(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, was host to the Poster Session A: Prostate Cancer. Dr. Arun Azad presented Poster 177: Saruparib + ARPI + ADT in patients with mHSPC: The phase 1/2 PETRANHA trial.
Dr. Azad began by noting that combinations of poly(ADP-ribose) polymerase inhibitors (PARPi) with ARPI and ADT have improved outcomes in metastatic castration-resistant prostate cancer, particularly in patients with BRCA mutations. Saruparib is a selective PARP1 inhibitor, and interim results from PETRANHA previously demonstrated high rates of undetectable PSA (uPSA) in mHSPC regardless of homologous recombination repair mutation (HRRm) status.1 The current analysis provides updated efficacy and safety data.
In this study, patients received oral saruparib 60 mg once daily combined with physician’s choice of ARPI (enzalutamide, abiraterone acetate, or darolutamide) plus ADT. Up to six months of prior ADT was permitted. Prior chemotherapy for metastatic prostate cancer was not allowed. Treatment continued until disease progression or intolerable toxicity. The study design is shown below.

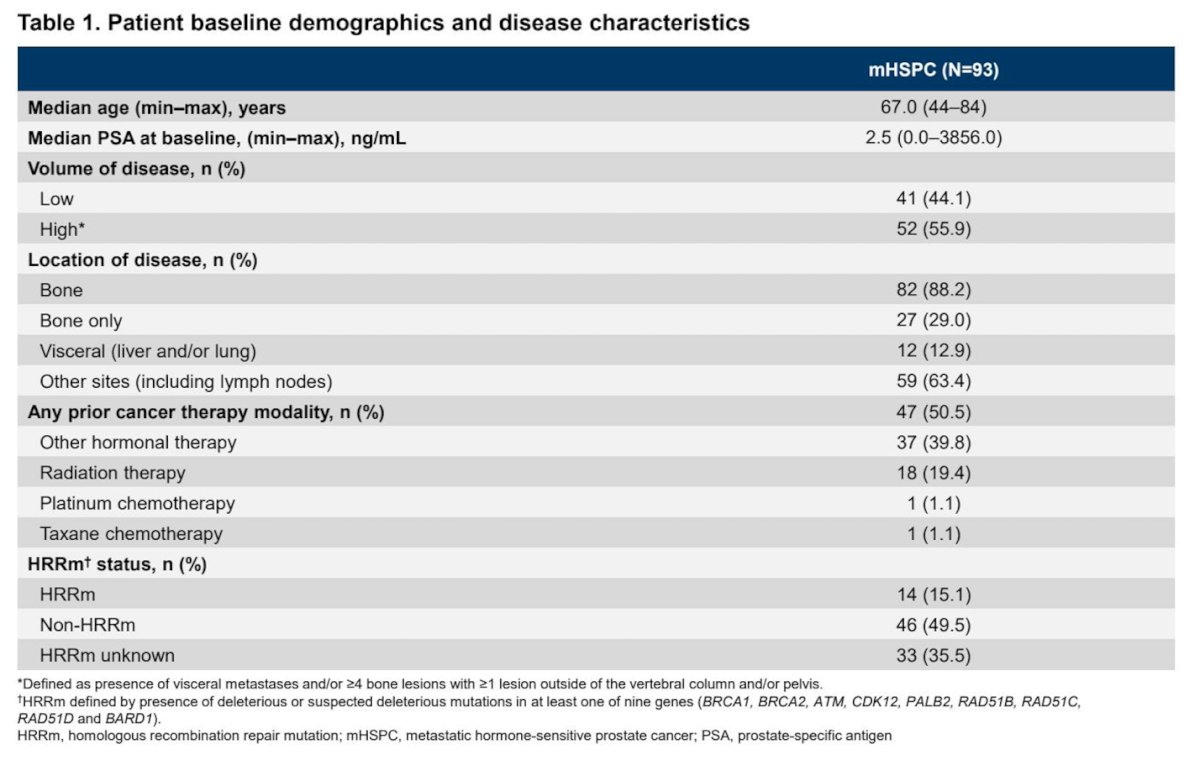
At the June 10, 2025, data cutoff, 93 patients with mHSPC had been treated. Most patients received darolutamide (n=76), with smaller numbers receiving abiraterone acetate (n=14) or enzalutamide (n=3). The median follow-up was 16.4 months. High-volume disease was present in 55.9% of patients, and 12.9% had visceral metastases. The baseline median PSA was 2.5 ng/mL, as illustrated in the table below.
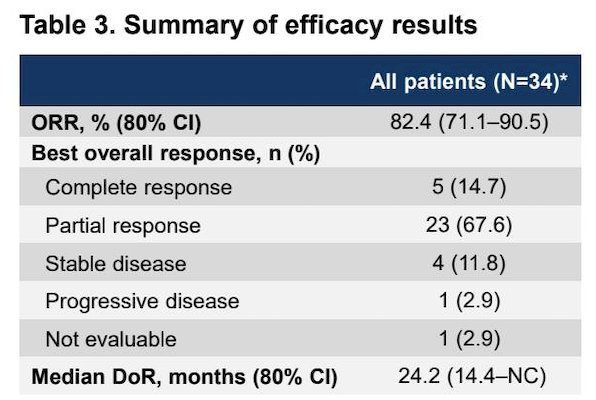
Among response-evaluable patients (34 of 93), the objective response rate (ORR) was 82.4%, including 14.7% complete responses. The confirmed uPSA rate at any time was 69.9%, and the confirmed 52-week uPSA rate was 76.7%.
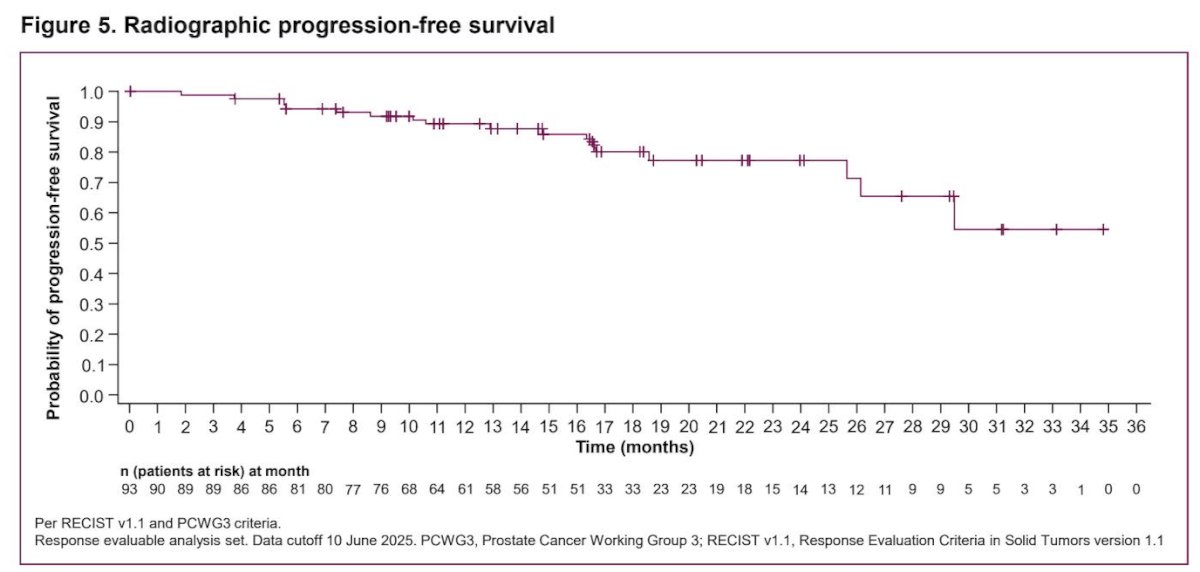
Dr. Azad reported that at a median follow-up of 16.4 months (range 0.0–34.8), the median radiographic progression-free survival had not been reached, with an 80% confidence interval of 29.5 months to not calculable.
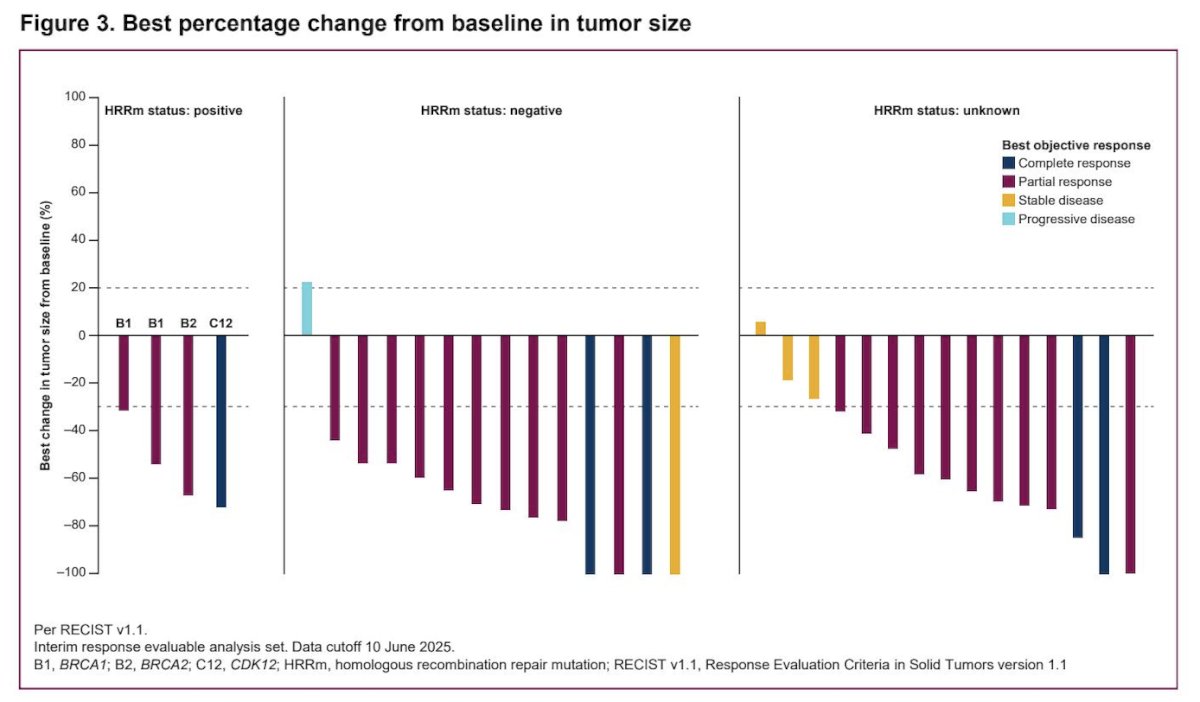
Importantly, efficacy was observed irrespective of HRRm status. Among patients with HRRm, the ORR was 100% compared to 85.7% in non-HRRm patients. Confirmed uPSA rates at any time were 71.4% in HRRm and 70.6% in non-HRRm patients. Confirmed 52-week uPSA rates were 77.8% and 73.9%, respectively.

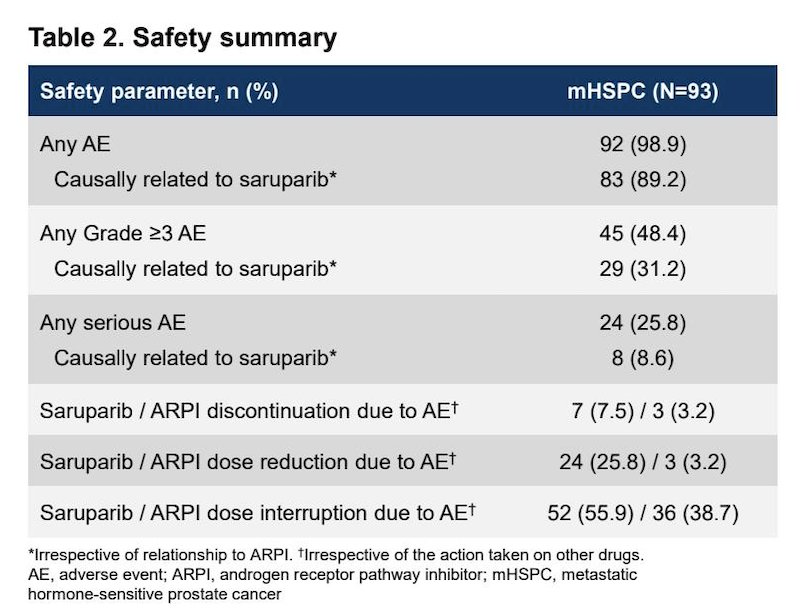
The combination demonstrated a manageable safety profile. Among 93 treated patients, nearly all experienced an adverse event, with Grade 3 or higher adverse events occurring in 48.4% of patients. Serious adverse events were reported in 25.8%, and treatment discontinuation due to adverse events occurred in 7.5% for saruparib and 3.2% for ARPI. No new safety signals were identified.
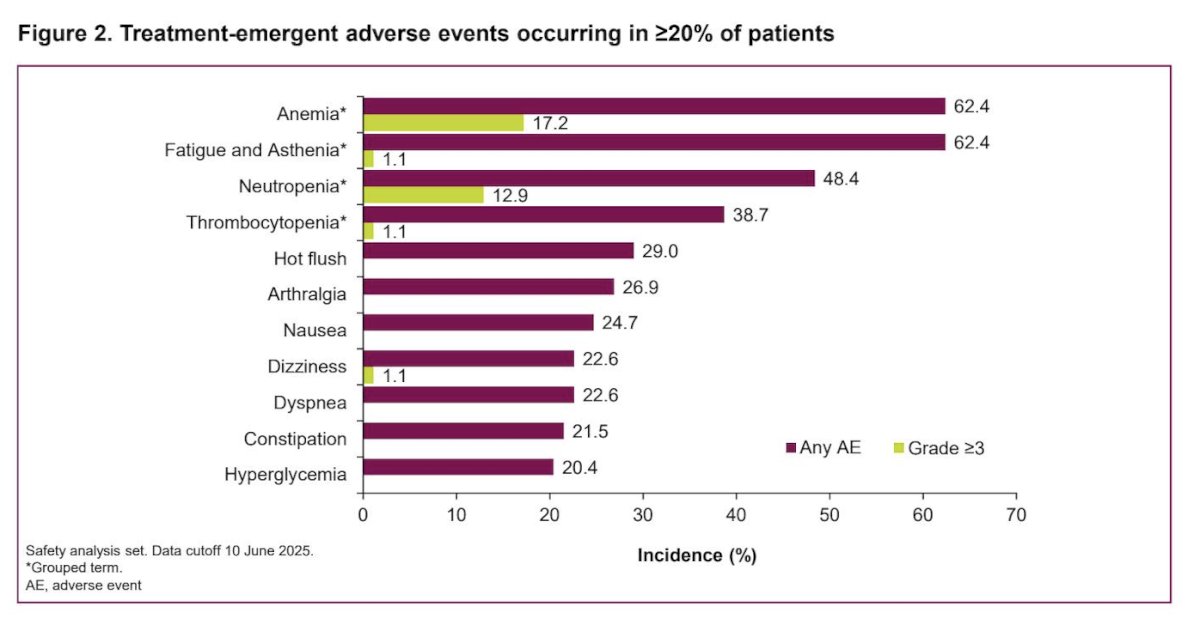
The most frequent treatment AEs were anemia, fatigue, asthenia, and neutropenia, as shown in the graphic below.
Dr. Azad concluded his presentation with the following key takeaways:
- Saruparib combined with ARPI and ADT induced high objective response rates and high rates of sustained undetectable PSA in patients with mHSPC.
- Clinical activity was observed regardless of homologous recombination repair mutation status.
- The safety profile of the triplet combination was manageable and consistent with known toxicities of the individual agents.
- These results support further evaluation in the ongoing Phase 3 EvoPAR-Prostate01 trial.
Presented by: Arun Azad, PhD, MBBS, FRACP, Professor, Department of Medicine, Peter MacCallum Cancer Centre, Melbourne, Victoria, Australia
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
Related content: Selective PARP1 Inhibition Combined with ARPIs Under Investigation in the PETRANHA in mHSPC - Arun Azad
- Arun Azad et al. PETRANHA: Phase 1/2 study of AZD5305 + novel hormonal agents in patients with metastatic prostate cancer-Interim safety and pharmacokinetic results.. J Clin Oncol 42, 123-123(2024). DOI:10.1200/JCO.2024.42.4_suppl.123