(UroToday.com) The 2026 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Andrew Laccetti discussing 52-week results from ARAMON assessing the efficacy and safety of darolutamide monotherapy in patients with castration sensitive prostate cancer after biochemical recurrence.
Darolutamide, an androgen receptor inhibitor, demonstrates low blood–brain barrier penetration, limited drug–drug interactions, robust efficacy across multiple disease settings, and a favorable safety profile, as reported in the phase 3 ARANOTE,1 ARAMIS,2 and ARASENS3 trials. The open-label, phase 2 ARAMON trial (NCT05526248) investigated the use of darolutamide monotherapy in patients with oligometastatic castration sensitive prostate cancer (CSPC) after biochemical recurrence. At ASCO GU 2026, Dr. Laccetti and colleagues reported the final lead-in outcomes at 52 weeks.
Eligible patients had confirmed CSPC, prior radical prostatectomy or radiotherapy, PSA ≥0.2 ng/mL after radical prostatectomy or ≥2 ng/mL after radiotherapy only, with a PSA doubling time ≤20 months, <5 asymptomatic metastatic lesions by conventional imaging and PSMA PET, serum testosterone >150 ng/dL, and an ECOG performance status score 0–1. Prior androgen deprivation therapy of ≤6 months was allowed if >6 months before the start of study treatment. Patients received darolutamide 600 mg twice daily for 52 weeks:

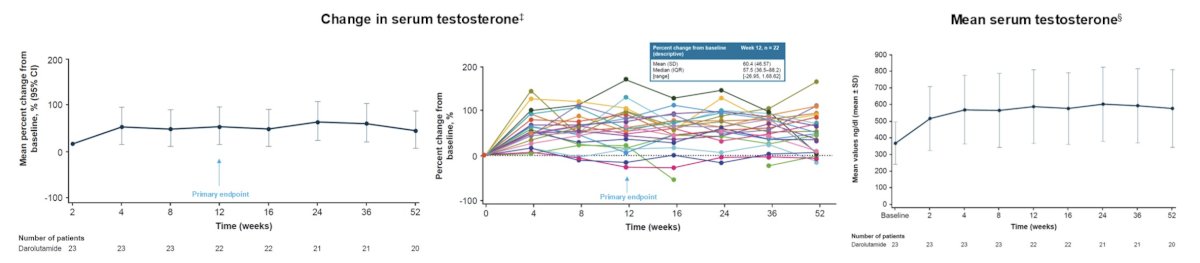
The primary endpoint was the change in serum testosterone from baseline to week 12 (secondary endpoint: change from baseline to weeks 24 and 52), and secondary endpoints were PSA response and safety. Exploratory endpoints included assessment of fat, glucose metabolism, bone turnover, changes in other sex hormones, and quality of life.
Of 23 eligible patients (evaluable set), the median age was 74 years (range 54–84), 61% were white, 91% had an ECOG performance status score 0, and 87% had a Gleason score <8. At study entry, median PSA was 6.0 ng/mL (range 2.1–27.4). From the start of darolutamide treatment, testosterone increased by 53% at week 12, 56% at week 24, and 48% at week 52. Mean serum testosterone concentrations increased through week 4 and then remained stable through week 52:
At week 52, deep PSA responses (PSA <0.2 ng/mL) were observed in 65% of patients, and 83% reached a 90% reduction in PSA: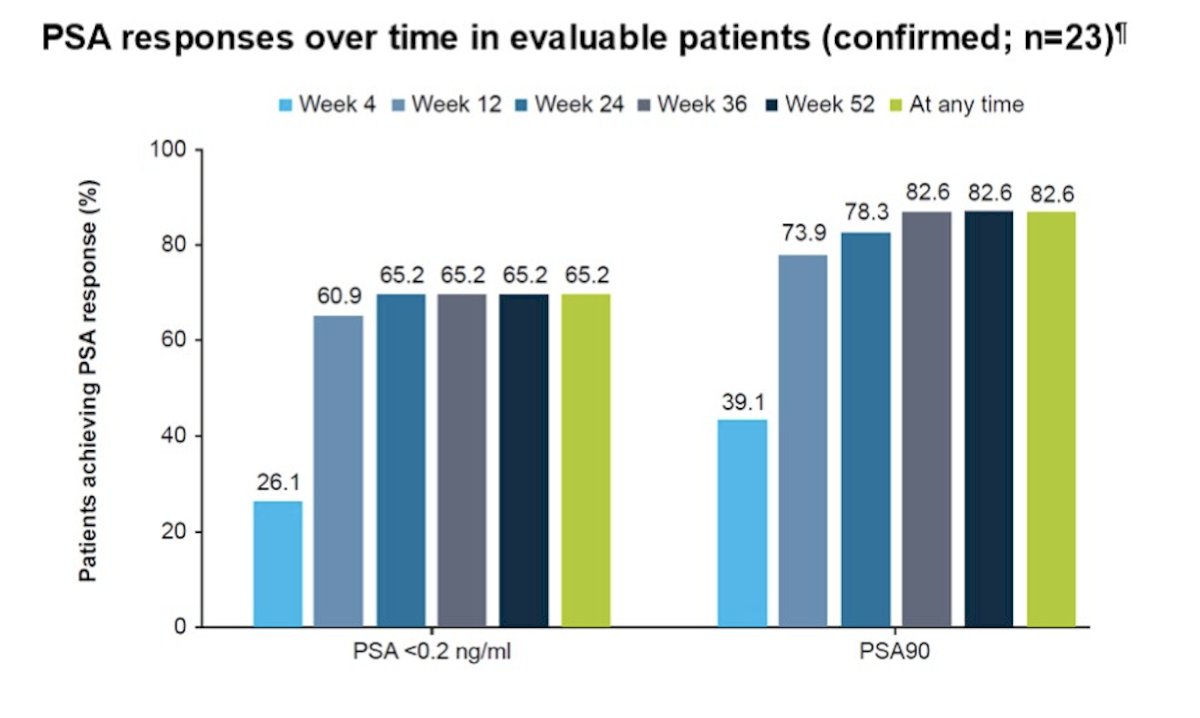
Minimal changes from baseline were observed over 52 weeks in measures of fat, glucose metabolism, bone turnover, and sex hormones (ie, luteinizing hormone, follicle-stimulating hormone, estradiol). Quality of life (per FACT-P total score) was maintained during the 52-week study:

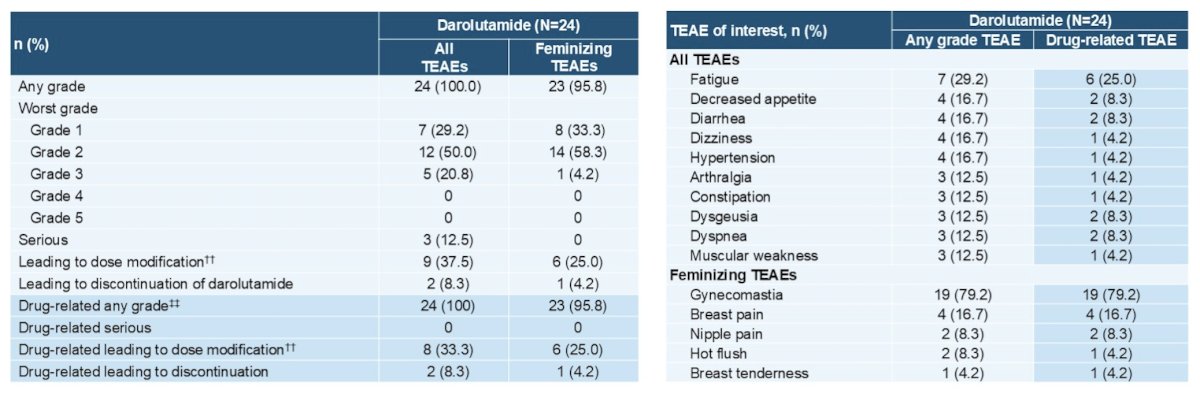
Darolutamide had a favorable safety profile with expected side effects for androgen receptor inhibitor monotherapy. Most treatment-emergent adverse events were grade 1 or 2, including feminizing treatment-emergent adverse events (gynecomastia, breast pain, hot flush, nipple pain, breast tenderness), which occurred mostly during the first 6 months of darolutamide:
Dr. Laccetti concluded his presentation discussing 52-week results from ARAMON with the following take-home points:
- In patients with CSPC after biochemical recurrence, darolutamide monotherapy moderately increased testosterone concentrations from baseline to week 12, which remained stable through week 52
- Deep PSA responses were observed, and the safety profile of darolutamide was consistent with known treatment-emergent adverse events of androgen receptor inhibitor monotherapy
Presented by: Andrew L. Laccetti, MD, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 26 – Sat, Feb 28, 2026.
References:
- Saad F, Vjaters E, Shore N, et al. Darolutamide in Combination with Androgen-Deprivation Therapy in Patients with Metastatic Hormone-Sensitive Prostate Cancer From the Phase III ARANOTE Trial. J Clin Oncol. 2024 Dec 20;42(36):4271-4281.
- Fizazi K, Shore N, Tammela TL, et al. Darolutamide in nonmetastatic castration-resistant prostate cancer. N Engl J Med. 2019;380(13):1235-1246.
- Smith MR, Hussain M, Saad F, et al. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med. 2022 Mar 24;386(12):1132-1142.