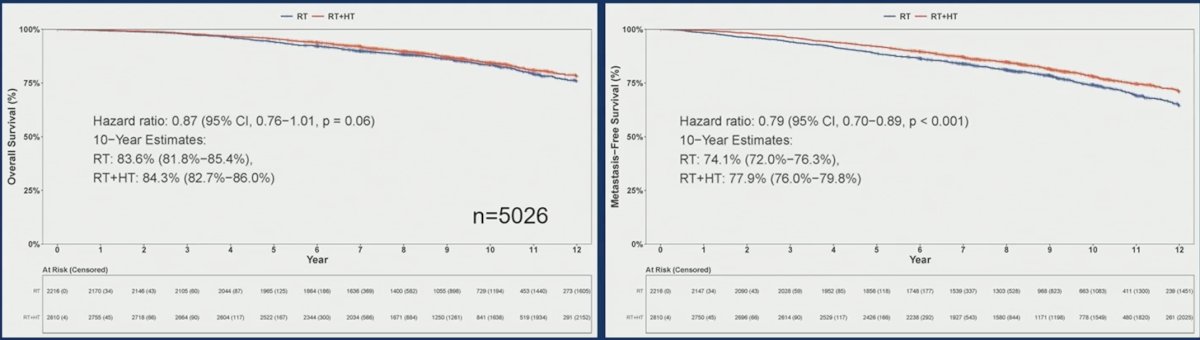
For hormone therapy duration and overall survival, short-term hormone therapy had a hazard ratio of 0.93 (95% CI 0.77-1.11), where has long term hormone therapy had a hazard ratio of 0.79 (95% CI 0.63 – 1.00):
There was no significant interaction between duration of hormonal therapy and this effect (p-interaction 0.25), though there was a significant interaction based on pre-postoperative radiotherapy PSA >0.5 ng/mL versus ≤0.5 ng/mL (p-interaction 0.02). For both overall survival and metastasis-free survival, the upper bound of the 95% CI of the hazard ratio for the addition of any hormonal therapy remains above 1 for all pre-radiotherapy PSAs, and for metastasis-free survival, the ICECAP surrogate threshold effect (0.81) was never crossed: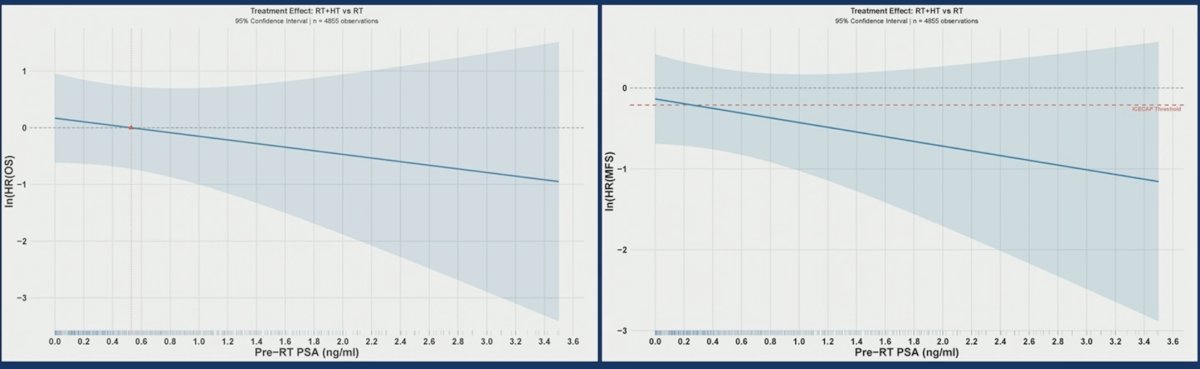
For patients randomized to ± long-term hormonal therapy (n = 1,088), the upper bounds of the 95% CI for overall survival fell below 1.0 at PSA >1.6 ng/mL and crossed 0.81 for metastasis-free survival at a pre-radiotherapy PSA of 2.1 ng/mL. This implies a significant overall and metastasis-free survival benefit may appear, but only at highly elevated PSAs (>1.6 ng/mL):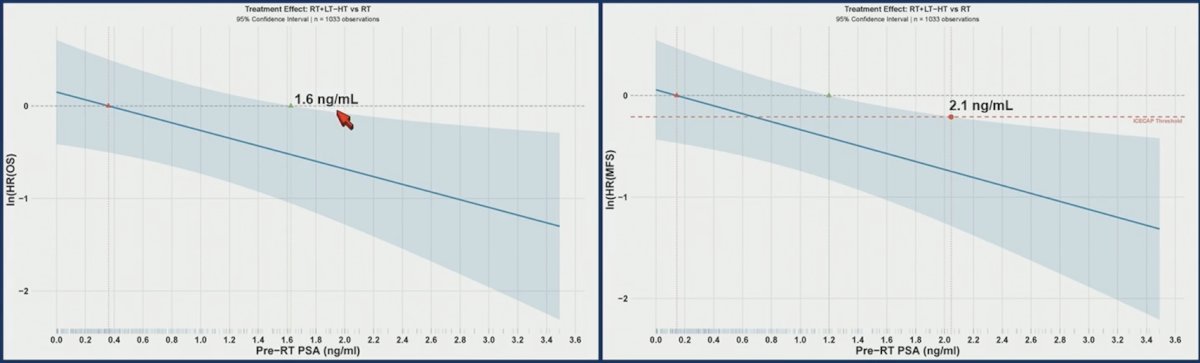
Dr. Kishan noted several limitations to this analysis, including (i) patients treated over a 17 year period (1998-2015), (ii) 70% of patients in the radiotherapy ± long term hormonal therapy cohort were on RTOG 9601, which used bicalutamide monotherapy (not ADT), (iii) improvement in earlier endpoints (ie. event free survival) by hormonal therapy may be of value to patients, even if the overall survival benefit is not robust, and (iv) enrollment predated the use of prognostic biomarkers (ie. Decipher) and advanced molecular imaging (ie. PSMA PET). Data from biomarker-driven trials such as NRG GU-006 will be highly informative.
Dr. Kishan concluded his presentation discussing an individual patient data meta-analysis assessing hormone therapy use and duration with post-operative radiotherapy for recurrent prostate cancer with the following take-home points:
- Who needs hormone therapy with post-operative radiotherapy? Only patients with a pre-post operative radiotherapy PSA > 0.5 ng/mL. This study found a significant interaction between hormone therapy effect and pre-postoperative radiotherapy PSA, and spline analyses overall showed no significant effect
- How long does hormone therapy with postoperative radiotherapy need to be? For most patients, short-term hormonal therapy is sufficient. There was no significant interaction between the hormone therapy effect and hormone therapy duration. An exploratory analyses suggests minimal benefit to hormone therapy prolongation
Presented by: Amar U. Kishan, MD, Professor, Executive Vice Chair of Clinical and Translational Research, Chief of the Genitourinary Oncology Service, Department of Radiation Oncology, University of California, Los Angeles (UCLA), Los Angeles, CA
Related content: POSEIDON Meta-Analysis Re-examines the Role of ADT with Salvage Radiation for Prostate Cancer - Amar Kishan
- Shipley WU, Seiferheld W, Lukka HR, et al. Radiation with or without Antiandrogen Therapy in Recurrent Prostate Cancer. N Engl J Med 2017;376(5):417-428.
- Burdett S, Fisher DJ, Tierney JF, et al. Duration of Androgen Suppression with Postoperative Radiotherapy (DADSPORT) for Nonmetastatic Prostate Cancer: A Collaborative Systematic Review and Meta-analysis of Aggregate Data. Eur Urol. 2025 Sep;88(3):277-290.