(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026, was host to the session Treatment Selection, Response Assessment, and Monitoring Across the Spectrum of Advanced Prostate Cancer. Dr. Andrew Armstrong discussed the Evaluation and Definition of Response and Progression from Trials to Clinical Practice.
Dr. Armstrong presented the case of a 57-year-old man with de novo mHSPC, harboring 7 bone metastases and T4N1 disease, with an initial PSA of 750 ng/mL. He was treated with triplet therapy (ADT, darolutamide, and docetaxel), achieving a PSA nadir of 0.1 at 12 months with radiographic improvement in nodal disease and stable bone findings, and continued on ADT plus ARPI. At 24 months, despite a persistently low PSA of 0.1, he developed upper neck pain and was found on MRI to have a large cervical soft tissue mass with epidural involvement. Surgical resection confirmed treatment-emergent small cell neuroendocrine prostate cancer (t-NEPC). NGS demonstrated TMPRSS2-ERG fusion, PTEN loss, and TP53 mutation. He was subsequently started on platinum-based doublet chemotherapy, underscoring the risk of lineage plasticity and aggressive transformation despite biochemical control.
Dr. Armstrong reviewed the foundational role of the Prostate Cancer Working Groups (PCWG), established nearly 30 years ago to standardize clinical trial design and interpretation in advanced prostate cancer. Beginning with the original PSA Working Group in 1999, these efforts defined consensus criteria for PSA response and progression, clarified the castration state, and formalized evolving disease states. PCWG2 (2008) and PCWG3 (2016) further refined eligibility and progression criteria, recognizing phenomena such as bone scan flare and discordance between PSA and imaging. The introduction of the “2+2” rule for radiographic progression helped prevent premature treatment discontinuation and enabled the successful development of ARPIs by ensuring therapy was not stopped based on unconfirmed early bone changes.
Dr. Armstrong emphasized that updated trial guidelines are needed to reflect the rapidly evolving therapeutic landscape. Over the past decade, multiple agents with distinct mechanisms, ARPIs, PARP inhibitors, precision therapies, PSMA radioligand therapy, and radium-223 have been approved and increasingly moved into earlier, hormone-sensitive settings. At the same time, PSMA PET imaging is now widely used to diagnose, stage, and monitor disease, yet standardized guidance on its incorporation into trial design remains limited. There is also a growing need for a more patient-centric disease state model that does not presuppose outcomes, along with harmonized endpoints applicable to earlier disease stages. Finally, as treatment decisions become increasingly biomarker-driven, trial frameworks must better integrate evolving tumor and patient genotypes and phenotypes in alignment with regulatory guidance and more robust evidence-based biomarker development.
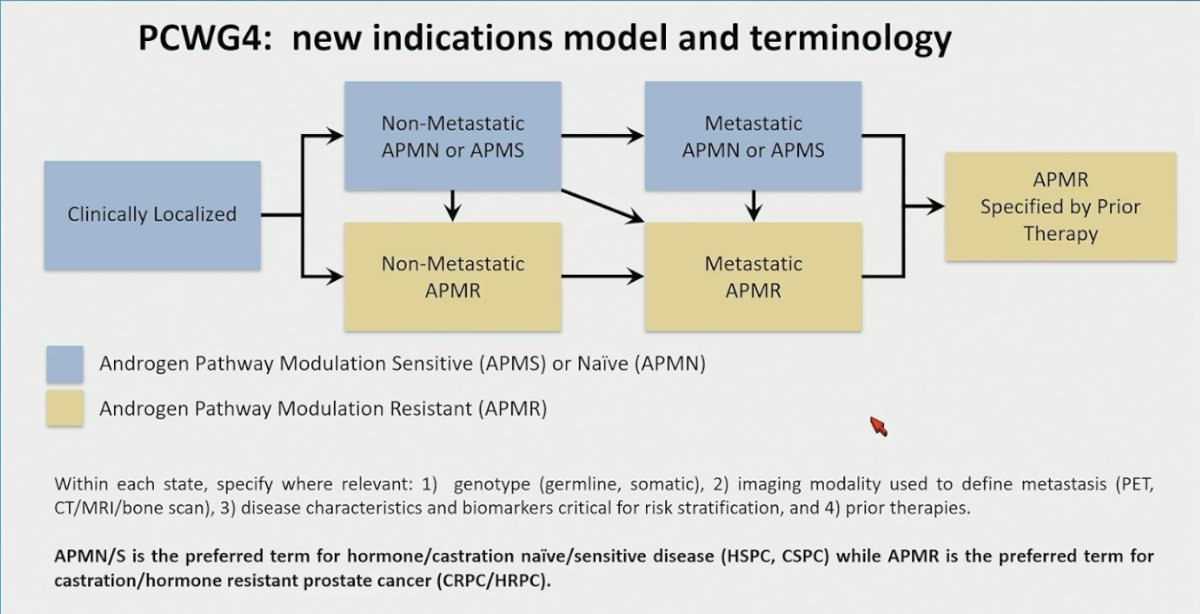
PCWG4 proposes an updated disease state model and terminology that reflects the widespread use of ARPIs and other modern therapies. Rather than relying solely on traditional “hormone-sensitive” and “castration-resistant” labels, the framework introduces androgen pathway modulation–naïve or sensitive (APMN/APMS) and androgen pathway modulation–resistant (APMR) states, applicable to both non-metastatic and metastatic disease. This nomenclature aims to be more biologically and treatment-informed, accounting for prior therapy exposure, imaging modality used to define metastases, and relevant genomic and biomarker features. In this model, APMN/APMS corresponds to hormone/castration-naïve or -sensitive disease, whereas APMR aligns with castration-resistant prostate cancer, providing a more precise and contemporary structure for clinical trial design and reporting.
Endpoints matter because they determine how therapies are approved, how trials are designed, how clinicians counsel patients, and how health systems allocate resources. Regulatory bodies rely on primary endpoints such as OS or PFS to grant approval and reimbursement. From a trial design perspective, endpoints define sample size, duration, and feasibility, influencing decisions to move from phase 2 to phase 3. Clinically, endpoints shape conversations with patients by translating data into meaningful expectations about survival, disease control, and quality of life. Without validated intermediate endpoints, it becomes difficult to explain benefit, compare options, or guide treatment decisions in real time. At a systems level, endpoints inform cost-effectiveness analyses and coverage decisions, integrating survival and quality-of-life outcomes into policy.
Moreover, he went on to discuss response endpoints and emphasized that their value is highly context dependent. PSA declines, and nadirs are inexpensive, rapid, and strongly prognostic, yet they are not validated surrogates for survival and may be discordant with imaging. Similarly, ctDNA and CTC responses allow for non-invasive, dynamic assessment of tumor burden and are often highly prognostic, but they require assay standardization and validation and are not yet broadly accepted as surrogate endpoints for approval. These measures can complement traditional imaging endpoints, but their interpretation must consider disease state, treatment mechanism, and clinical setting.
He highlighted that most regulatory approvals in prostate cancer have been driven by hard clinical endpoints such as overall survival, radiographic progression-free survival, delay in metastasis, or symptom improvement. OS has supported approval for multiple agents, including taxanes, ARPIs, PARP inhibitors in selected populations, and LuPSMA. Metastasis-free survival and rPFS have also led to approvals or label expansions in earlier disease settings. Patient-reported outcomes and symptom improvement supported earlier approvals in the 1990s. In contrast, PSA declines, CTC changes, or ctDNA responses, while prognostic and clinically informative, have not independently led to regulatory approvals to date, as illustrated below.
Dr. Armstrong emphasized that PCWG4 provides structured guidance on incorporating non-imaging response endpoints into modern trial design. These measures can support early go/no-go decisions and accelerate development timelines, particularly in earlier-phase studies. However, no single endpoint guarantees success, and none are validated surrogates for overall survival. PCWG4 encourages the thoughtful integration of multiple measures, including CTC conversion, ctDNA reduction or normalization where appropriate, PSA declines and nadir, and patient-reported outcomes such as pain and global quality-of-life assessments, interpreted within the clinical context. The framework also recognizes the value of normalizing adverse prognostic laboratory markers such as ALP, LDH, hemoglobin, and albumin, while reinforcing that these signals must ultimately be linked to meaningful long-term outcomes
He highlighted multiple studies demonstrating that PSA declines and CTC reductions are strongly prognostic across disease states. In both mCRPC and mHSPC, achieving deep PSA responses or CTC conversion to zero is consistently associated with improved overall survival, as shown in analyses from ARCHES, CHAARTED, and other cohorts. While these markers are not validated surrogates for OS, identifying and incorporating such prognostic factors into trial design can improve risk stratification, enrich study populations, and enhance interpretation of early treatment signals.
He further noted that ctDNA content is also strongly prognostic. Across multiple studies in mCRPC, higher baseline ctDNA fraction and dynamic changes over time consistently correlate with worse overall and progression-free survival, independent of other clinical factors. Quantitative ctDNA levels can stratify patients into distinct risk groups and may enhance prognostic modeling when combined with clinical variables. While not yet a validated surrogate endpoint, ctDNA provides a powerful, minimally invasive biomarker that can inform trial enrichment and risk-adapted study design.
While overall survival remains the gold standard endpoint, he emphasized that other delay or prevention endpoints are increasingly important in modern trial design. Radiographic PFS provides earlier readouts and has supported regulatory approvals, though it does not always translate into OS or quality-of-life benefit. Clinical PFS captures symptomatic progression and meaningful clinical events beyond imaging, but definitions vary across studies. Metastasis-free survival has emerged as a validated endpoint in certain earlier disease settings, particularly in the adjuvant space. Together, these endpoints complement OS and reflect a broader, more nuanced assessment of treatment benefit in contemporary prostate cancer care.
He highlighted emerging meta-analytic data in mHSPC demonstrating a strong correlation between rPFS, cPFS, and overall survival. Trial-level analyses show that improvements in 3-year rPFS rates closely track with 5-year OS outcomes, with correlation coefficients in the 0.8 range, suggesting these endpoints may function as promising surrogates in the androgen pathway modulation–sensitive setting. Both rPFS and cPFS demonstrated robust associations with OS across multiple studies, supporting their potential use as earlier efficacy endpoints when overall survival data require prolonged follow-up.
He highlighted a clear disconnect between PSA progression and radiographic progression across phase III ARPI trials such as ARCHES, ENZAMET, and TITAN. A substantial proportion of patients experienced radiographic progression without a concomitant PSA rise, reflecting potential lineage plasticity and loss of PSA as a reliable disease marker in some cases. Discordant progression was common and carried a similarly poor prognosis compared with concordant progression. These findings underscore the need for routine imaging and the integration of additional biomarkers beyond PSA to more accurately monitor disease evolution in the modern treatment era.2-4
Dr. Armstrong reviewed key imaging principles carried forward from PCWG2 and PCWG3 into PCWG4. Imaging endpoints should remain simple, globally feasible, and avoid reliance on proprietary software models that may become obsolete. Importantly, imaging-based endpoints are considered candidates until clinically validated, and radiographic progression as a regulatory endpoint does not necessarily mean loss of treatment benefit. He revisited the 2+2 rule for bone scans, which requires confirmation of new lesions to distinguish true progression from flare. PCWG4 proposes refinement of the confirmatory scan approach, including the 2+0 rule (Shown below), while acknowledging the concern that mandatory confirmation may delay recognition of ineffective therapy in some patients.
In PCWG4, the “Rule of 5” was introduced to refine the interpretation of new bone lesions on imaging. If five or fewer new metastases are detected, the prior PCWG3 confirmation approach applies, requiring a follow-up scan to confirm progression. However, if more than five new lesions are identified, this is considered sufficient evidence of progression without the need for confirmatory imaging (see below). This modification aims to balance the need to avoid misclassifying flare as progression while reducing delays in recognizing clear disease progression.
Dr. Armstrong noted that PCWG4 formally incorporates PSMA PET into response assessment. If PSMA PET is performed before 8 weeks, findings are considered non-actionable. At 8 weeks or later, new lesions can be taken at face value as evidence of progression. Changes in disease volume or SUV parameters are considered investigational and should be collected, but there are no formal partial or progressive response definitions based solely on SUV or volume; complete responses may be reported. For now, new lesions remain the primary bridge for defining progression, with RECIST criteria still applying to the CT component of PSMA PET/CT imaging.
He also addressed what constitutes a new lesion on PSMA PET. Similar to PCWG2 and 3, there is no single strict definition. Instead, high reader confidence is recommended, based on a combination of factors such as intensity of PSMA uptake, correlation with cross-sectional imaging, and the overall pattern of spread, recognizing that even registration trials have lacked a uniform consensus definition.
Dr. Armstrong clarified that the Rule of 5 also applies to PSMA PET for bone, nodal, and pulmonary metastases. If five or fewer new lesions are identified, confirmation on a subsequent scan is required; if six or more new lesions are present, this constitutes progression. These findings should be reported separately from conventional bone scan and CT results, and their treatment implications remain investigational until further validated. Importantly, the Rule of 5 does not apply to liver or other non-pulmonary visceral metastases, where any single new lesion in the liver, adrenal gland, or other non-pulmonary visceral site is considered progression.
Dr. Armstrong concluded his presentation with the following key takeaways:
- PCWG4 provides updated guidance on endpoints for clinical trials, regulatory decision-making, and clinical practice in the modern treatment era.
- Intermediate delay/prevent endpoints, such as radiographic PFS and metastasis-free survival, may capture meaningful patient benefit beyond overall survival.
- PSMA-based response and delay/prevent endpoints have been proposed, but require prospective validation in ongoing trials.
- Response-based endpoints, including PSA decline or nadir, CTC or ctDNA conversion, pathologic response, and radiographic response, can serve as early efficacy signals when responses are confirmed and durable.
- Radiographic progression may occur without PSA rise, particularly on ARPI therapy, requiring continued imaging vigilance.
- Implementation of PCWG4 recommendations aims to accelerate therapeutic development and support more personalized treatment strategies that maximize survival and quality of life for patients most likely to benefit.
Presented by: Andrew Armstrong, MD, MSc, Medical Oncologist, Professor of Medicine, Surgery, Pharmacology and Cancer Biology, Director of the Urologic Research, Duke Cancer Institute, Center for Prostate and Urologic Cancers, Durham, NC
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
References:
- Sweeney CJ, Chen YH, Carducci M, Liu G, Jarrard DF, Eisenberger M, Wong YN, Hahn N, Kohli M, Cooney MM, Dreicer R, Vogelzang NJ, Picus J, Shevrin D, Hussain M, Garcia JA, DiPaola RS. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. N Engl J Med. 2015 Aug 20;373(8):737-46. doi: 10.1056/NEJMoa1503747. Epub 2015 Aug 5. PMID: 26244877; PMCID: PMC4562797.
- Armstrong AJ, Szmulewitz RZ, Petrylak DP, Holzbeierlein J, Villers A, Azad A, Alcaraz A, Alekseev B, Iguchi T, Shore ND, Rosbrook B, Sugg J, Baron B, Chen L, Stenzl A. ARCHES: A Randomized, Phase III Study of Androgen Deprivation Therapy With Enzalutamide or Placebo in Men With Metastatic Hormone-Sensitive Prostate Cancer. J Clin Oncol. 2019 Nov 10;37(32):2974-2986. doi: 10.1200/JCO.19.00799. Epub 2019 Jul 22. PMID: 31329516; PMCID: PMC6839905.
- Sweeney CJ, Martin AJ, Stockler MR, Begbie S, Cheung L, Chi KN, Chowdhury S, Frydenberg M, Horvath LG, Joshua AM, Lawrence NJ, Marx G, McCaffrey J, McDermott R, McJannett M, North SA, Parnis F, Parulekar W, Pook DW, Reaume MN, Sandhu SK, Tan A, Tan TH, Thomson A, Vera-Badillo F, Williams SG, Winter D, Yip S, Zhang AY, Zielinski RR, Davis ID; ENZAMET trial investigators and Australian and New Zealand Urogenital and Prostate Cancer Trials Group. Testosterone suppression plus enzalutamide versus testosterone suppression plus standard antiandrogen therapy for metastatic hormone-sensitive prostate cancer (ENZAMET): an international, open-label, randomised, phase 3 trial. Lancet Oncol. 2023 Apr;24(4):323-334. doi: 10.1016/S1470-2045(23)00063-3. PMID: 36990608.
- Chi KN, Chowdhury S, Bjartell A, Chung BH, Pereira de Santana Gomes AJ, Given R, Juárez A, Merseburger AS, Özgüroğlu M, Uemura H, Ye D, Brookman-May S, Mundle SD, McCarthy SA, Larsen JS, Sun W, Bevans KB, Zhang K, Bandyopadhyay N, Agarwal N. Apalutamide in Patients With Metastatic Castration-Sensitive Prostate Cancer: Final Survival Analysis of the Randomized, Double-Blind, Phase III TITAN Study. J Clin Oncol. 2021 Jul 10;39(20):2294-2303. doi: 10.1200/JCO.20.03488. Epub 2021 Apr 29. PMID: 33914595.